
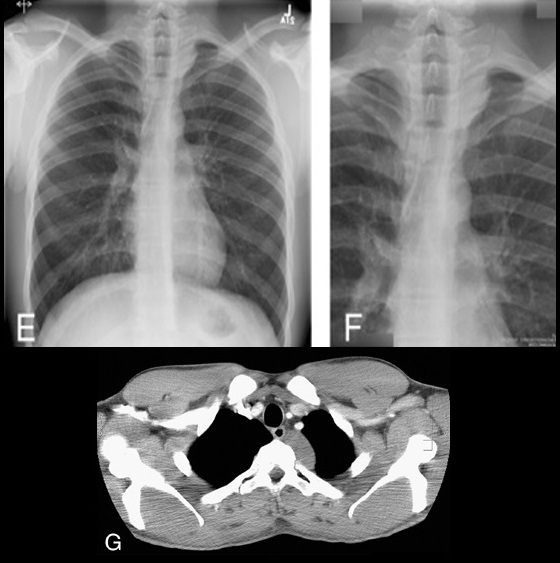
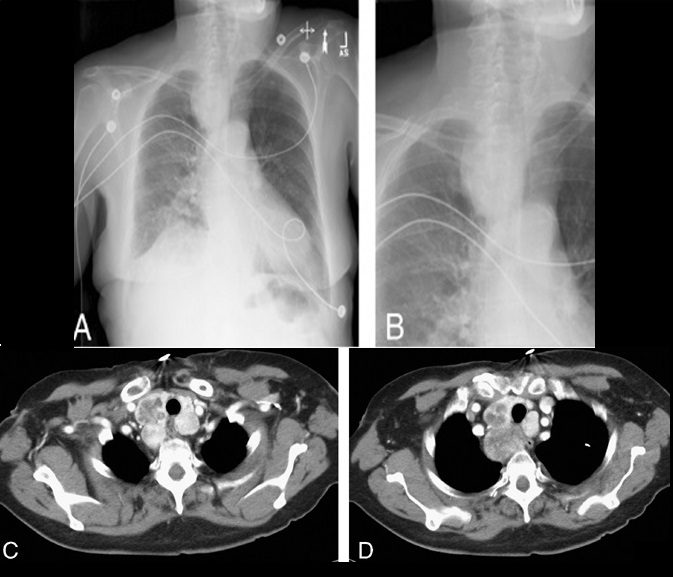
Cervicothoracic sign. Frontal radiograph of the chest with a coned view (A, B) demonstrates a mass projecting over the right superior mediastinum with indistinct borders along its superior margin. Follow-up enhanced CT of the chest (C, D) reveals a mass extending from the cervical region into the anterior mediastinum representing a multinodular goiter. Conversely, in the case of a posterior mediastinal mass, the supralateral margins project above the level of the clavicles and are clearly defined on the frontal radiograph (E, F) in this patient (different patient from A, B) with a biopsy-proven ganglioneuroma (G, CT image).
Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
This sign is based on the understanding that if a thoracic mass is in direct contiguity with the soft tissues of the neck, the borders delineating their point of contact will be lost or obscured.11 Anatomically, the thoracic inlet parallels the first ribs, and the posterior aspects of the lung apices extend further superiorly than the anterior portions.12 On PA chest radiographs, a mass clearly delineated on all borders above the level of the clavicles lies posterior to the level of the trachea and completely within the lung.13 When the cephalic border of a mass is obscured at or below the level of the clavicles, it is deemed to be a “cervicothoracic lesion”13 involving the anterior mediastinum (Figs. 3A–E). Mediastinal masses posterior to the trachea are well outlined above the level of the clavicles due to the interface with lung in the posterior aspects of the lung apices (Figs. 3F, G).
Cervicothoracic sign
Cervicothoracic sign. Frontal radiograph of the chest with a coned view (A, B) demonstrates a mass projecting over the right superior mediastinum with indistinct borders along its superior margin. Follow-up enhanced CT of the chest (C, D) reveals a mass extending from the cervical region into the anterior mediastinum representing a multinodular goiter. Conversely, in the case of a posterior mediastinal mass, the supralateral margins project above the level of the clavicles and are clearly defined on the frontal radiograph (E, F) in this patient (different patient from A, B) with a biopsy-proven ganglioneuroma (G, CT image).
Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
This sign is based on the understanding that if a thoracic mass is in direct contiguity with the soft tissues of the neck, the borders delineating their point of contact will be lost or obscured.11 Anatomically, the thoracic inlet parallels the first ribs, and the posterior aspects of the lung apices extend further superiorly than the anterior portions.12 On PA chest radiographs, a mass clearly delineated on all borders above the level of the clavicles lies posterior to the level of the trachea and completely within the lung.13 When the cephalic border of a mass is obscured at or below the level of the clavicles, it is deemed to be a “cervicothoracic lesion”13 involving the anterior mediastinum (Figs. 3A–E). Mediastinal masses posterior to the trachea are well outlined above the level of the clavicles due to the interface with lung in the posterior aspects of the lung apices (Figs. 3F, G).