
Classification of Diseases
In this section we discuss the various ways lung cancer has been classified. The two most important classifications are the histological and the TNM staging classifications. The histopathological classifications divide the disease into two fundamental groups as we discussed in above in the sttrucural principles section; small cell and non small cell carcinomas. This distinction is important in the approach to the management and prognostication of the disease.
The staging classification divides the disease into groups based on size of tumor, extent of adenopathy, and systemic extent of disease.
Other classifications that are helpful include the functional status of the patient in considering surgery, and the radiological classifications of lung tumor based on morphology.
Histopathology
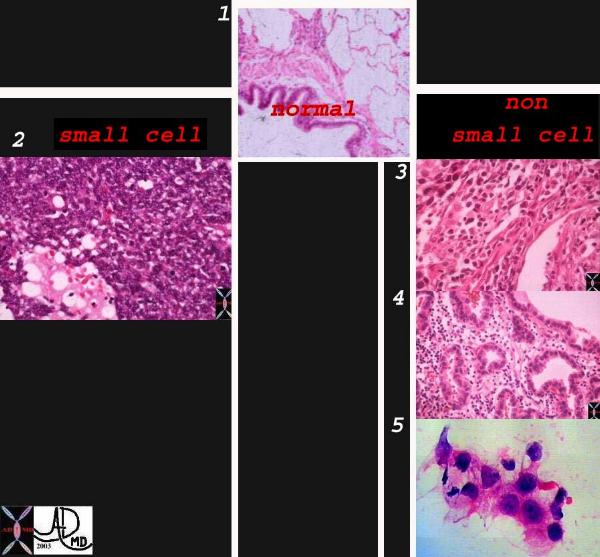
Classification system of carcinoma of the lung based on histological subtype. This collage of histopatholgy images of lung carcinoma shows part of a normal bronchiole and a few alveoli (1), followed by a small cell carcinoma (left lower 2) and non small cell carcinoma grouped together on the right side with squamous cell (3), adenocarcinoma with glandular formation (4), and undifferentiated large cell derived from pleural aspirate (5). 1-4
Courtesy Dr Armando Fraire MD, and image 6 courtesy of tumorboard.com 32501cL02
Histological Types
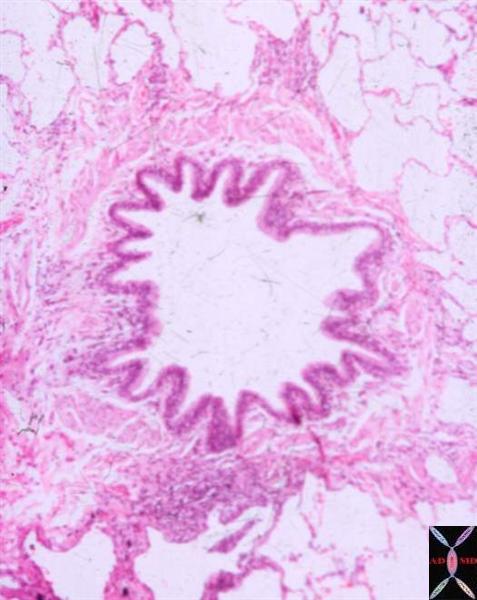
Normal
Courtesy Dr. Armando Fraire
TheCommonVein.net
32508
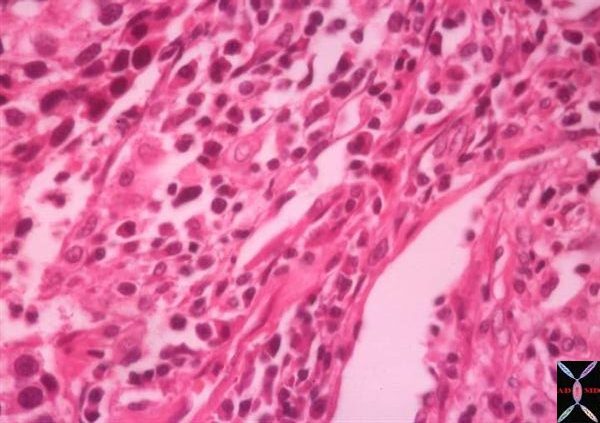
Small Cell

Courtesy Dr Armando Fraire MD
TheCommonVein.net 32517
Squamous Cell
TheCommonVein.net
32501
Keywords
lungs pulmonary neoplasm primary malignant malignancy squamous cell carcinoma SCC histopathology
Adenocarcinoma
TheCommonVein.net
32510
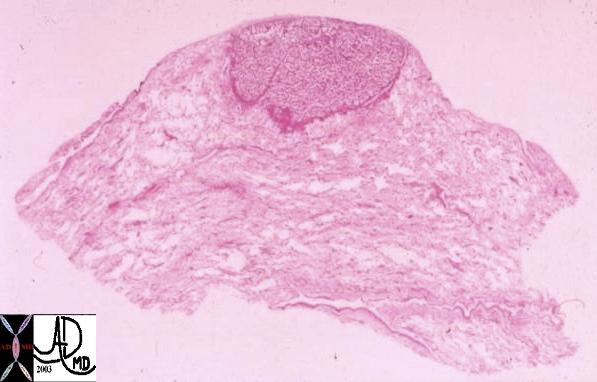
This whole mount of a part of the periphery of the lung reveals a peripherally located nodule without evidence puckering of overlying pleura. Microscopically this proved to be a papillary carcinoma.
Courtesy Armando Fraire MD. 32812
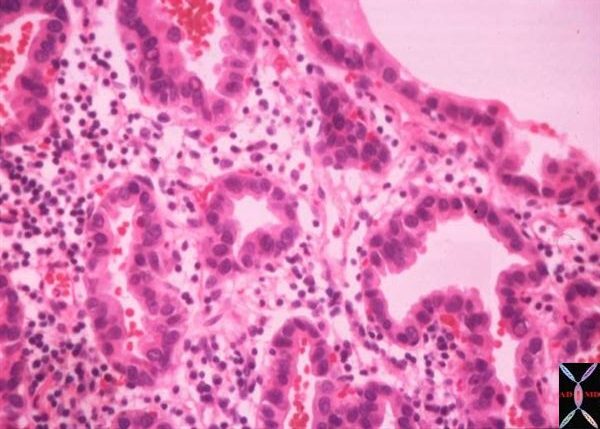
Adenocarcinoma with Lepidic Growth
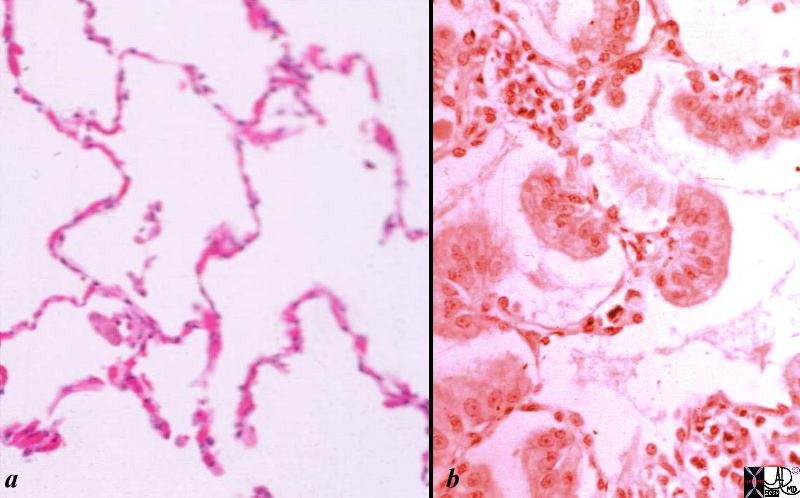
Histological sections of a group of a normal alveoli (a) and alveoli filled with nests of malignant cells.
Normal lung- is shown in low magnification. Note the cup-shaped alveolar spaces outlined by delicate thin alveolar capillary membrane with the lumen of the alveoli being mostly empty .
In image b the malignant cellular material originates from and spreads along the alveolar epithelium without destroying the alveolar walls. The malignant clusters of cells seem to be hanging from the alveolar epithelium like washing from a washing line. Note groups of tall, columnar, mucin producing cells spreading along preexisting alveolar walls, which is typical of bronchioloalveolar carcinoma.
Courtesy Dr Armando Fraire MD
TheCommonVein.net
32828c02.8s
Large Cell
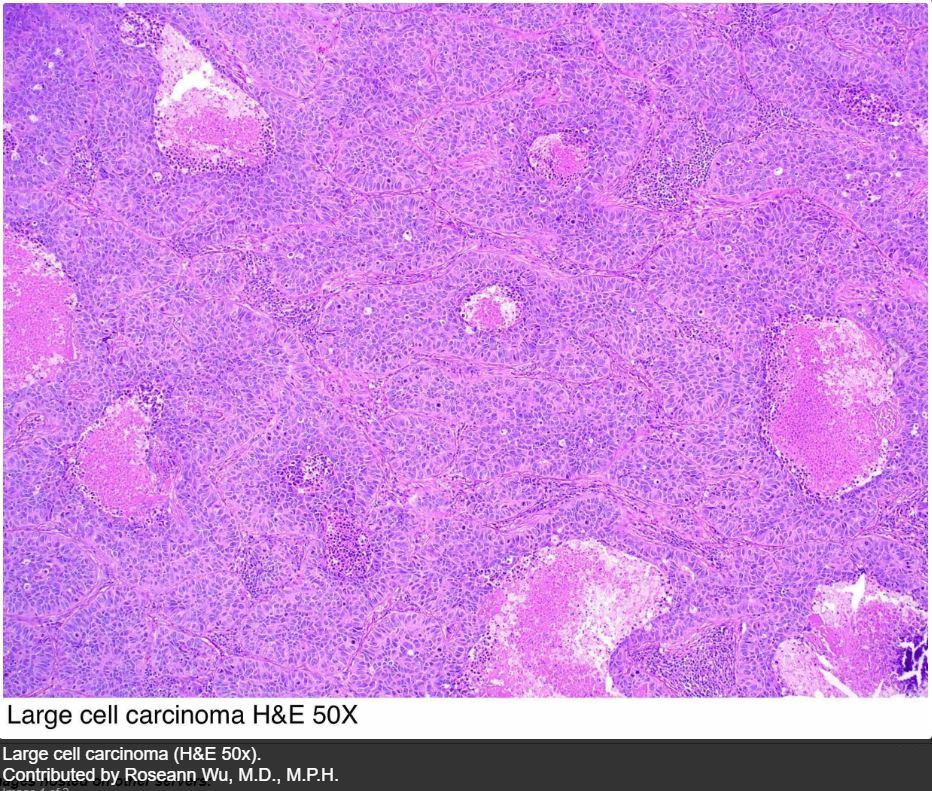
Contributed by Dr Rosean Wu MD MPH from pathologyoutlines.com/
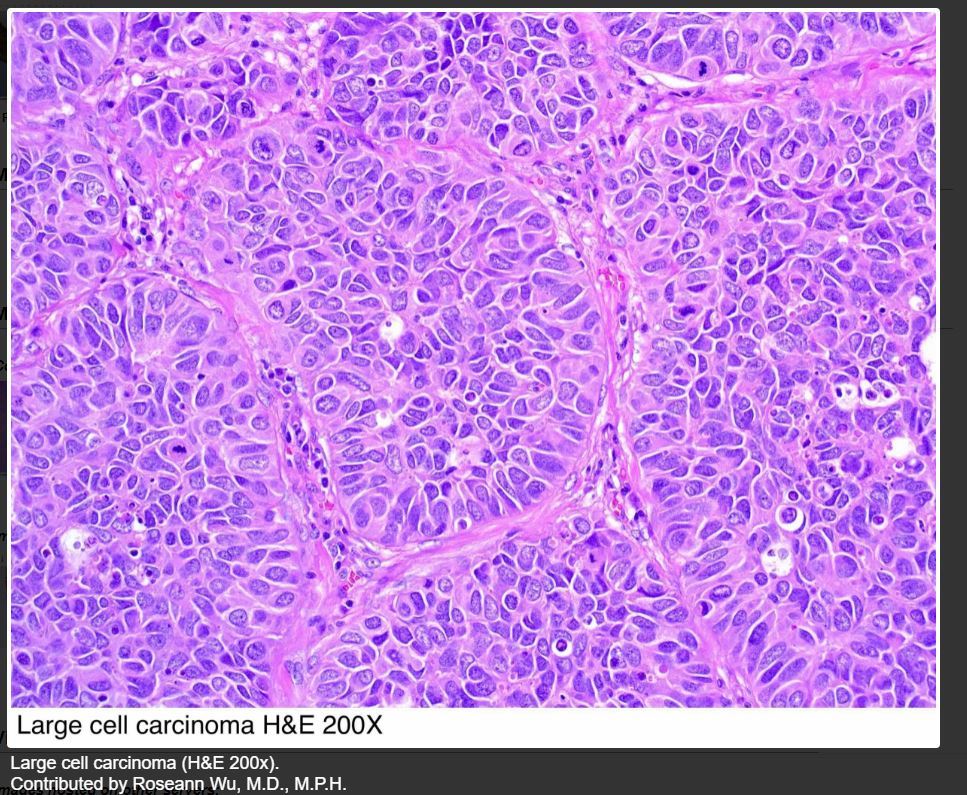
Contributed by Dr Rosean Wu MD MPH from pathologyoutlines.com/
|
Histological Types |
% Total |
|
Squamous Cell |
29% |
|
Small Cell |
20% |
|
Large Cell Carcinoma |
9% |
|
Large Cell Neuroendocrine |
2% |
|
Adenocarcinoma a) acinar b) papillary c) bronchioalveolar d) mucus secreting |
32% |
|
Adenocarcinoma with Lepidic Growth (Bronchioloalveolar) |
3% |
|
Others |
12% |
Preinvasive lesions include;
Squamous dysplasia/carcinoma in situ
Atypical adenomatous hyperplasia
Diffuse idiopathic pulmonary neuroendocrine hyperplasia
Gross Pathology
Carcinoma of the lung most commonly presents as a mass and less commonly as an alveolar process which is the mode of presentation for the bronchioloalveolar type. However because it originates in a tubular system and because of its infiltrative nature the macroscopic picture will depend on the presence or absence of atelectasis, localized emphysema, associated pneumonia, lymphangitis, pleural involvement and pericardial involvement
Size
Malignant tumors range in size from a few mms to up to 10 or even 15 cms.
Large cell carcinoma is usually large, bulky, and well circumscribed.
Shape
The tumors themselves are mostly nodular or round or irregularly shaped, except for alveolar cell which may look like a segmental pneumonia. Bronchioalveolar carcinoma may also take the form of a single nodule or more often, as multiple diffuse nodules that coalesce to produce a pneumonia-like consolidation.
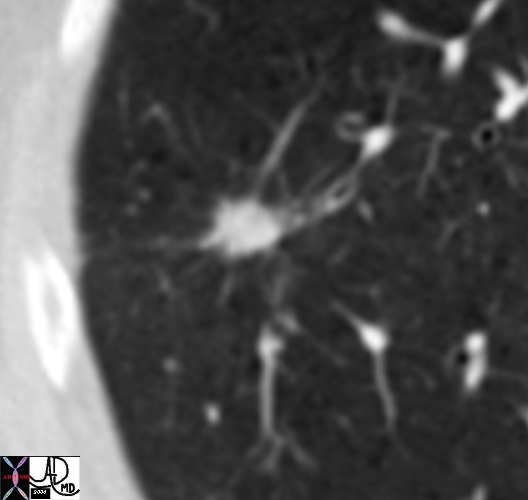
Suspicious Spiculated Nodule |
| 46361b01 Copyright 2010 Courtesy Ashley Davidoff MD |
Position
Squamous and small cell carcinomas tend to be central while adenocarcinomas including alveolar carcinomas tend to be peripheral, often near a pleural surface. The pleural surface is often pinched over the tumor. Squamous cell carcinoma also tends to be found more commonly in the upper bronchi.
Character
Adenocarcinoma is usually hard to the feel with a white or grey and glistening matrix.
Squamous cell carcinoma usually presents as a well circumscribed, rubbery mass appearing as a gray-white and dry matrix, often associated with hemorrhage, necrosis, and cavitation. (10-20%) (32202c)
Large cell carcinoma is usually a well delineated bulky tumor with a pink gray cut surface often complicated by hemorrhage and necrosis.
Bronchioloalveolar carcinoma, may present as a mucinous mass, as diffuse multinodular lesion, or as a infiltrate.