
RA c/b ILD (COP biopsy 2003) on tofacitinib and low dose prednisone who has been followed in the ILD clinic.
He has established RA (seropositive) and ILD. He has long standing lung disease (see below) but was reasonably stable until 2018 when started feeling unwell with troublesome cough and dyspnea on exertion. He also noted intermittent night sweats.
He has had lung disease starting around 2003 when he presented with BOOP (biopsy in 2003, see below), responsive to prednisone. He was later diagnosed with RA
1 year ago
cough at night occasionally productive of clear sputum for the preceding 2 months but declined any fevers, worsening dyspnea, or night sweats. At the time given the radiographic and physiologic progression of the underlying ILD he was started on nintedanib, TTE was requested, and we discussed the possibility of referral to a lung transplant center.
Normal biventricular size and systolic function with LVEF 65%. No regional wall motion abnormalities. Normal biatrial size. Mild aortic and mitral leaflet thickening without stenosis. Mild MR.
Otherwise valves appear functionally normal. Trace TR with estimated PA systolic pressure of 32 mmHg, assuming RA pressure of 3 mmHg. Interatrial septum appears intact by color Doppler. IVC is normal size. No significant pericardial effusion. Compared to prior
report of 4/2005, similar findings.
Pulmonary Function Trend Report
| Date | FVC | FEV1 | ratio | FeF25-75 | TLC | RV | DLCO |
| 8/24/20 | 3.4 98% | 2.75 101% | 81 | 2.7 103% | 5.47 95% | 1.93 93% | 8.17 35% |
| 5/16/19 | 3.18 84% | 2.64 89% | 79 | 3.29 115% | — | — | 8.1 35% |
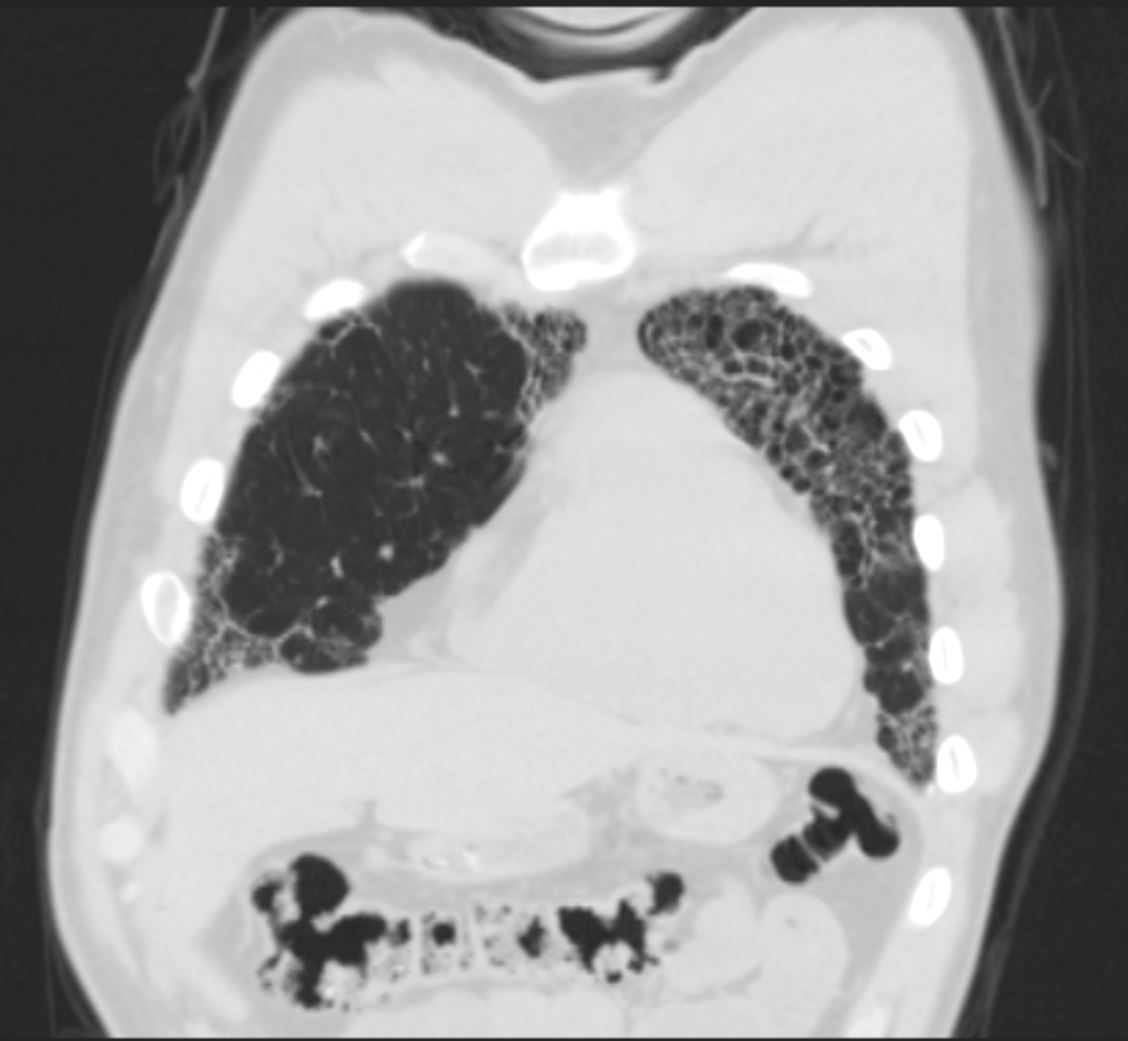
ILD conference – concensus was that the current radiographic pattern is consistent with RA-ILD in an UIP pattern
8 years ago – Hx of RA








15 years ago








1 year ago



References
Arakawa et al AJR 2011