
In a Nutshell
-
- Upper Lobe Predominance
- Follow Lymphatics
- Pleural and Fissural
- Centrilobular and Interlobular Septa
- Lymph Nodes (Egg Shell)
- Nodules that Cluster
THE “S” OF SARCOIDOSIS
It starts at the surface, travels along the pleura and then the fissures towards the hila and mediastinum, then back along the pleura and finally going centrally along the bronchovascular bundles towards the hila

“S” of SARCOIDOSIS It starts at the surface Travels along the pleura and the n the fissures towards the hila and mediastinum, then back along the pleura and finally going centrally along the bronchovascular bundles towards the hila
Ashley Davidoff MD
Sarcoidosis is a nodular granulomatous disease which predominates in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The “S” for sarcoidosis drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting superficially in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
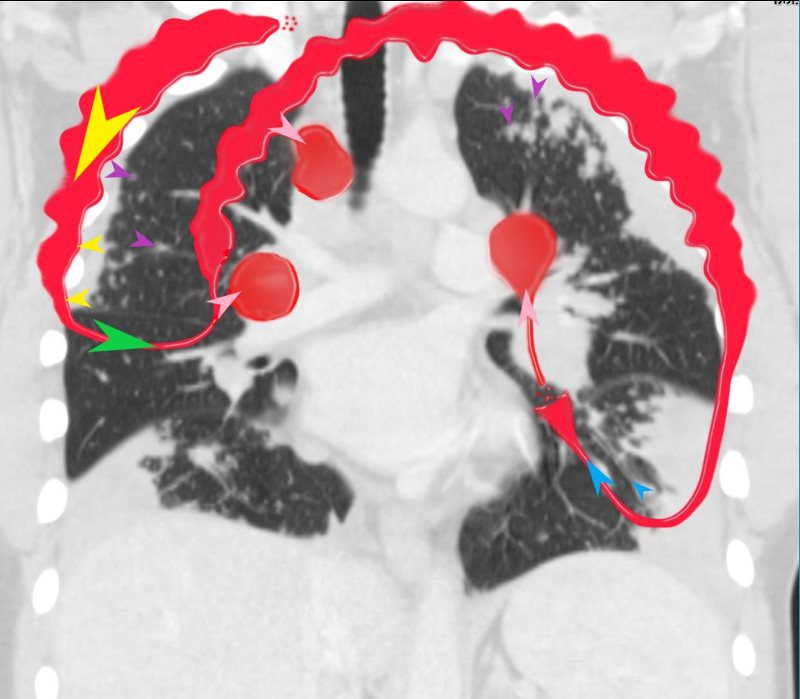 LYMPHATIC DRAINAGE
LYMPHATIC DRAINAGE“S” of SARCOIDOSIS
In this diagram the arrows show the direction of flow of the lymphatics. Pleural lymphatics (yellow arrows), Fissural lymphatics, green arrows), flow from the interlobular septa (purple arrows) and along the bronchovascular bundles (blue arrows) all flow toward the lymph nodes in the hila and mediastinum (pink arrows).
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The “S” drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
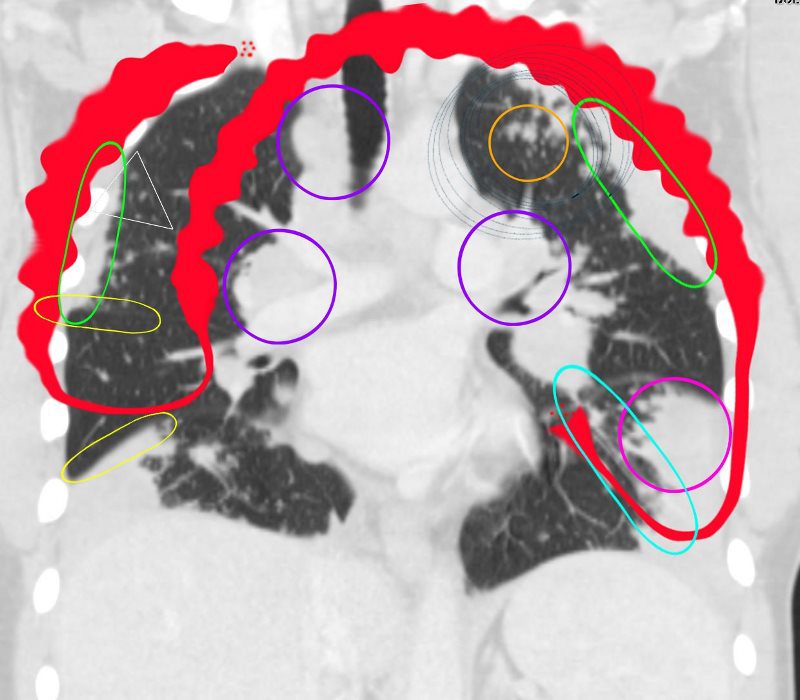
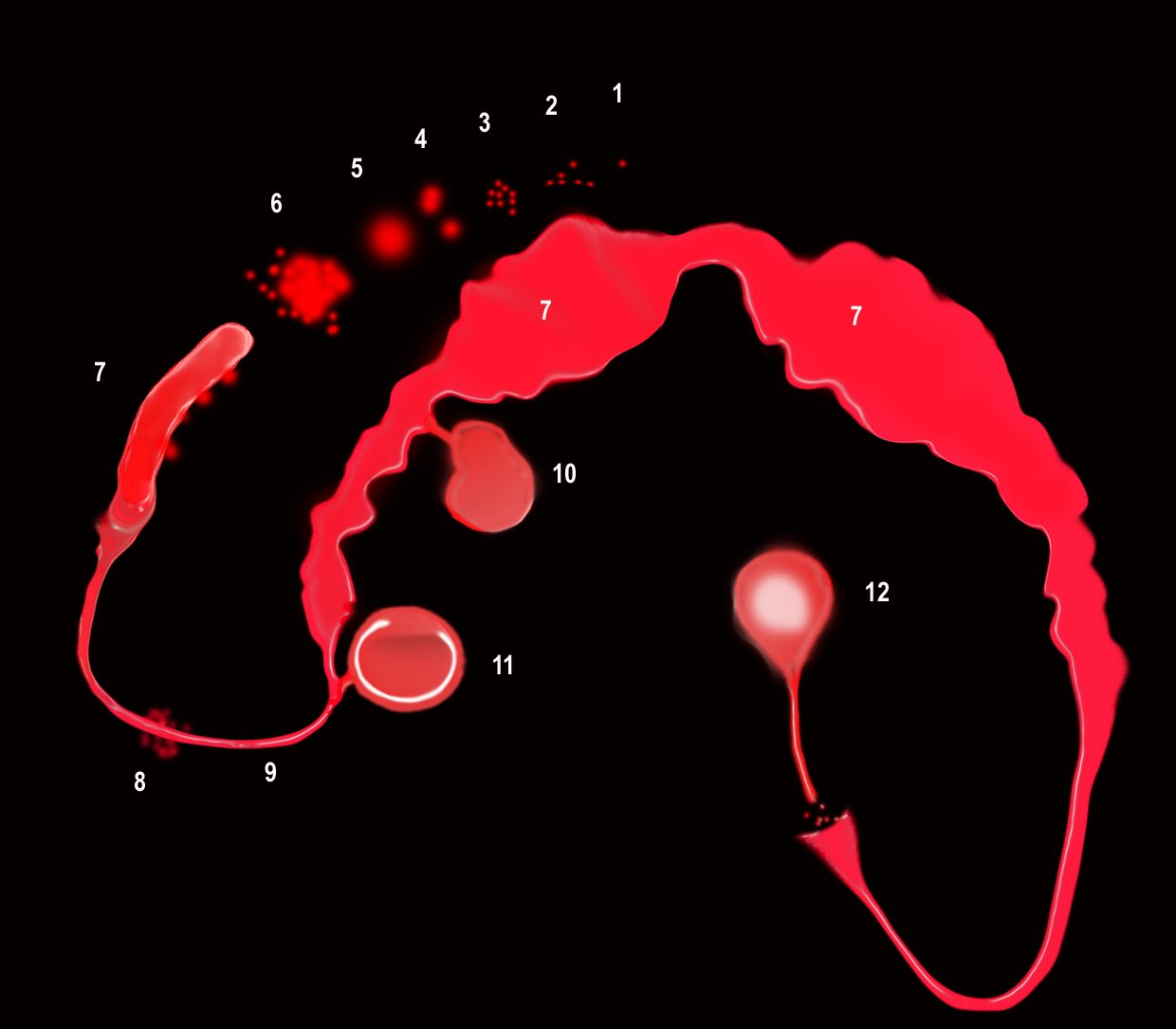 MORPHOLOGY OF THE STRUCTURAL CHANGES
MORPHOLOGY OF THE STRUCTURAL CHANGES“S” of SARCOIDOSIS
The granulomas start as micronodules in close association with the lymphatics (1) spread in the intralobular septa and centrilobular bronchioles ((2) cluster and conglomerate to form macro nodules (4,5) sometimes manifesting as the galaxy sign (6). As they cluster and conglomerate they can cause conglomerate masses along the pathway (7) most commonly centrally as the lymphatics become confluent in the hila (7)
The lymphovascular bundles may be accompanied by nodularity (8) or just by thickening (9).
The lymph nodes in the mediastinum become significantly enlarged and fleshy (10). They often calcify (12) sometimes on the calcify on the rim of the node (eggshell calcification (11)
Ashley Davidoff MD
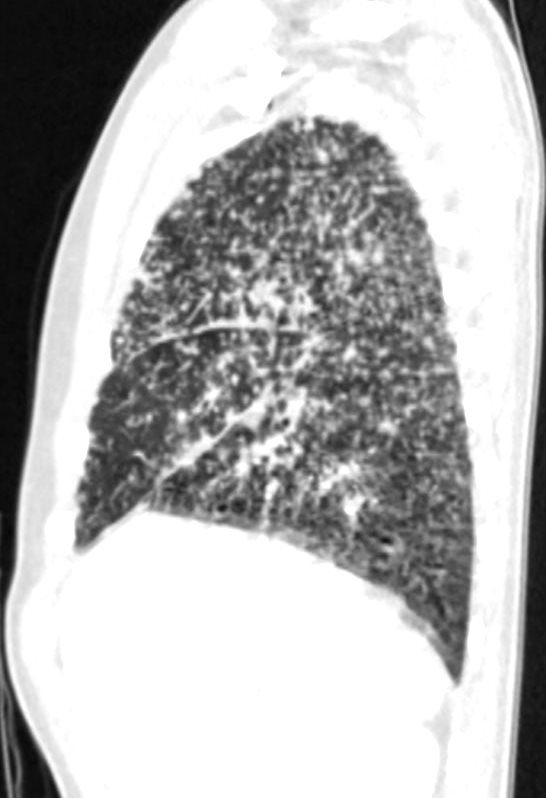
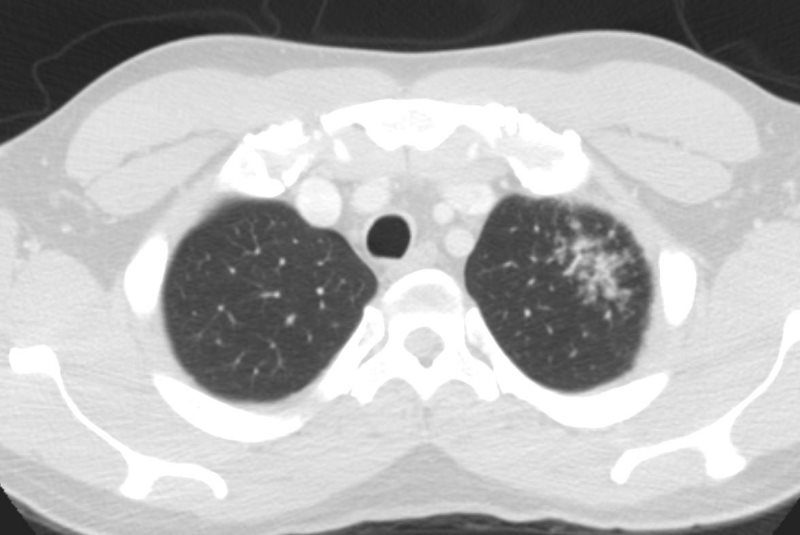
Nodules in the Secondary Lobules
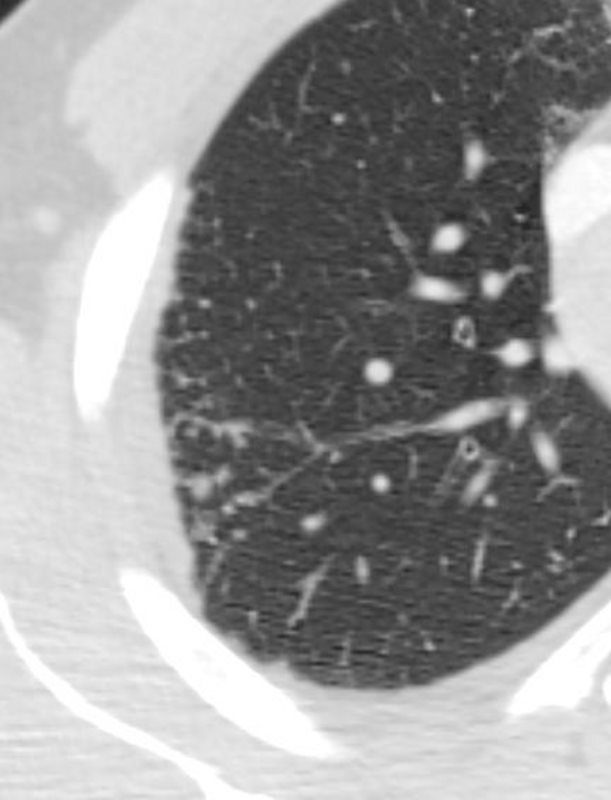 CT WITH SUBPLEURAL AND LYMPHOVASCULAR NODULES IN THE RIGHT UPPER LOBE – INTERLOBULAR SEPTA AND CENTRILOBULAR
CT WITH SUBPLEURAL AND LYMPHOVASCULAR NODULES IN THE RIGHT UPPER LOBE – INTERLOBULAR SEPTA AND CENTRILOBULAR
Ashley Davidoff MD
Coalescence Thickening and Nodularity in Pleura and Subpleural Region
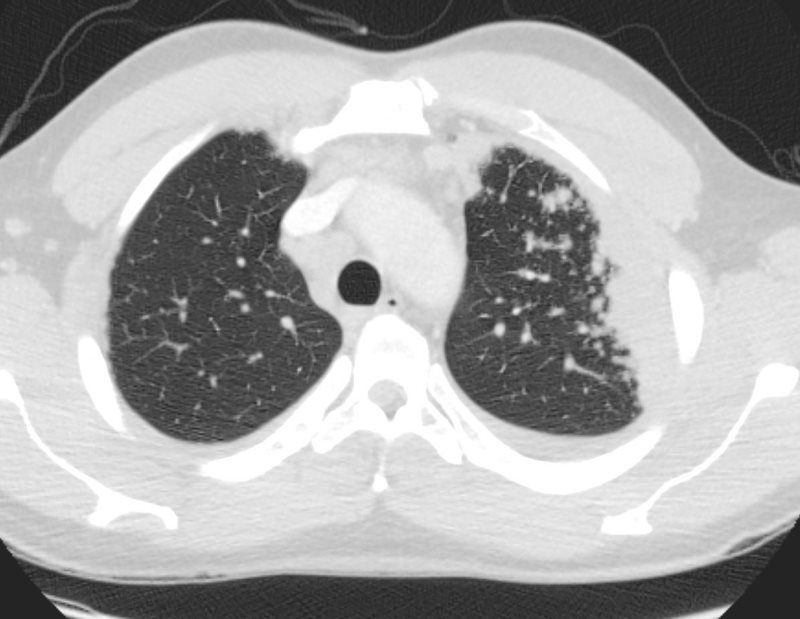 CT WITH SUBPLEURAL AND LYMPHOVASCULAR NODULES IN THE LEFT UPPER LOBE
CT WITH SUBPLEURAL AND LYMPHOVASCULAR NODULES IN THE LEFT UPPER LOBE
Ashley Davidoff MD
- When the nodularity, clustering and or mass formation involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Fissural Involvement

When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
Ashley Davidoff MD
Ashley Davidoff MD
Lympadenopathy
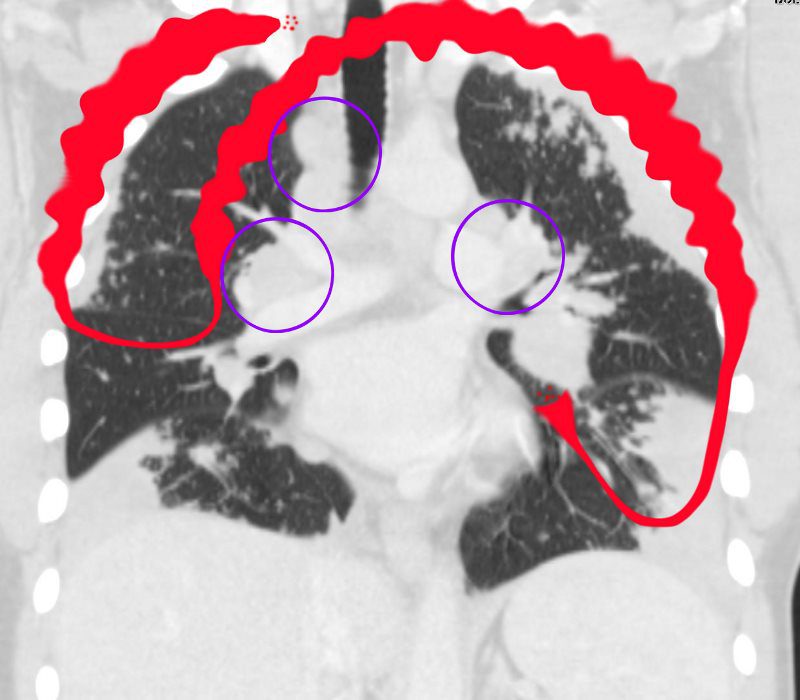
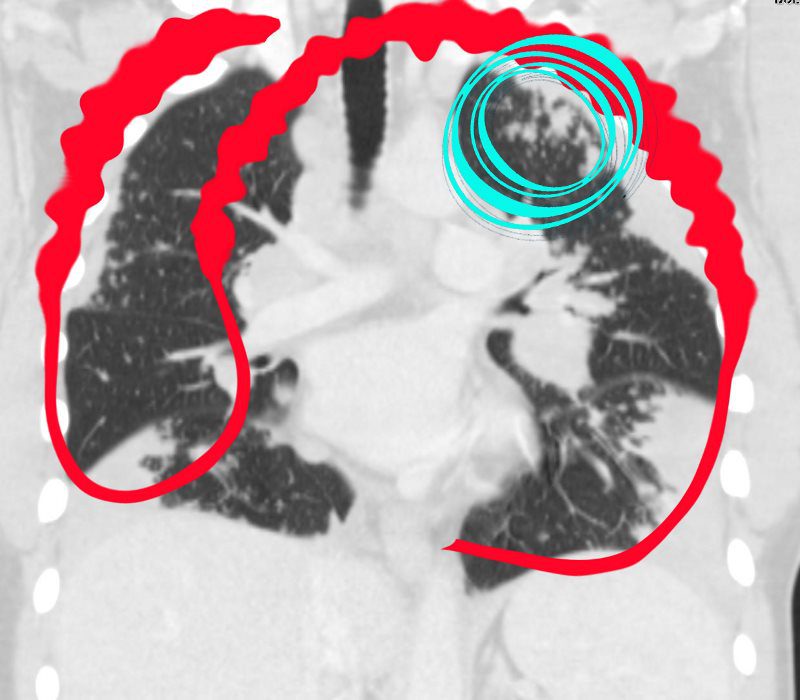
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Ashley Davidoff MD
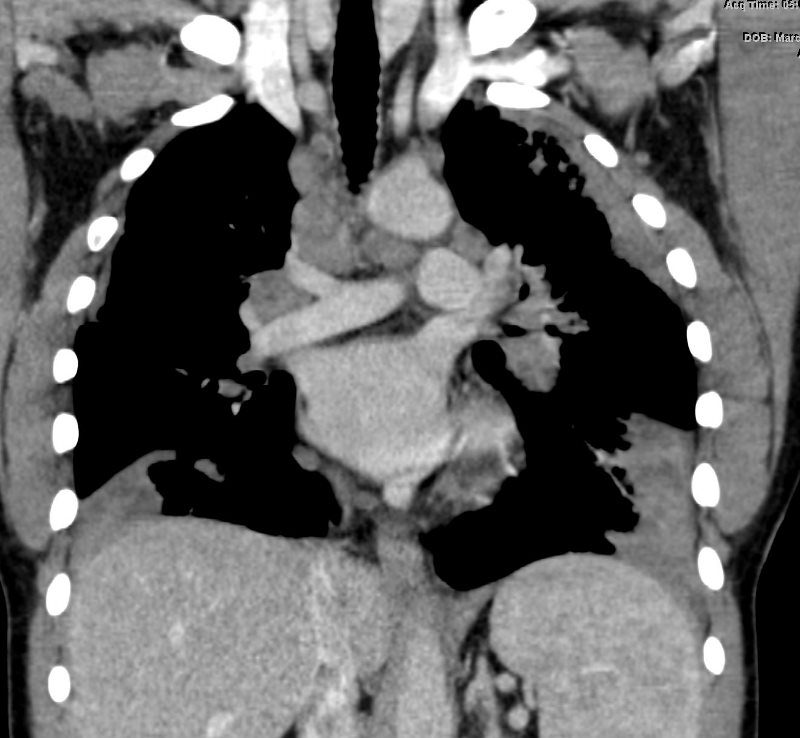 CT with MEDIASTINAL AND HILAR ADENOPATHY
CT with MEDIASTINAL AND HILAR ADENOPATHY
Pawnbroker’s Sign
Ashley Davidoff MD
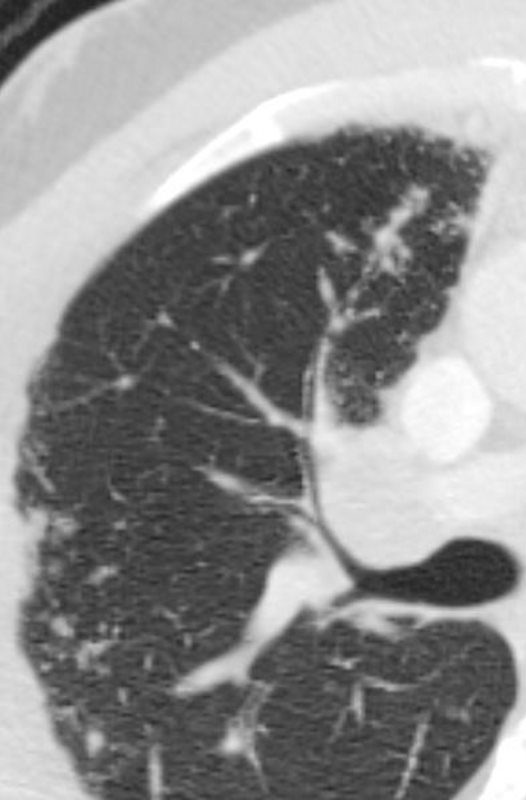
Micronodules, Nodules, Coalescence and the Galaxy Sign
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD
Ashley Davidoff MD

Thickening around the Airways
When the nodularity, clustering and or mass formation involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Ashley Davidoff MD
CT OF SARCOIDOSIS
GIF FILE
