70 y.o. female former smoker (quit 20 years ago) with hx of COPD, recurrent steroid responsive hypoxic respiratory failure, hypersensitivity pneumonitis, HTN, breast cancer (, s/p left mastectomy 5years ago), thrombocytosis (on hydrea), arthritis, s/p multiple spinal surgeries, TKA b/l who presents today for new patient evaluation ?ILD.
Animals/birds/agriculture: had a pet bird for 7 years which was removed from the household a month ago, has 2 dogs.
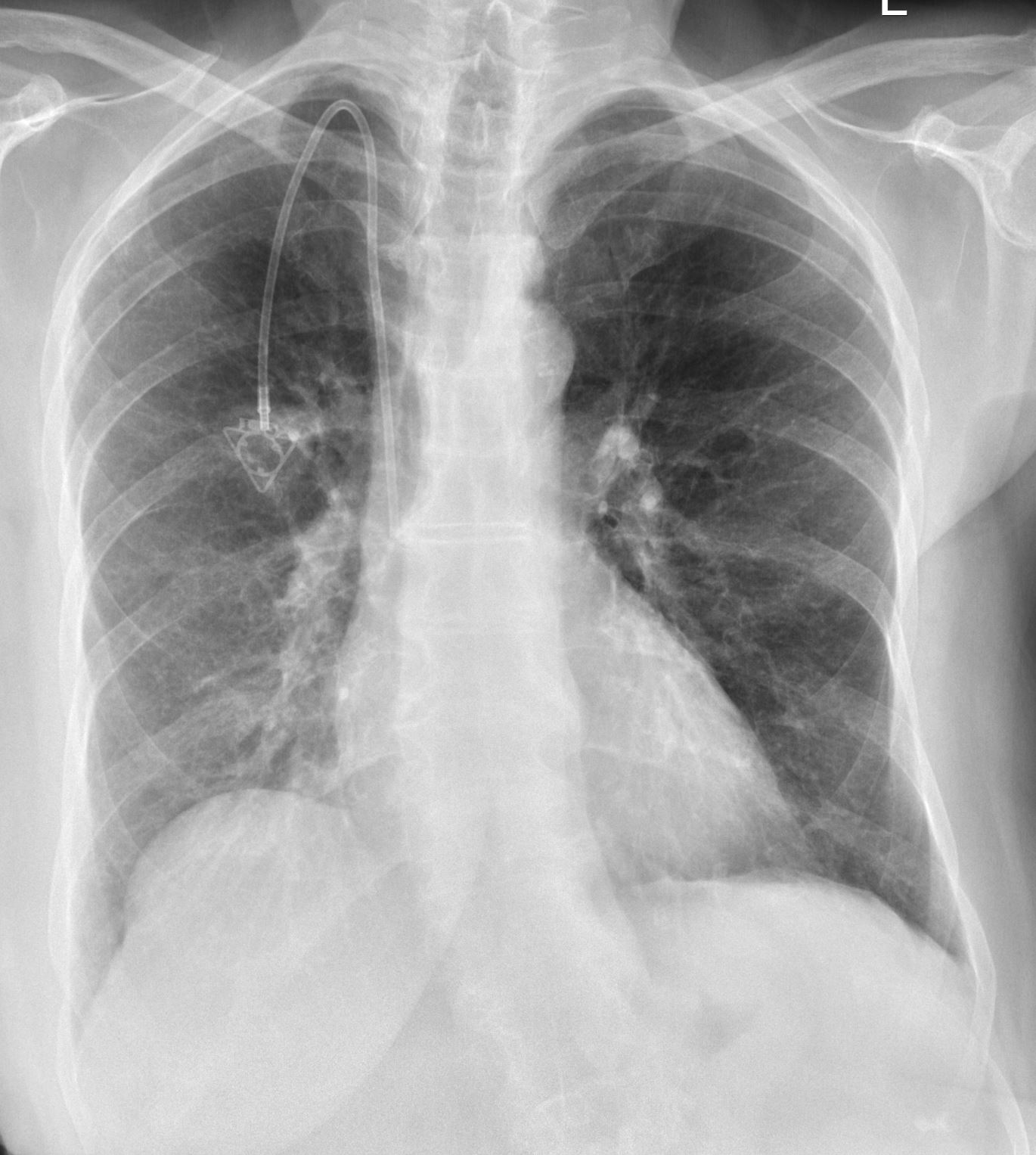
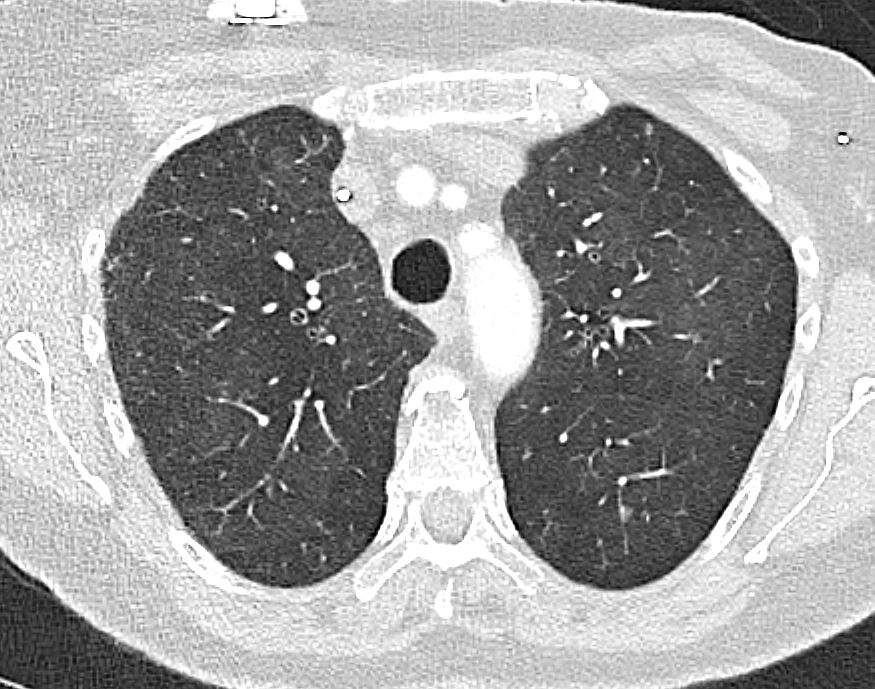


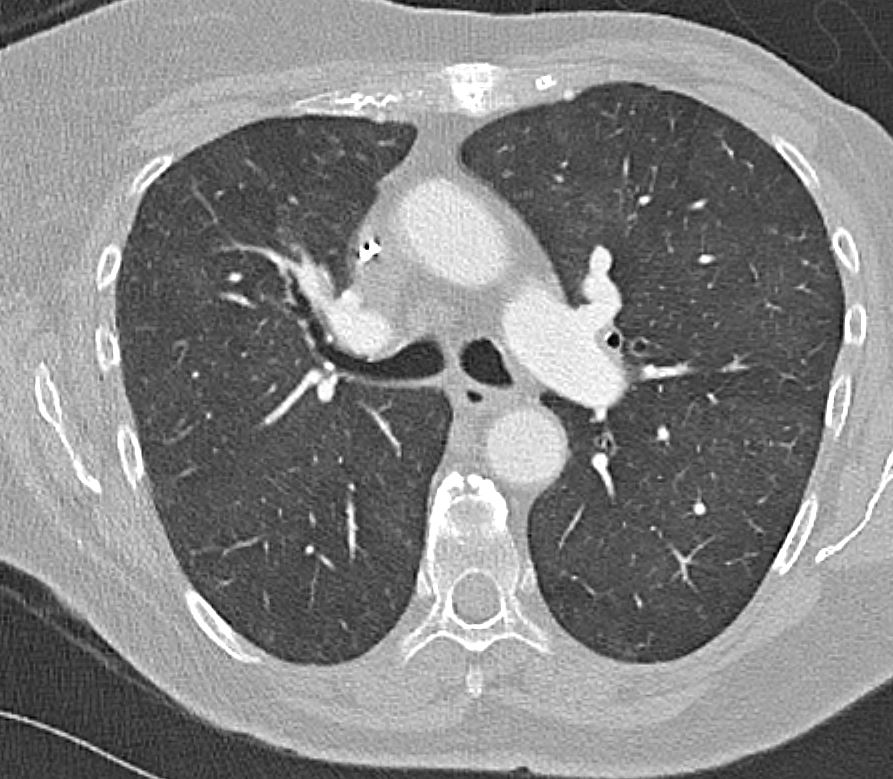

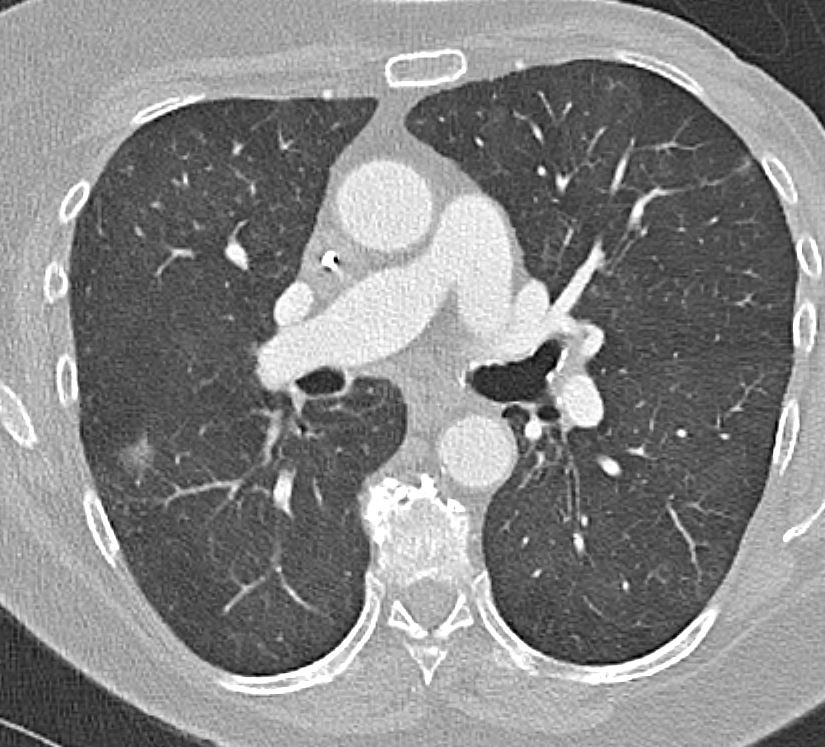
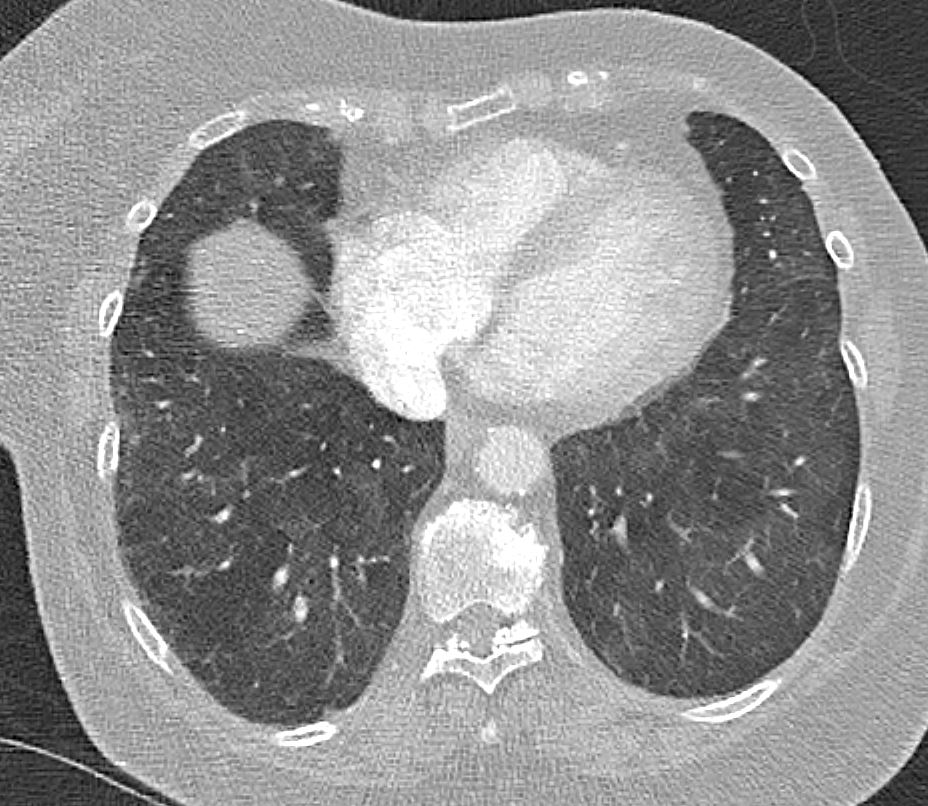
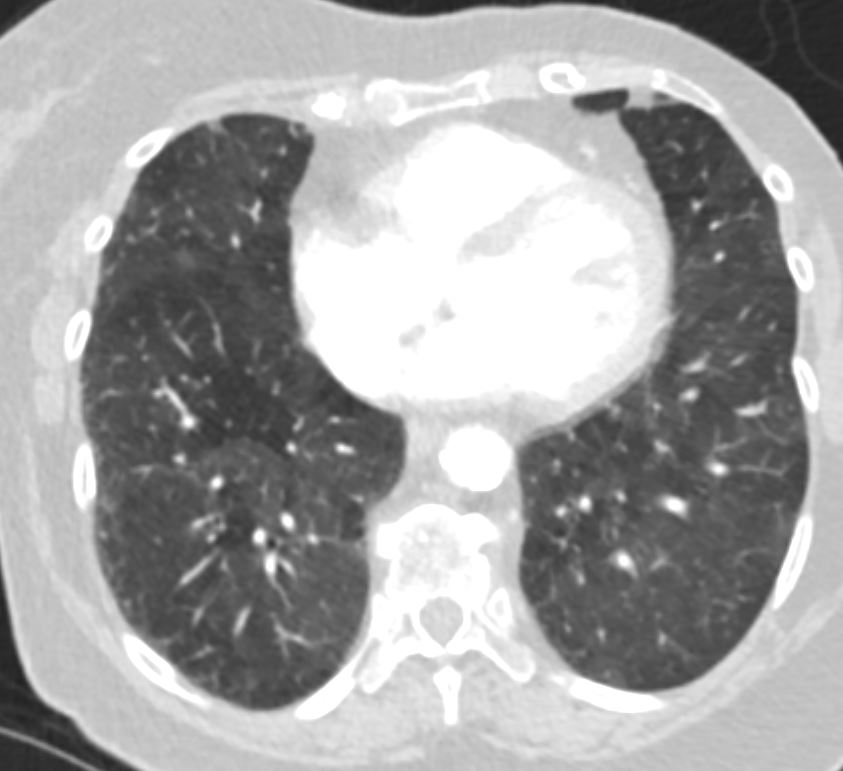

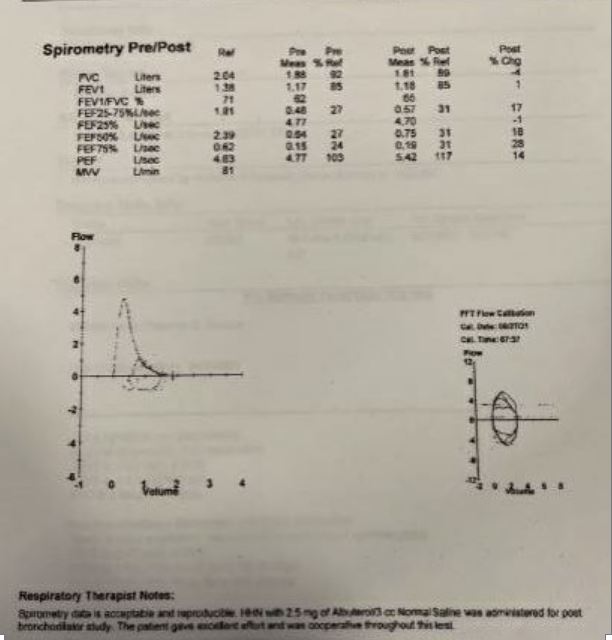
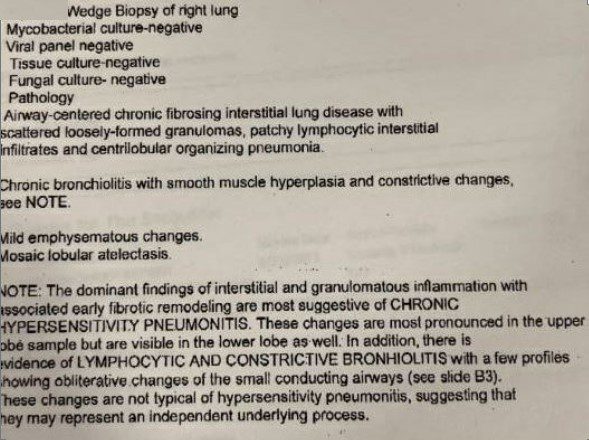
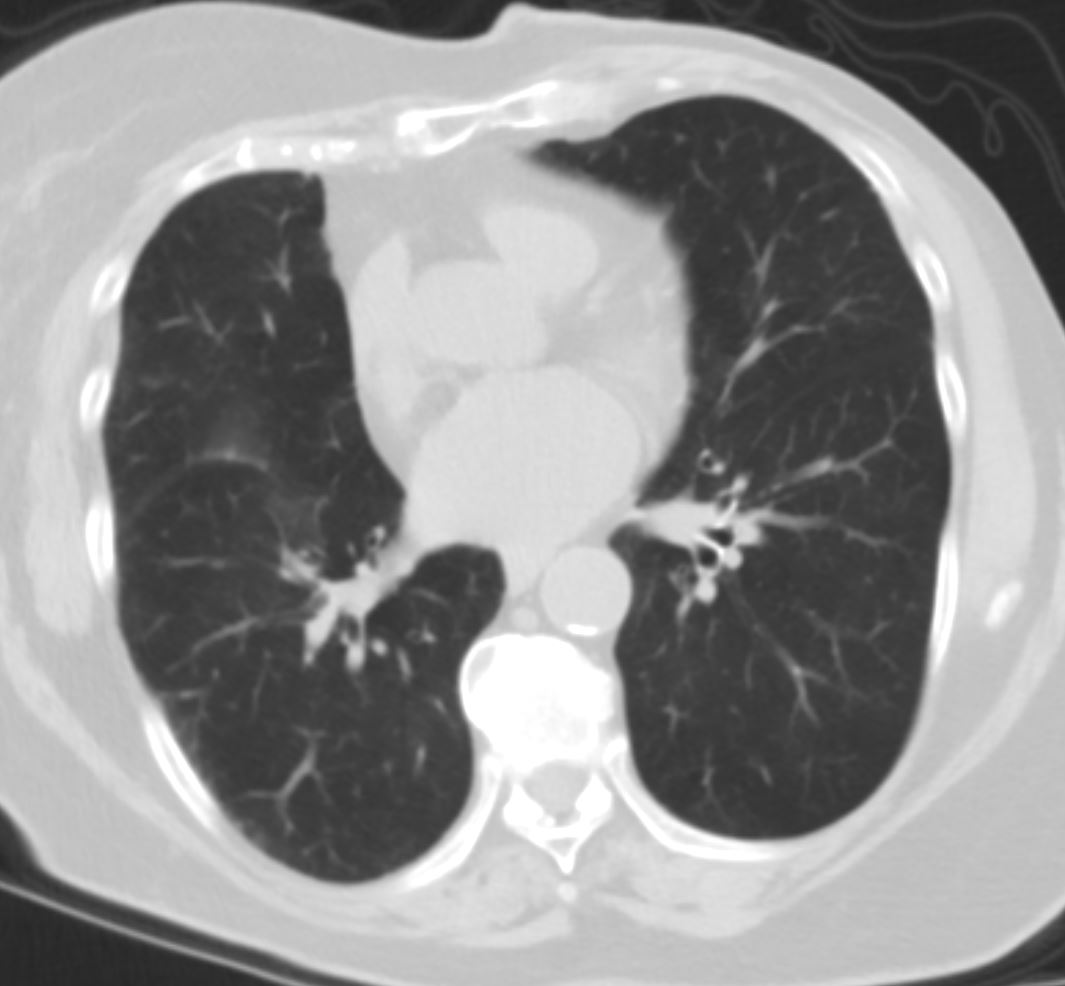
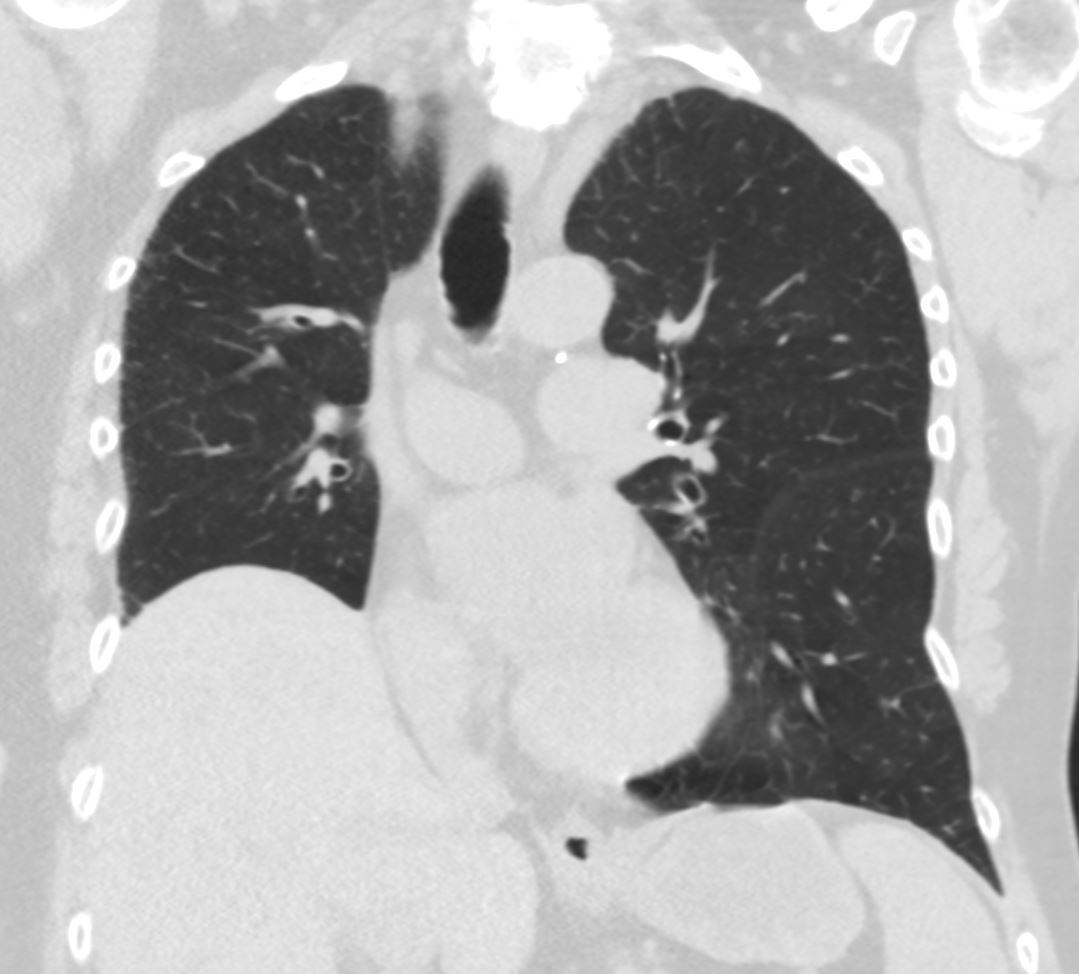
Pt with 11 month hx of DOE and hypoxic respiratory failure. She reports 3 hospitalizations with short lived improvement after short course of steroids followed by recurrence of symptoms after coming off steroids. She is currently on a prolonged steroid taper, she was started on 0.5 mg/kg prednisone in September, but so far reports little improvement. She has been following with a community pulmonologist who has initiated excellent work up and she presents now to BMC for secondary review of her pathology to help determine ultimate diagnosis and potential treatment options. Her most recent CT chest reveals diffuse GGOs with scattered nodularity. Pathology from a VATs wedge biopsy notable for fibrotic remodeling most suggestive of chronic hypersensitivity pneumonitis, with additional evidence of mild emphysema, and evidence of lymphocytic and constrictive bronchiolitis possibly representing an additional independent underlying process.
bird, as the bird has only been moved to the sun room and not out of the house. Strongly encouraged pt to completely remove the bird from the home. In regards to the steroids, reasonable to continue slow taper as you have been doing.