- 70 y.o. male with history notable for: emphysema/pulmonary fibrosis on home O2 (3L at rest, 4L with exertion), previous smoker (quit 10 years ago), severe OSA compliant with CPAP, arthritis, chronic rash, BPH who presents for follow-up.
- recently undergone a pharmacologic stress test
- no evidence of ischemia. He continued to have baseline dyspnea on exertion,
- reduced DLCO on PFTs.
- of recent
- significant decline in his respiratory status.
- rheumatology and had a serologic work-up completed that was inconsistent with any one diagnosis.
- increasing supplemental oxygen and is now on 3L at rest and 4L with exertion.
- stops after every 4 steps
- no chest pain or palpitations.
- TTE 2 years ago
- Normal LV cavity size, with
- mildly increased wall thickness,
- normal global systolic function.
- Calculated LVEF is 57%
- Normal RV size and global RV systolic function.
- Moderately dilated LA size (43 mL/m^2).
- rheum workup with
- + ANA /Cryo , referred to rheumatology
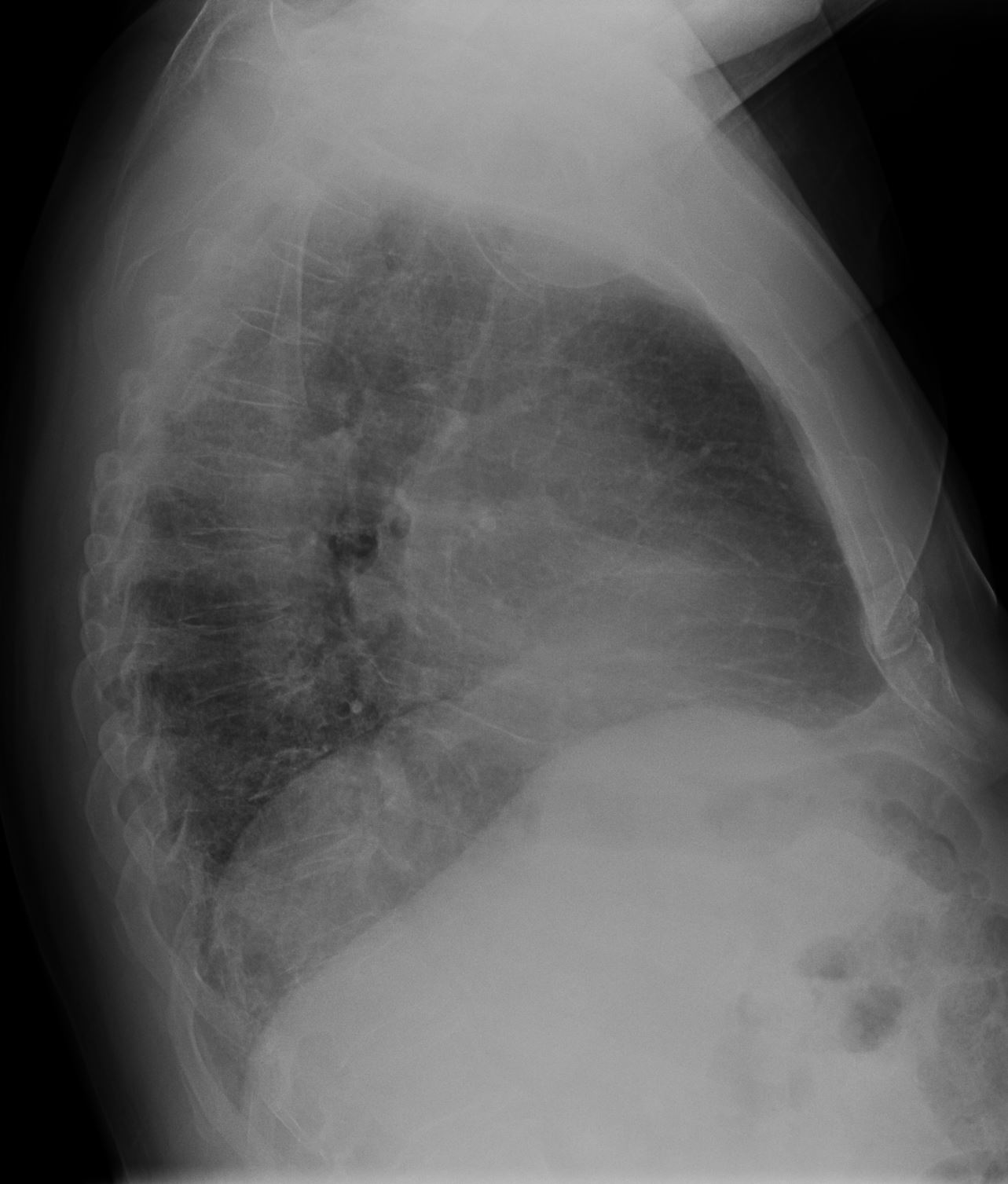
- CXR current

70M NSIP fibrotic 001 CXR decreased vol fibrosis PAH - Chest CT
-
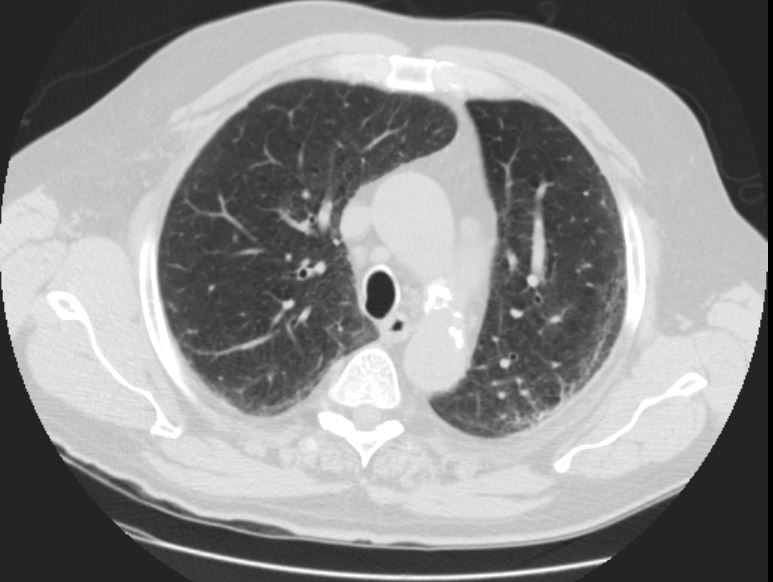
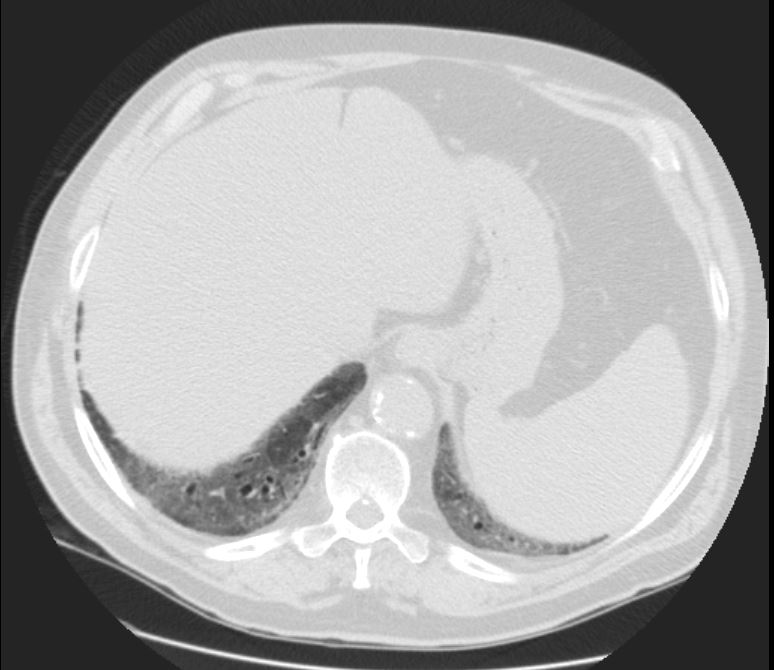
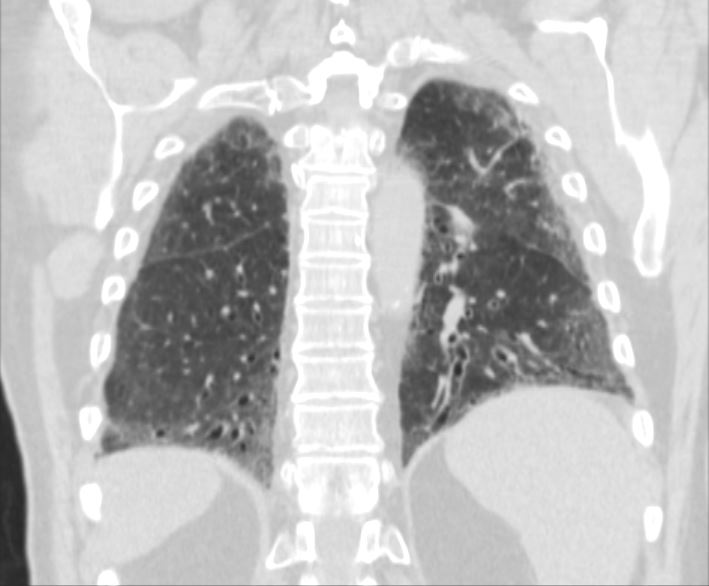
70M NSIP fibrotic 002 CT current subpleural fibrosis - COPD/subpleural fibrosis.
- Subpleural groundglass opacity
- bilateral reticulations
- slightly worse lower lobes.
- traction bronchiolectasis in the lower lobes.
- No honeycombing is visualized.
- suggestive of interstitial lung disease with a
- NSIP pattern.
- Findings are stable since 2 years ago
have progressed over 7years - Mild upper lobe centrilobular emphysema
- Enlarged main pulmonary artery measuring 4.3 cm indicating pulmonary hypertension