
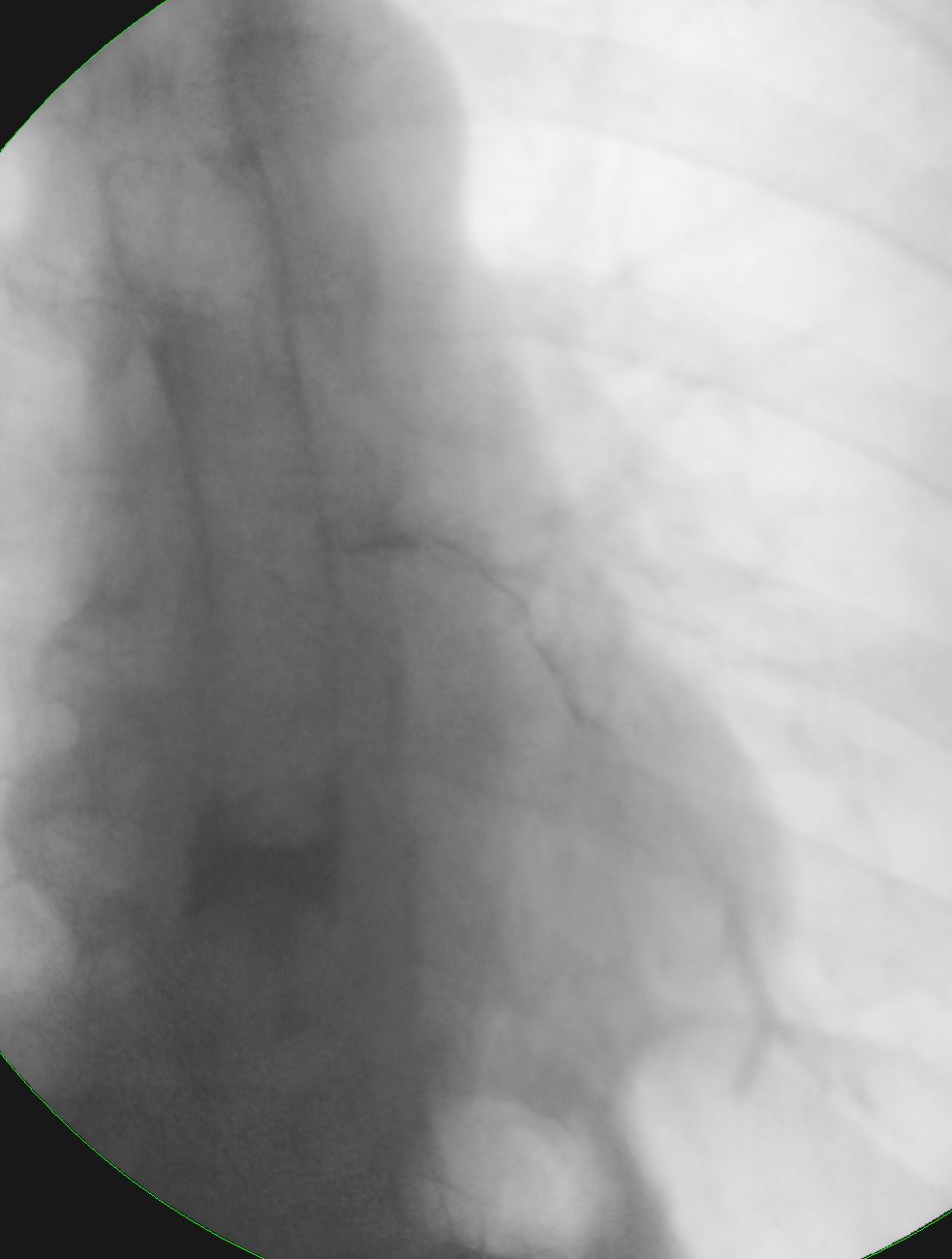
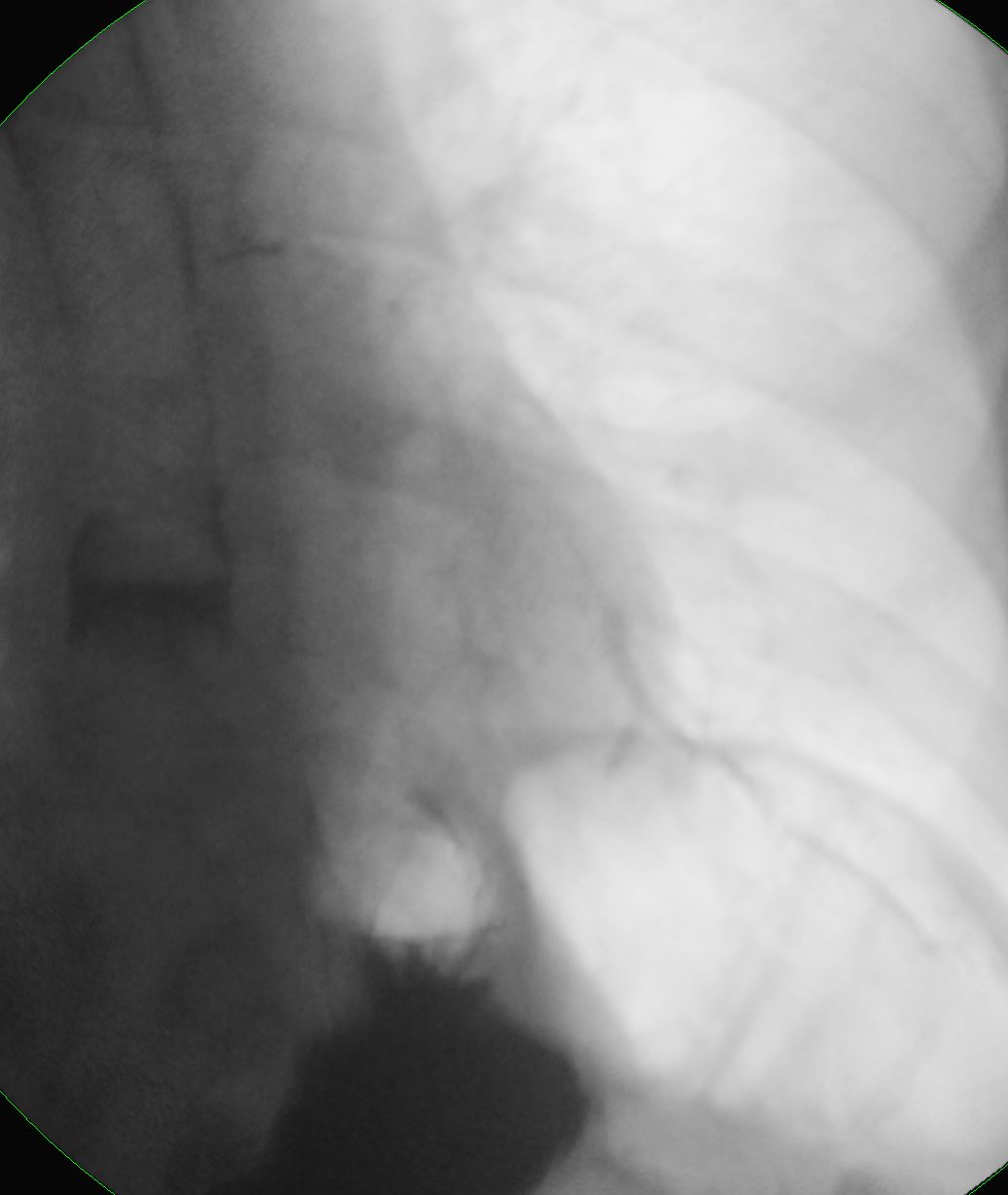
Barium Swallow Aspiration into the Trachea

Barium swallow in the LPO projection shows abnormal accumulation of contrast along the walls of the trachea secondary to aspiration. Contrast also lines the wall of the posteriorly positioned esophagus with a small air fluid level in the primary stripping wave of the esophagus. The contrast lined superior aspect of the epiglottis is seen among the vallecula and pyriform sinuses.
Ashley Davidoff MD TheCommonVein.net 46505c
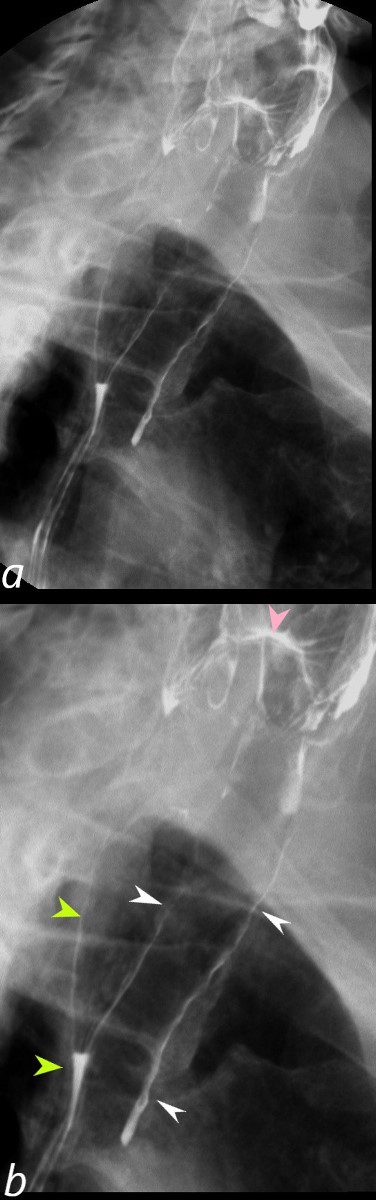
Barium swallow in the LPO projection shows abnormal accumulation of contrast along the walls of the trachea (b, white arrowheads) secondary to aspiration. Contrast also lines the wall of the posteriorly positioned esophagus (b, light green arrowheads) with a small air fluid level in the primary stripping wave of the esophagus (b, lower light green arrowhead). The contrast lined superior aspect of the epiglottis (pink arrowhead) is seen among the vallecula and pyriform sinuses.
Ashley Davidoff MD TheCommonVein.net 46505cL
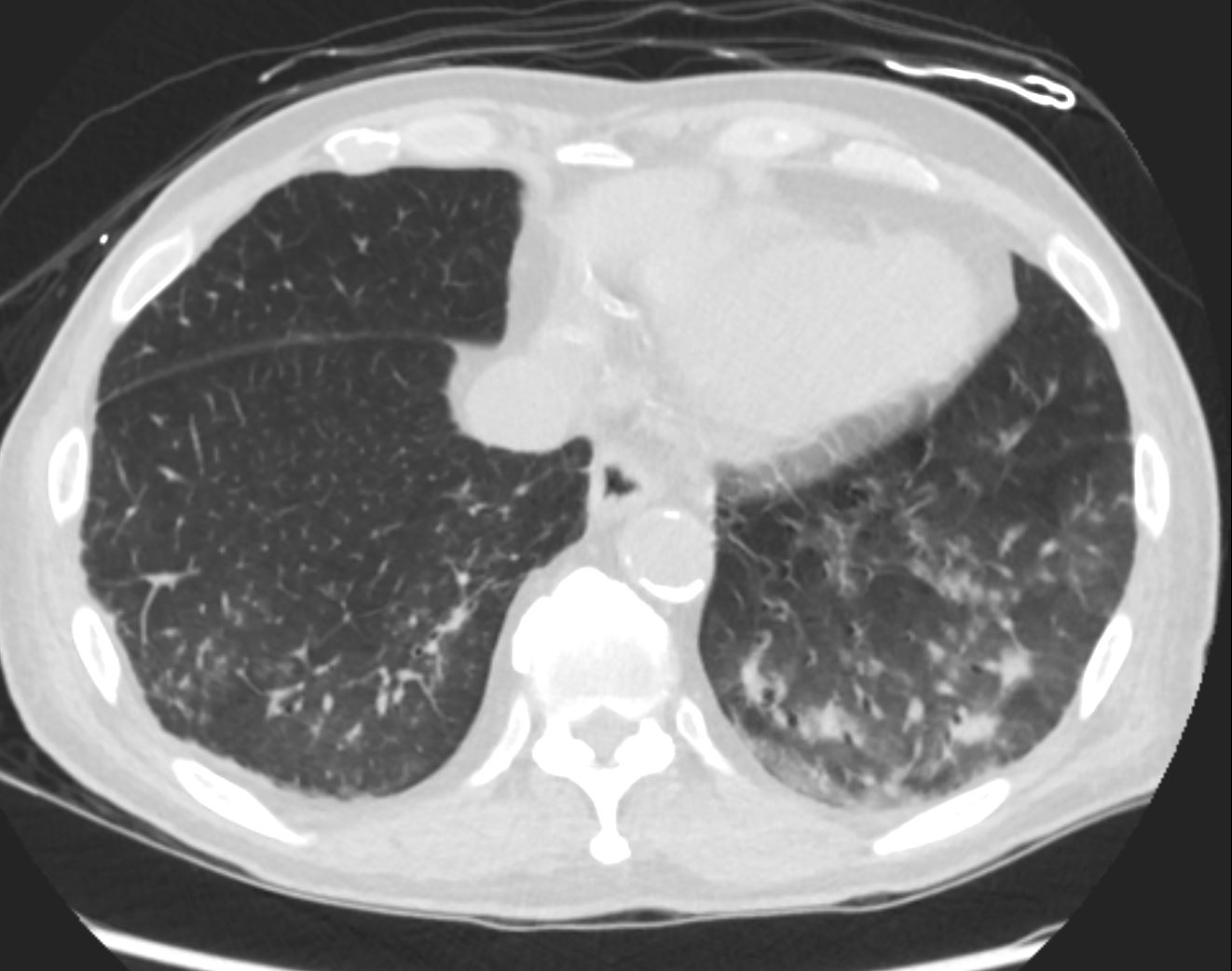
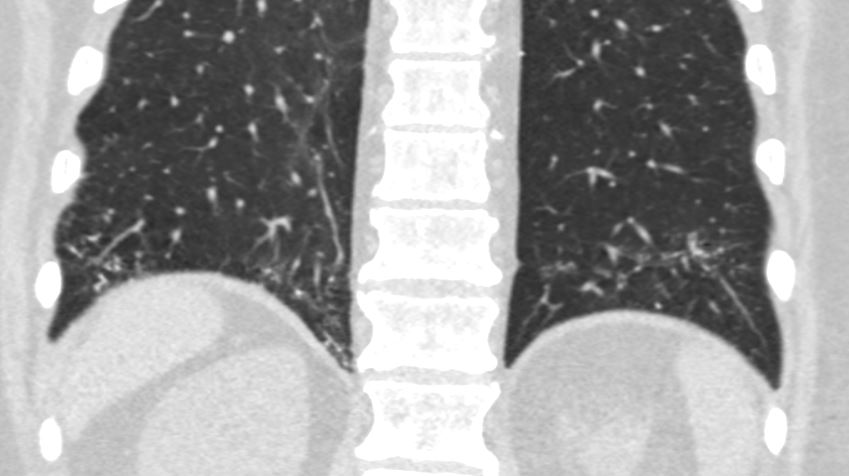
Bibasilar Aspiration Pneumonia
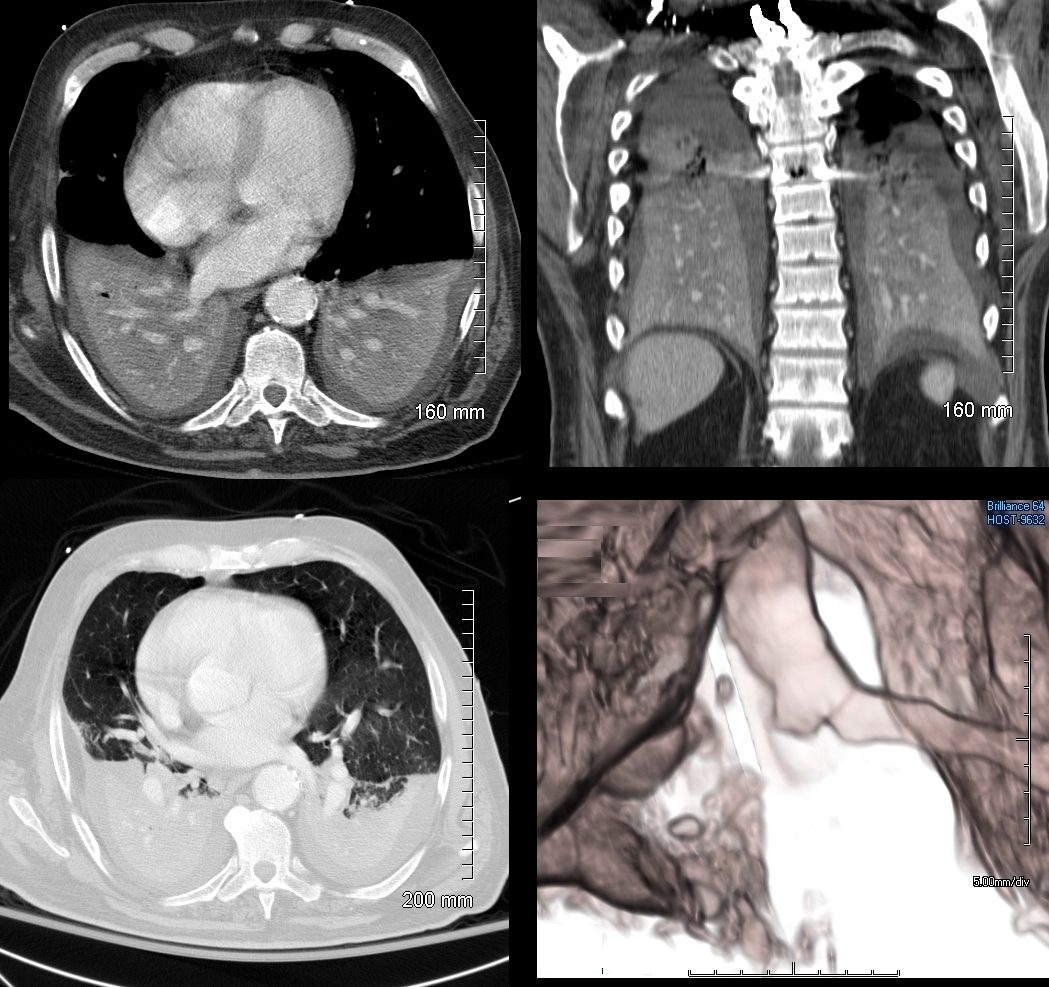
74 year old male alcoholic with bilateral basilar lobar atelectasis caused by bilateral aspiration
CT scan shows airless lower lobes with small bilateral effusions. 3D reconstruction shows total obstruction of the right mainstem bronchus, and patent proximal mainstem bronchus
Ashley Davidoff MD TheCommonVein.net
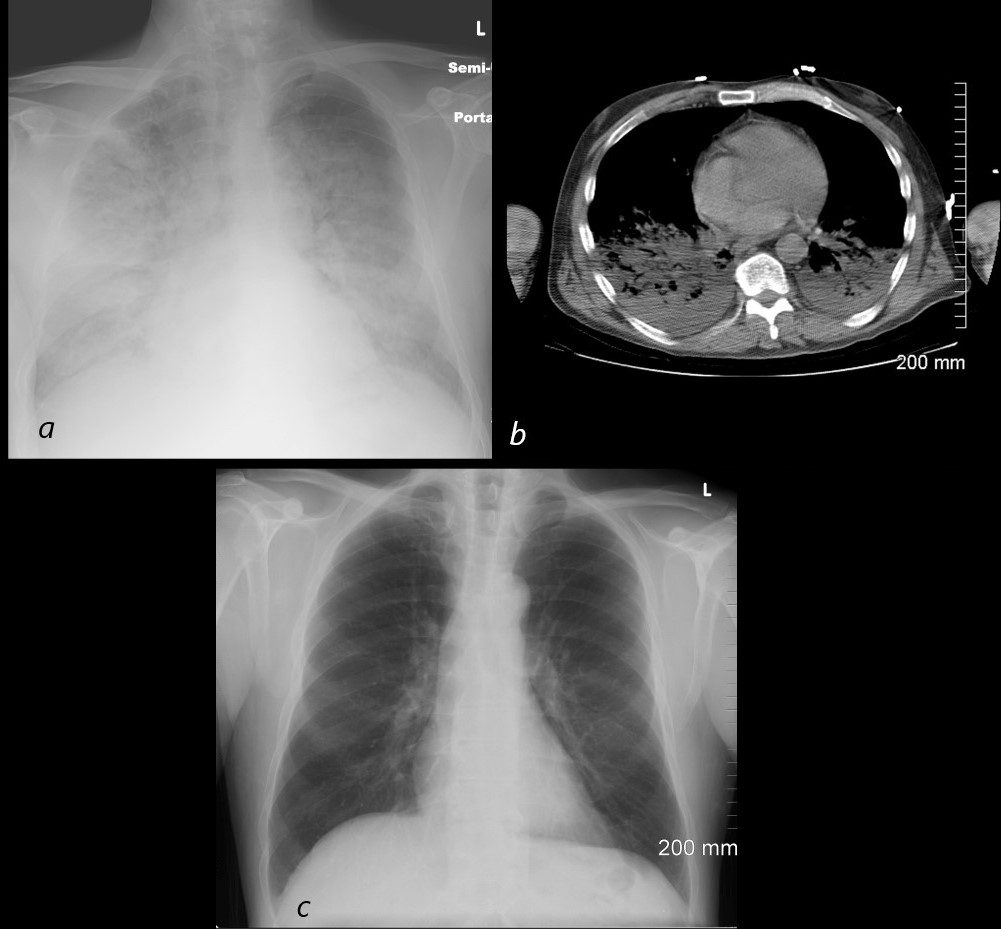
54 year old male alcoholic with seizures presents with diffuse alveolar disease consistent with pulmonary edema (a). CT scan (b) shows bibasilar infiltrates consistent with aspiration.
Follow up CXR 6 months later (c) shows resolution
Ashley Davidoff MD TheCommonVein.net
72-year-old male presents with acute dyspnea
Aspirate Occluding the Right Lower Lobe Bronchus

CT of a 72-year-old male with acute dyspnea shows a focal accumulation of low-density aspirate in the right lower lobe (white ring in lower image)
Ashley Davidoff MD TheCommonVein.net 136037c
Aspirate Occluding the Right Lower Lobe Bronchus
Medial and Lateral Basal Consolidation
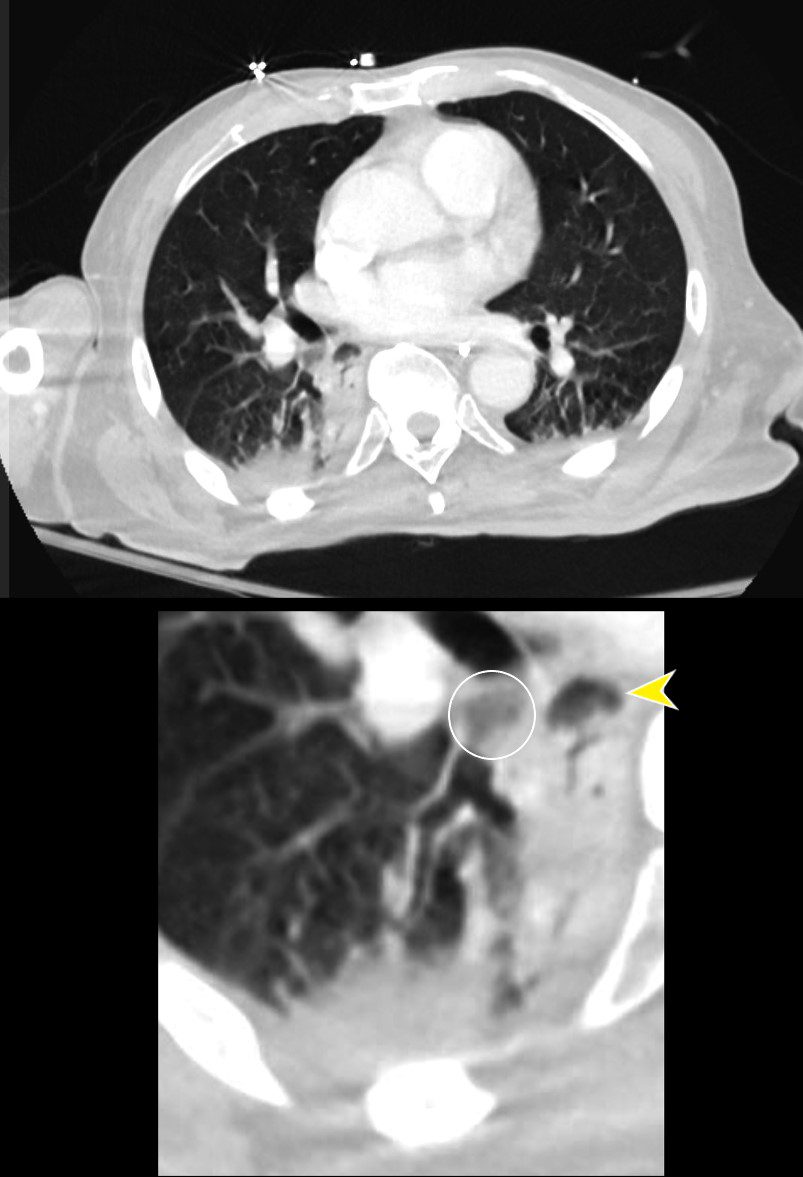
CT of a 72-year-old male with acute dyspnea shows a focal accumulation of low-density aspirate in the right lower lobe (white ring in lower image). Distal to the obstruction the posterior segmental and medial segmental airways are patent, but associated atelectasis is noted in those segments of the right lower lobe. The esophagus is displaced to the right and appears to contain some aerated content.
Ashley Davidoff MD TheCommonVein.net 136038cL
Aspirate Partially Occluding the Right Lower Lobe Bronchus and Extending into the Medial and Posterior Segments with Associated Atelectasis and Consolidation
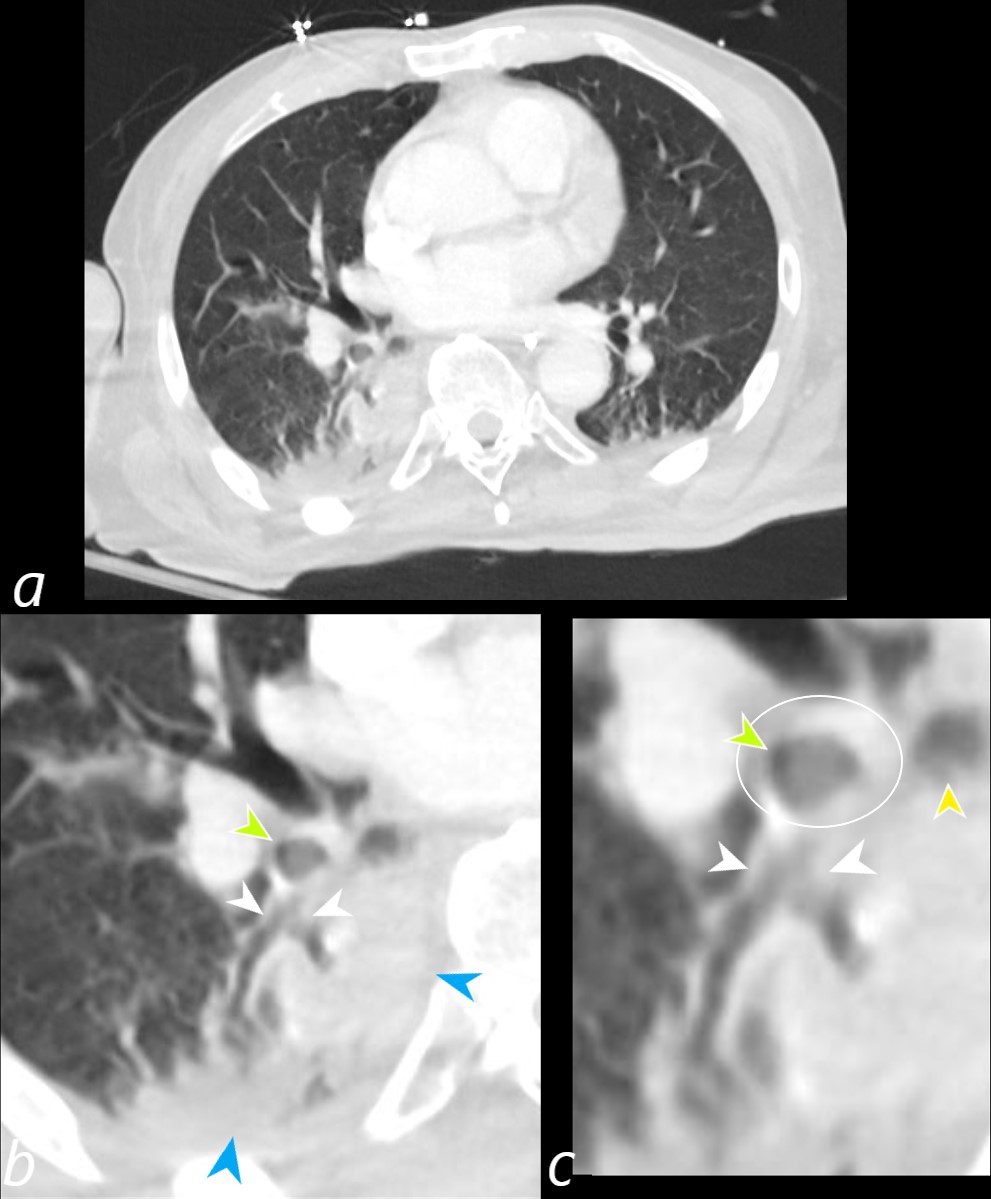
CT of a 72-year-old male with acute dyspnea shows a sub-totally occluded bronchus distal to the more complete obstruction noted in the previous section (green arrowheads b and c, and ringed in white in c). Distally at the branch point of the lower lobe bronchus there is partial filling of the medial and posterior segments (white arrows b and c). Secondary to the aspiration there is post obstructive atelectasis of the medial and posterior segments of the right lower lobe. The esophagus is displaced to the right, and appears to contain some aerated content (yellow arrowhead c).
Ashley Davidoff MD TheCommonVein.net 136041cL
Aspiration and Tree in Bud
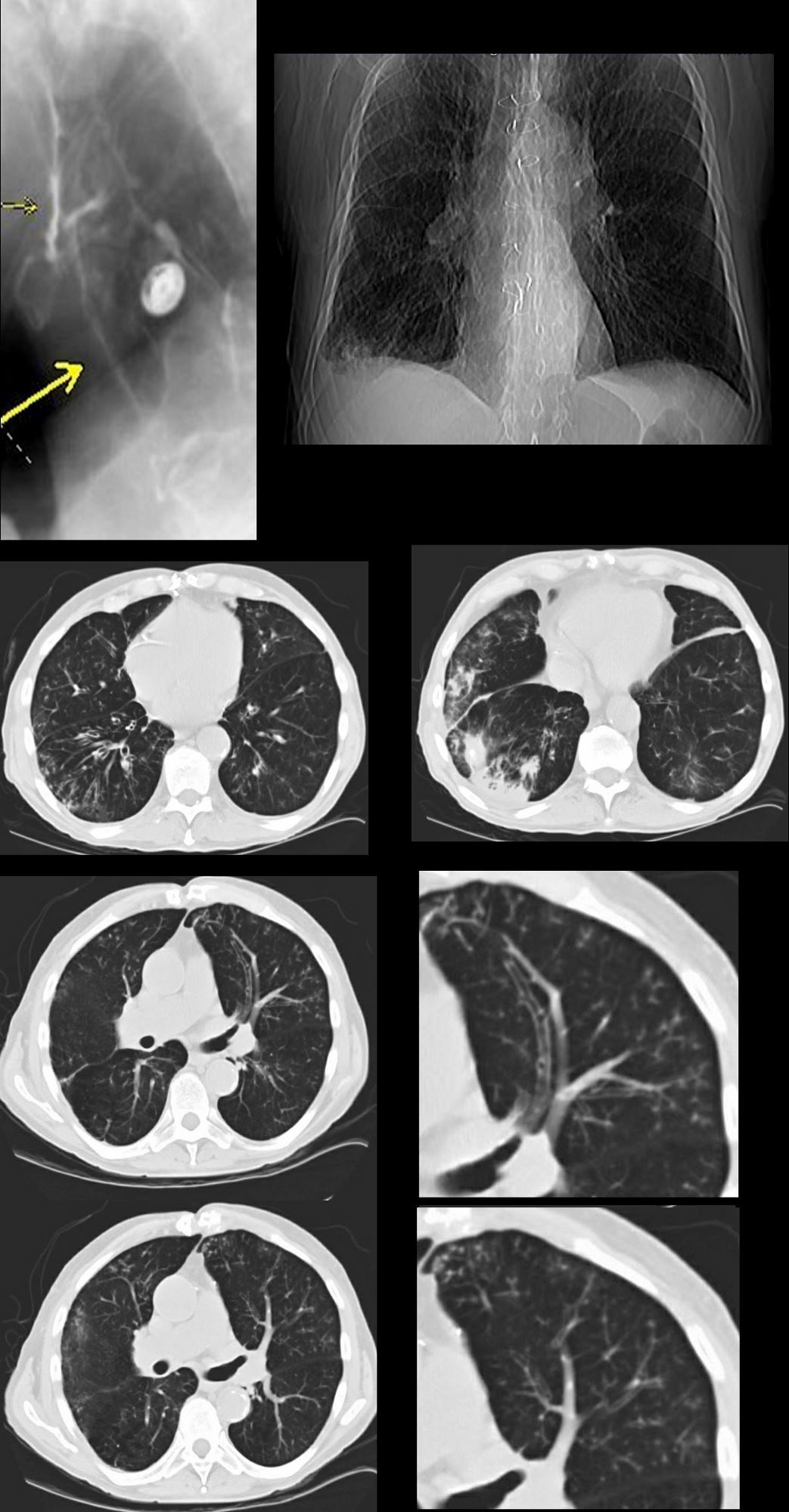
87 year old male with history of cough and suspicion of aspiration shows barium aspiration into the proximal trachea (upper right) The scout view ( upper right) shows an infiltrate at the right base, Thickened airways in the right lower lobe (2nd row left ) is associated with a pneumonic infiltrate in the right lower lobe (lower right) consistent with aspiration. There are thickened airways to the lingula (3rd and 4th row) with magnified view showing tree in bud changes (right sided images 3rd and 4th row)
All these finding likely relate to spiration though lingula involvement is not usual
Ashley Davidoff MD Ashley Davidoff MD TheCommonVein.net
Tree in Bud

Ashley Davidoff MD TheCommonvein.net
Ashley Davidoff MD TheCommonvein.net
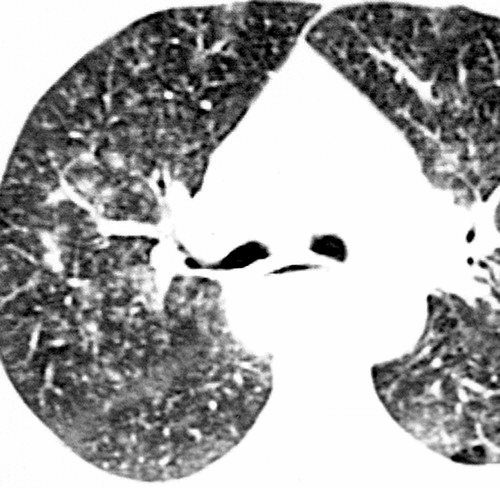
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005

Ashley Davidoff MD The CommonVein.net
Ashley Davidoff MD The CommonVein.net
Aspiration from a Esophageal to Bronchial Fistula in a Patient with Esophageal carcinoma and a Stent
Ashley Davidoff MD TheCommonVein.net squamous-cell-carcinoma-001
Ashley Davidoff MD TheCommonVein.net squamous-cell-carcinoma-002

Ashley Davidoff MD TheCommonVein.net squamous-cell-carcinoma-003