
-
Causes
-
- Infection
- Viral
- COVID 19
-
-

COVID 19
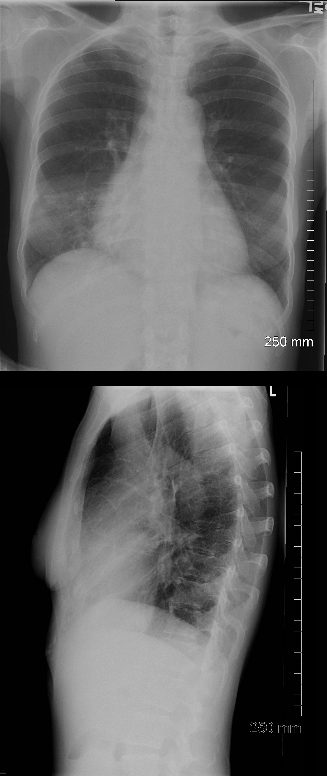
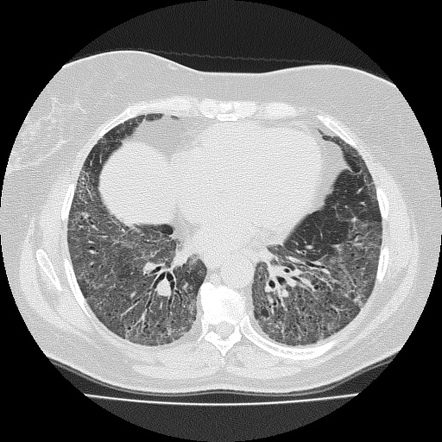
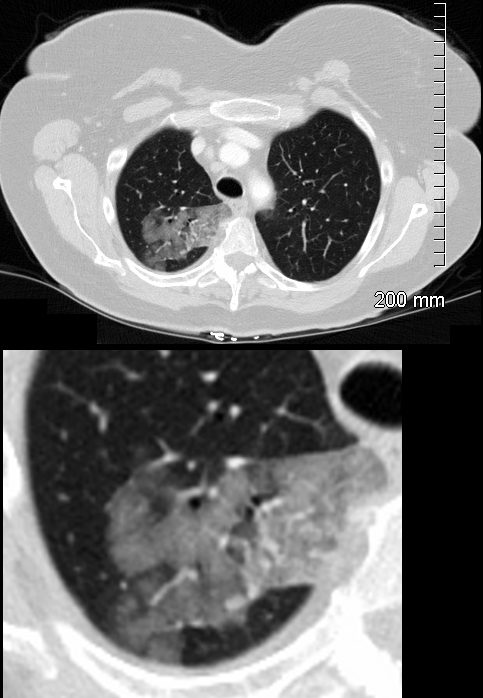
55-year-old male presents with a fever and a cough.
CXR findings reveal vague peripheral, bibasilar, “ground glass” changes in the lower lung zones.
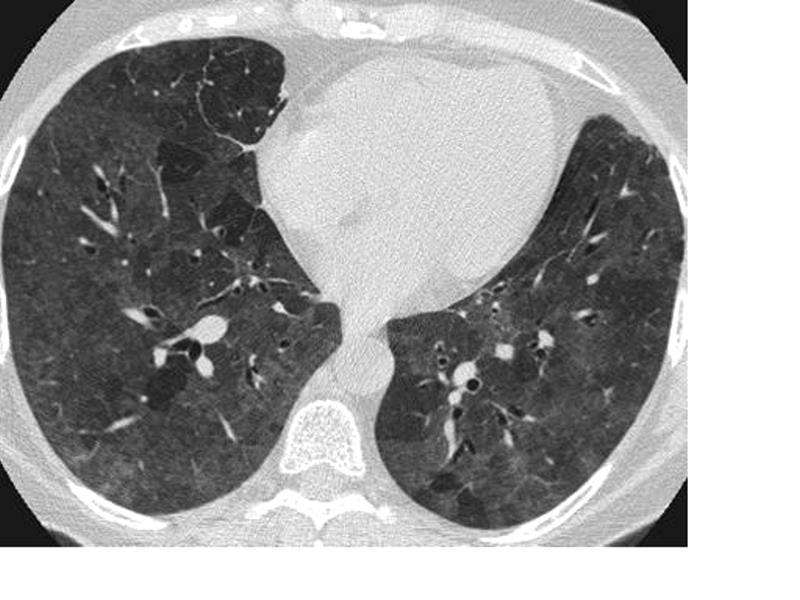
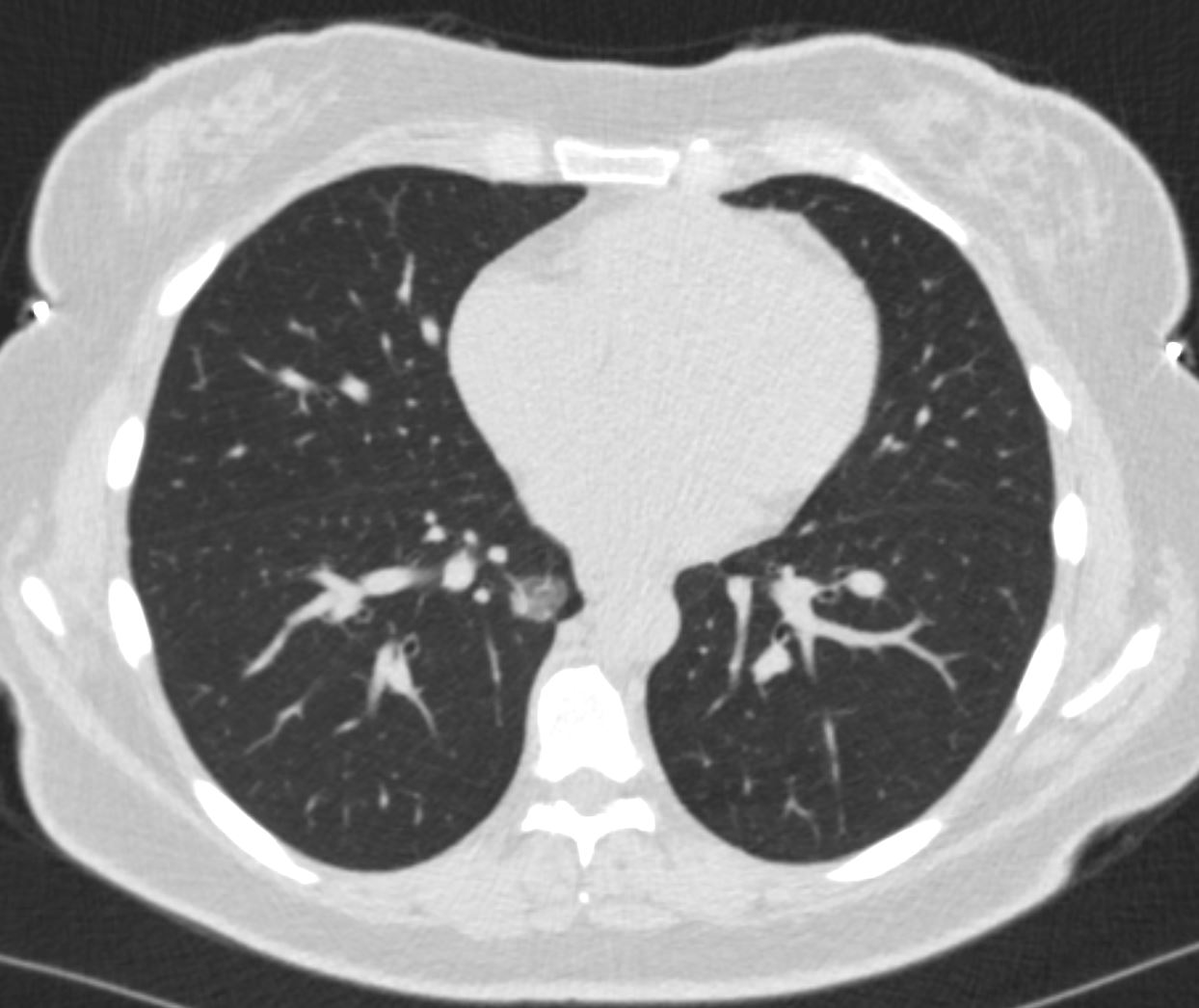
The CT scan confirms the presence of bilateral, predominantly basilar, nodular, and peripheral mixes ground glass and consolidative opacifications consistent with the diagnosis of COVID 19. Differential diagnosis however includes other viral pneumonias, allergic alveolitis and other multifocal and organizing pneumonias.
Courtesy Kevin Chang MD
TheCommonVein.net
-
-
- HIV Likely PCP
-
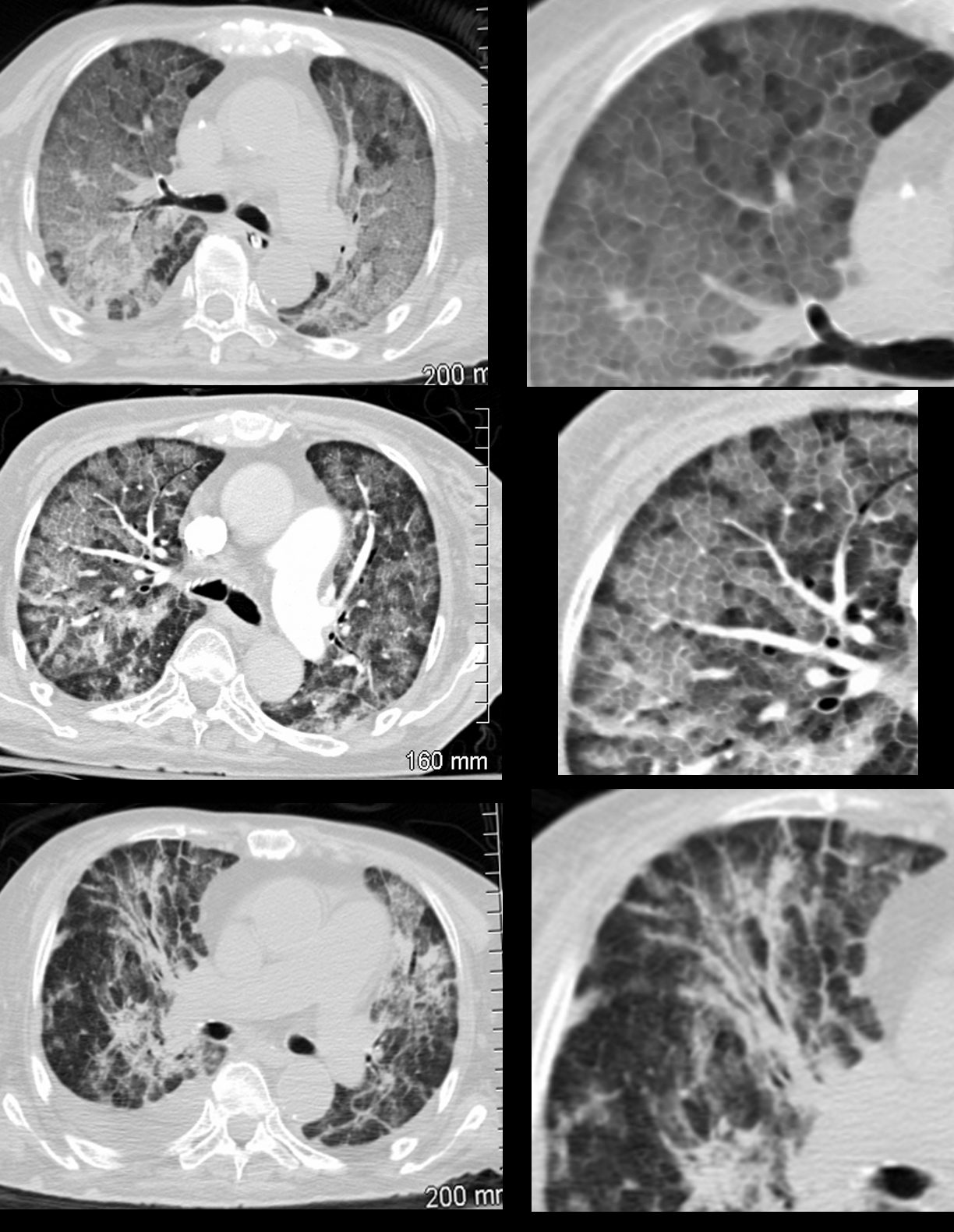
HIV and Diffuse ground Glass
36 year old female with HIV presents with dyspnea. CT scan on presentation (upper images) show extensive disease with crazy paving pattern. Following adjunctive steroid therapy, the patient showed early mild improvement with persistence of crazy paving, peripheral sparing and regions of improved aeration (middle panel). Continued improvement continued subsequently with improved aeration, minimal residual crazy paving and bronchovascular infiltrate ( lower panel).
Ashley Davidoff MD TheCommonVein.net 30755c -
HIV CMV
CMV – Multicentric Pneumonia
Cytomegalovirus pneumonia. CT scans in a 31-year-old woman with a history of type 1 diabetes mellitus complicated by end-stage renal disease. The patient had previously undergone kidney and pancreas transplant and presented with 2 days of right lower quadrant abdominal pain associated with nausea and vomiting. Upon further work-up, patient was found to have cytomegalovirus viremia. (above) Axial and (be;low) coronal CT images demonstrate diffuse randomly distributed small pulmonary nodules (arrows), many of which are ill-defined and distributed in the secondary pulmonary lobules and perilymphatic regions.
Parekh, M et al Review of the Chest CT Differential Diagnosis of Ground-Glass Opacities in the COVID Era Radiology Vol. 297, No. 3 July 2020CMV – Multicentric Pneumonia
Cytomegalovirus pneumonia. CT scans in a 31-year-old woman with a history of type 1 diabetes mellitus complicated by end-stage renal disease. The patient had previously undergone kidney and pancreas transplant and presented with 2 days of right lower quadrant abdominal pain associated with nausea and vomiting. Upon further work-up, patient was found to have cytomegalovirus viremia. (above) Axial and (be;low) coronal CT images demonstrate diffuse randomly distributed small pulmonary nodules (arrows), many of which are ill-defined and distributed in the secondary pulmonary lobules and perilymphatic regions.
Parekh, M et al Review of the Chest CT Differential Diagnosis of Ground-Glass Opacities in the COVID Era Radiology Vol. 297, No. 3 July 2020
-
- COVID 19
- Viral
- Inflammation
- Sarcoidosis
-
-
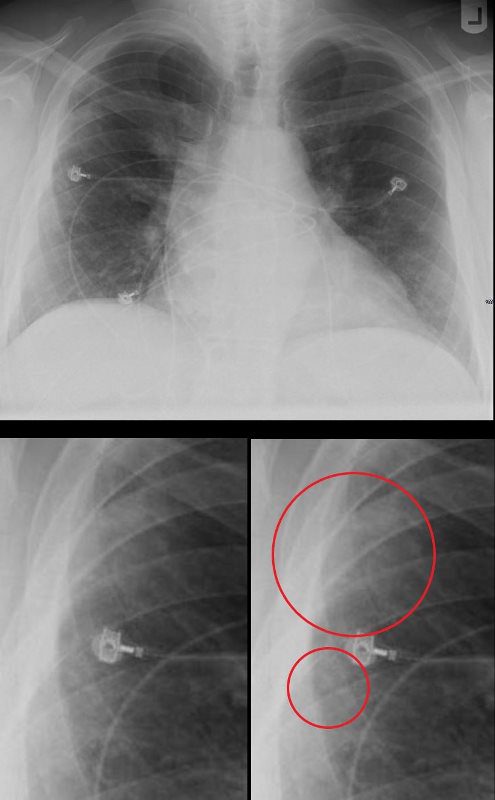
CXR FRONTAL
SARCOIDOSIS – CHARACTERISTIC NODULES
51-year-old male with history of sarcoidosis
The frontal CXR shows subtle nodular changes in the right upper peripheral lung field (red circles) and the lateral examination shows 3 regions of nodular changes (red arrowheads)
The CT examination scout film confirms 3 major regions of nodular change in the posterior and superior segment of the RUL along the confluence of the right major and minor fissure and in the posterior segment of the left upper lobe peripherally.
The axial images show a variety of characteristic changes including;
Ground glass opacity
Stellate or flame shaped nodules
Semisolid nodules
Fissural based nodules
Subpleural nodules
Micronodules along the
lymphovascular and
bronchovascular bundles of the secondary lobule
Calcified nodule some of which are surrounded by soft tissue of the granuloma
There are small calcified nodes in the mediastinum, but no significant pathological adenopathy
No obvious cardiac nor splenic involvement is noted
Ashley Davidoff MD
TheCommonVein.net
-
- Wegeners
-
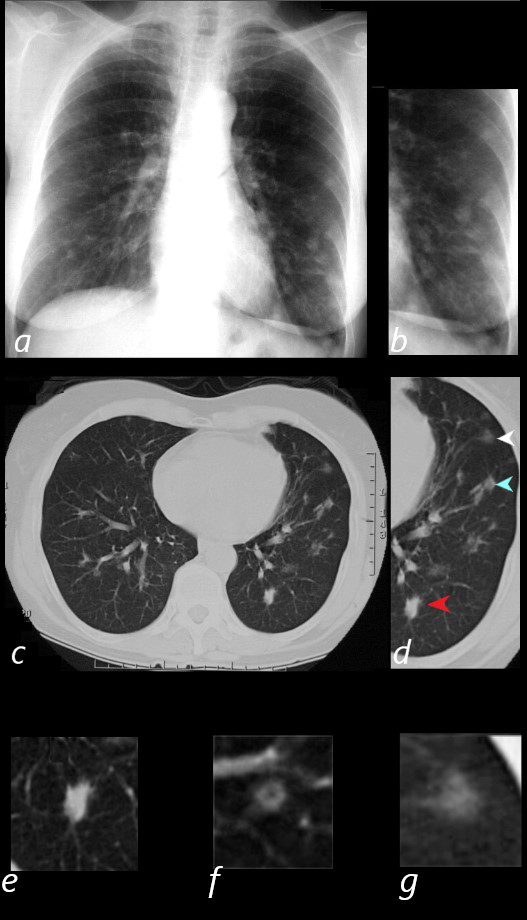
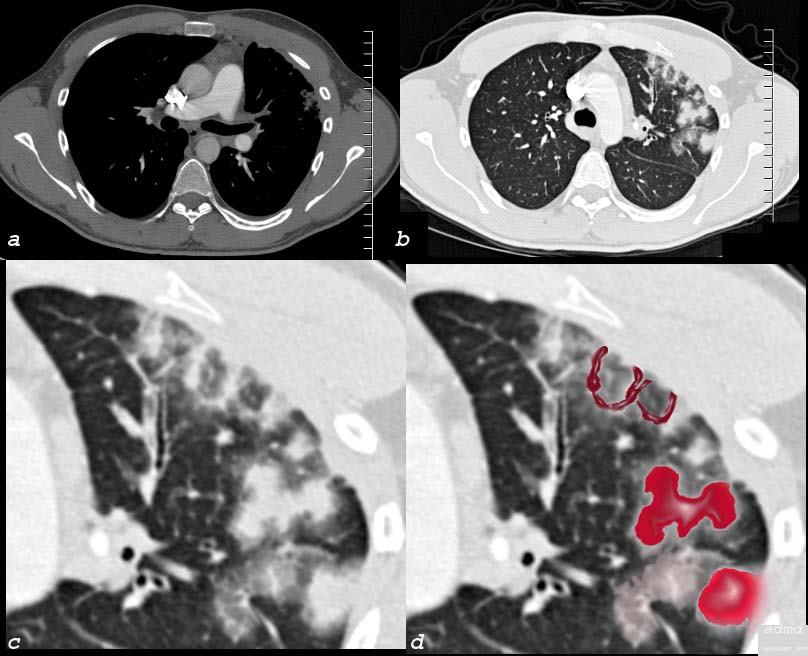
NODULES OF WEGENER”S GRANULOMATOSIS, aka GRANULOMATOSIS WITH POLYANGIITIS, GPA
65 year old female presents with epistaxis and with nodular changes on CXR (a) magnified in b.
CT scan in axial projection (c) and magnified in d, reveals 3 types of nodules.
A spiculated solid nodule (red arrow head) is magnified in e, a bronchocentric nodule (teal arrowhead) is magnified in e. This may represent a cavitating nodule or hemorrhagic change around a bronchiole (cheerio sign) A ground glass nodule (white arrowhead) is magnified in g.
Ashley Davidoff MD-
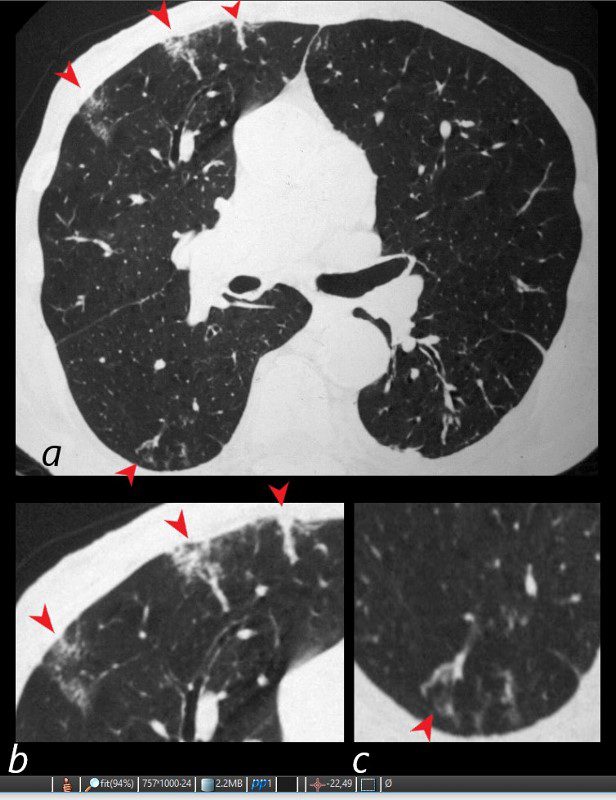
WEGENER’S GRANULOMATOSIS WITH POLYANGIITIS, GPA,VASCULITIS AND MICROINFARCTION
81-year-old male with weight loss, renal failure, and hemoptysis
CT axial view (a) shows multiple peripheral wedge shaped ground glass densities subtended by distended feeding vessels (a,b,c, red arrowheads) reflecting areas of microinfarction due to vasculitis that affects both the arterioles and venules.
Priscilla Slanetz MPH MD
TheCommonVein.net -
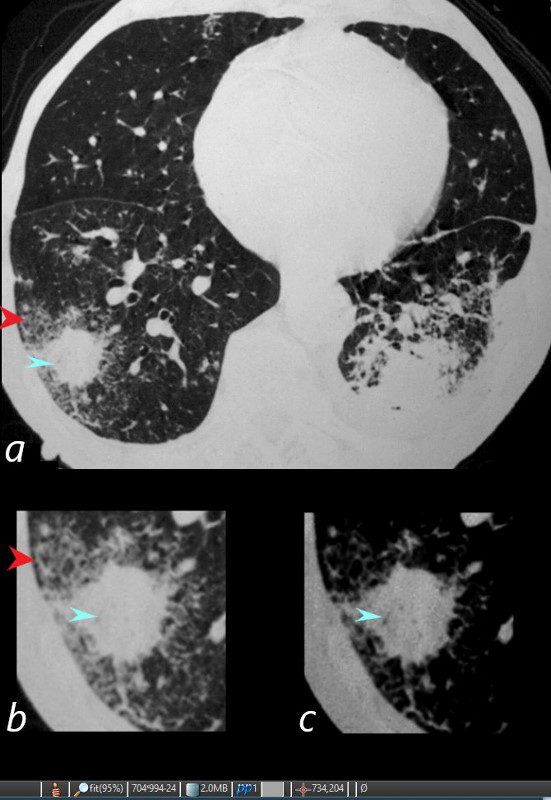
WEGENER’S GRANULOMATOSIS WITH POLYANGIITIS, GPA, HALO SIGN AND AIR BRONCHOGRAMS
81-year-old male with weight loss, renal failure, and hemoptysis
CT axial view (a) shows a 2 cm solid nodule in the RUL surrounded by A HALO SIGN OF GROUND GLASS CHANGES AND RETICULAR CHANGES (a,b, red arrowheads), indicating surrounding hemorrhage, and subtle air bronchograms (a,b,c, teal arrowheads) best appreciated in c with narrowed windows.
Priscilla Slanetz MPH MD -
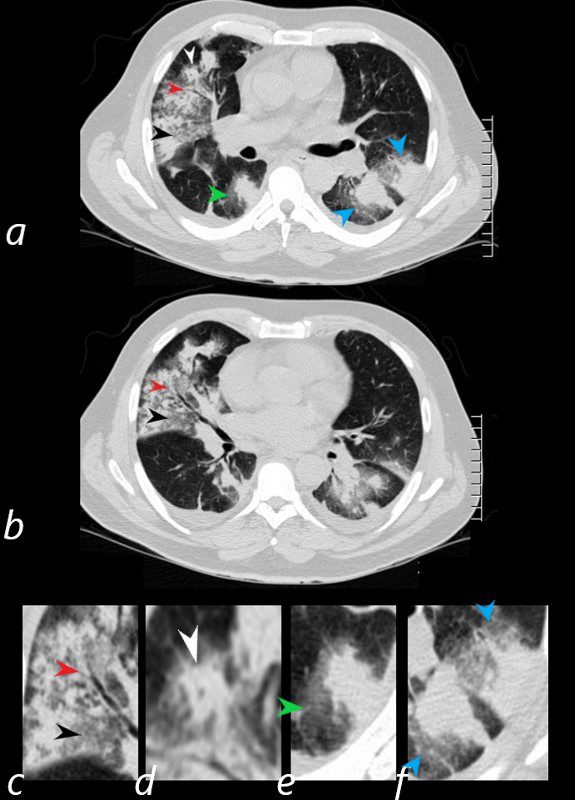
HEMORRHAGE, GROUND GLASS, HALO SIGN, AIR BRONCHOGRAM AND CHEERIO SIGN, WEGENER’S GRANULOMATOSIS WITH POLYANGIITIS, GPA.
57 year old male presents with a history of hemoptysis and dyspnea.
Axial CT scans show multicentric nodular consolidations with air bronchograms (red arrowheads a ,b, c), ground glass infiltrate (black arrowheads, a,b,c) halo sound around nodules and masses in the RLL (a,e, green arrowheads) and in the LLL 9a,f, blue arrowheads). Lastly there is a cheerio sign (a,d, white arrowheads) either representing granulomatous mass surrounding an airway, or central cavitation of a nodule.
Ashley Davidoff MD.
57 year old male presents with a history of hemoptysis and dyspnea.
Axial CT scans show multicentric nodular consolidations with air bronchograms (red arrowheads a ,b, c), ground glass infiltrate (black arrowheads, a,b,c) halo sound around nodules and masses in the RLL (a,e, green arrowheads) and in the LLL 9a,f, blue arrowheads). Lastly there is a cheerio sign (a,d, white arrowheads) either representing granulomatous mass surrounding an airway, or central cavitation of a nodule.
Ashley Davidoff MD TheCommonVein.net
-
-
- Immune
- SLE
-
ACUTE ALVEOLAR PNEUMONITIS
PA and lateral chest X-ray of a 54 year old female with SLE shows bibasilar ground glass infiltrates.
The heart is slightly enlarged and the region of the IVC on the lateral examination is also enlarged
Ashley Davidoff MD key word acute pneumonitis SLE-
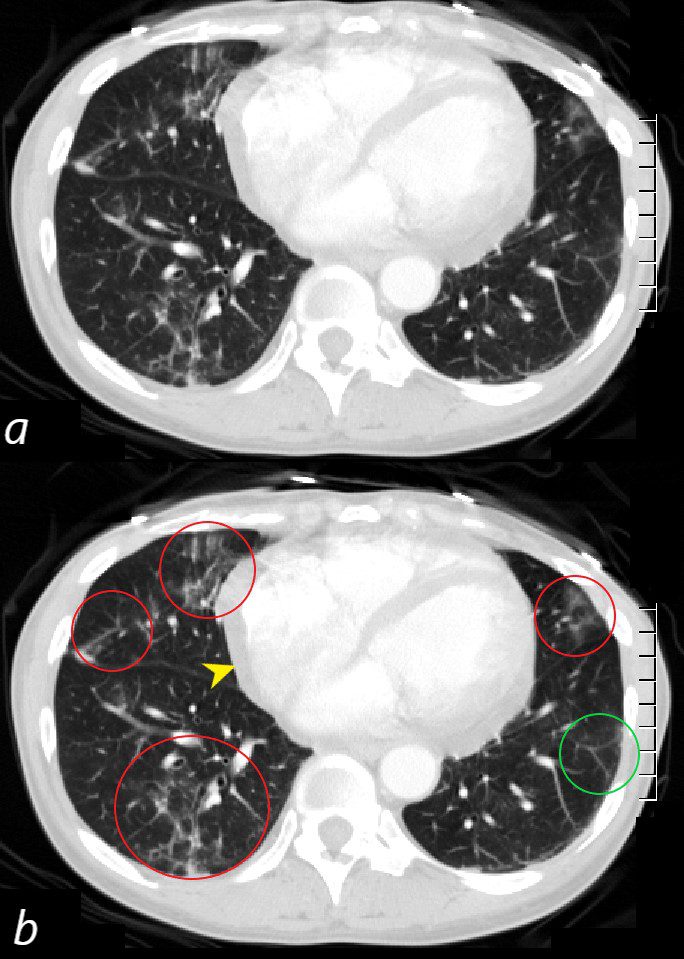
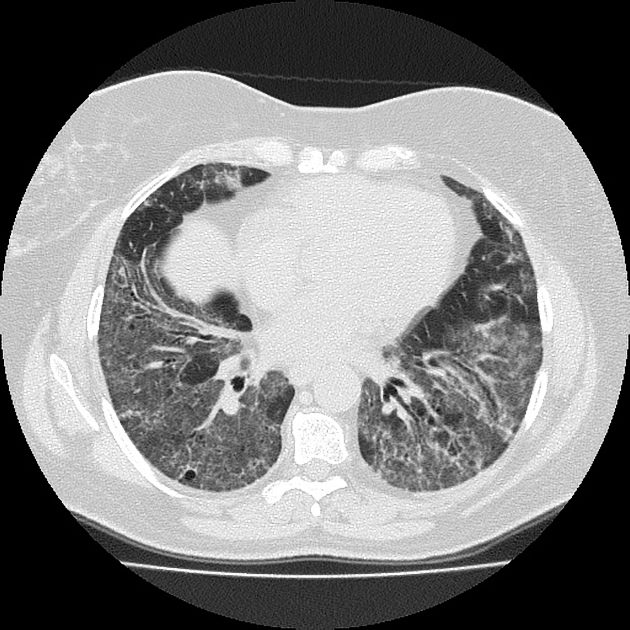
ACUTE ALVEOLAR PNEUMONITIS
CT scan through the 4 chambers of the heart using lung windows is from a a 54 year old female with SLE. Recent CXR showed bibasilar ground glass infiltrates.
The scan shows basilar multicentric infiltrates with elements of ground glass change and small airway wall thickening (red circles in the right lower lobe middle lobe and lingula, as well as interlobular septal thickening (green circle) in the lateral basal segment of the left lower lobe. A small pericardial effusion is present (yellow arrowhead)
Ashley Davidoff MD key words SLE acute pneumonitis pericardial effusionSLE and LUNG PARENCHYMA
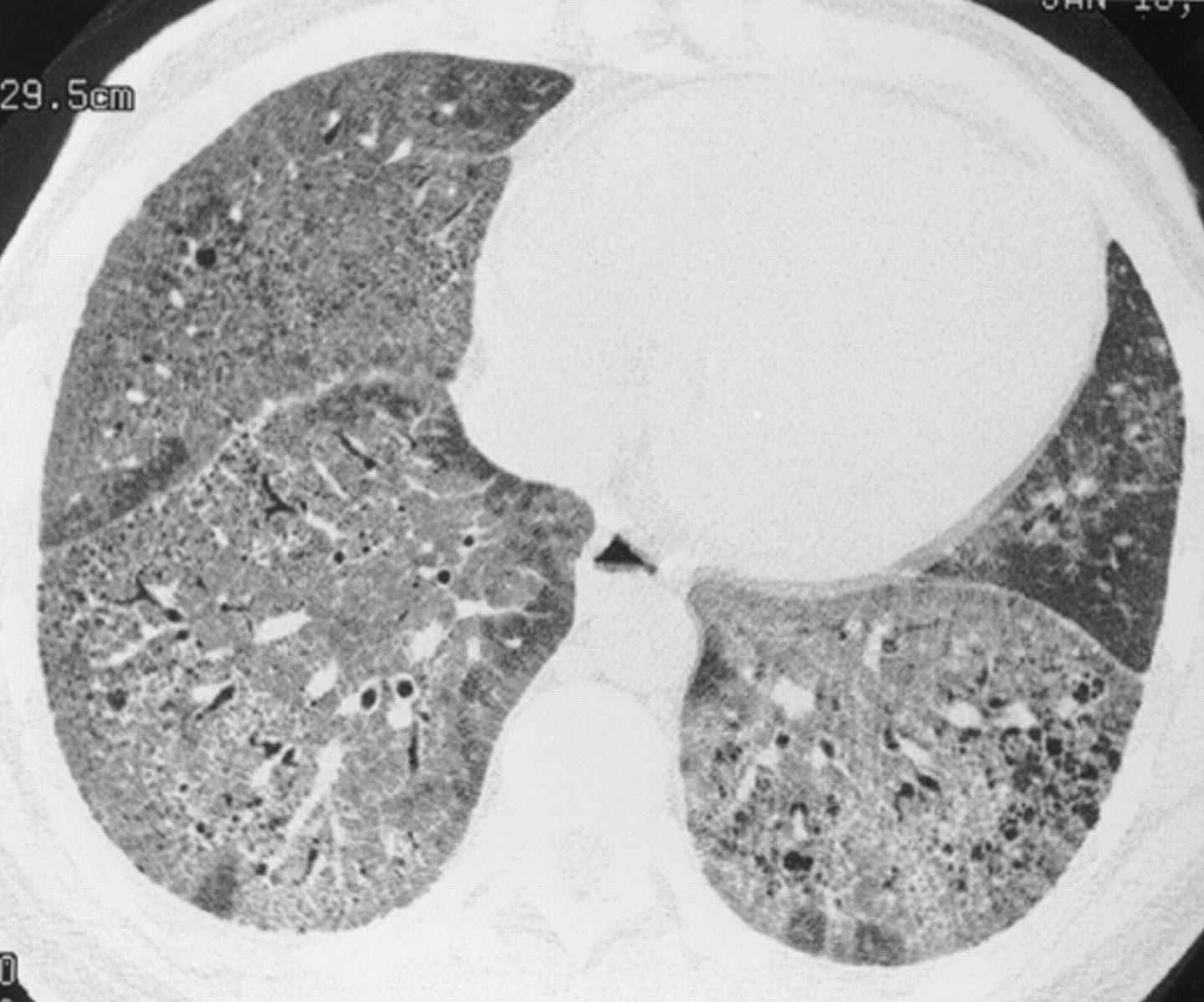
Chronic interstitial pneumonia in a 35 year old woman with SLE. HRCT scan shows extensive ground glass opacities admixed with coarse linear bands and honeycomb cysts. Open lung biopsy confirmed the diagnosis. Ground glass opacities represented a mixture of fibrosis and interstitial mononuclear cell infiltrates. Treatment with corticosteroids, azathioprine, and later cyclophosphamide failed and she subsequently underwent a single lung transplantation.
Keane et al Pleuropulmonary manifestations of systemic lupus erythematosus
BMJ Volume 55, Issue 2-
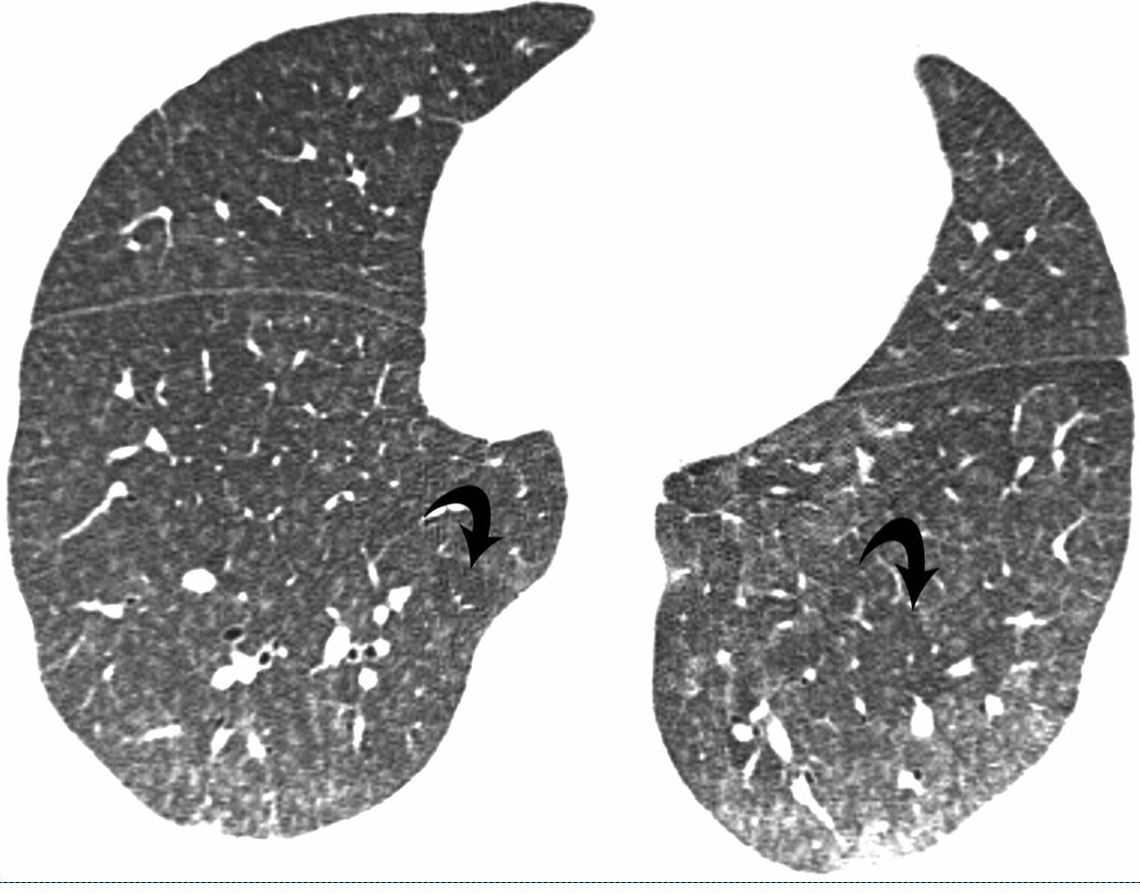
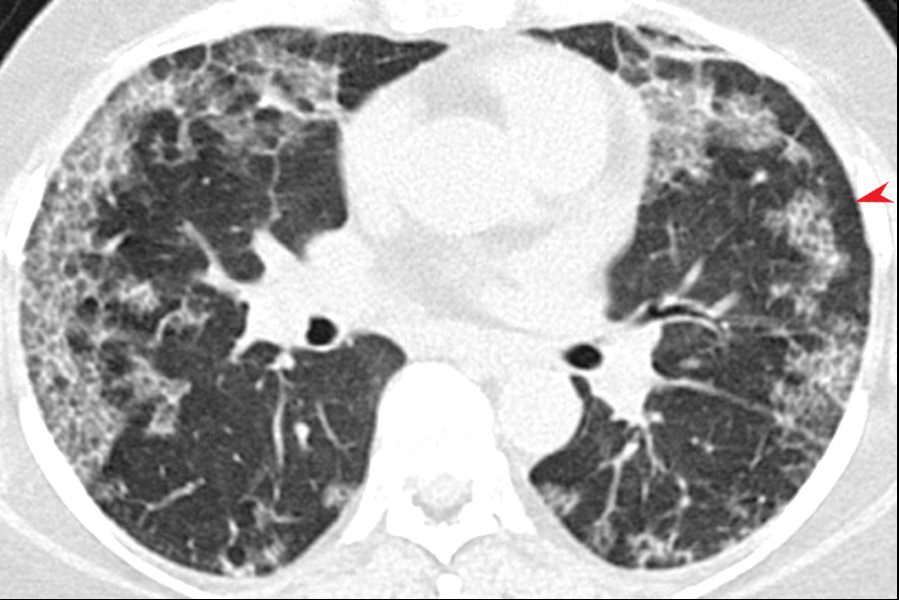
41-year-old man with subacute hypersensitivity pneumonitis. High-resolution CT image shows bilateral poorly defined centrilobular nodules and ground-glass opacities. Also evident are lobular areas (arrows) of decreased attenuation.
-
-
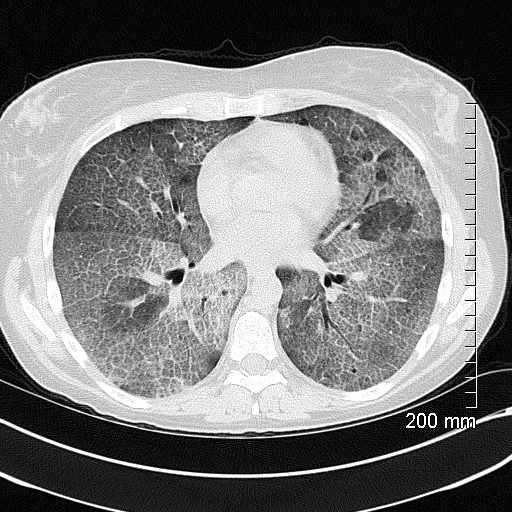
Hypersensitivity Pneumonitis ground Glass with Mosaic Attenuation
High-resolution CT: increase in density in areas of ground glass and air trapping in lower lobes in patients with hypersensitivity pneumonitis
Courtesy Mluisamtz11Accumulation of proteinaceous material in the alveoli, impairing gas exchange and leading to respiratory failure. Extensive thickening of interlobular septa leading to crazy paving appearance. Half filled alveoli lead to ground glass appearance
Ashley Davidoff TheCommonVein.net lungs-0738b
-
-
- Sarcoidosis
- Infection
-

Excellent example of crazy paving
Ashley Davidoff TheCommonVein.net 117625
-
-
-
-
- ILD
-
GROUND GLASS MORPHOLOGY IN ILD
Ground glassinfiltrates are one of the features of the interstitial disease with increased density without obscuring the airways and vessels
-
- NSIP
-
-
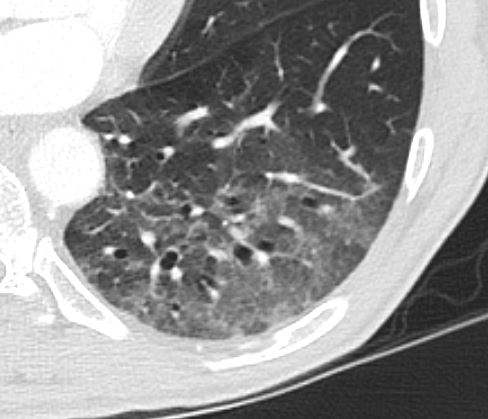
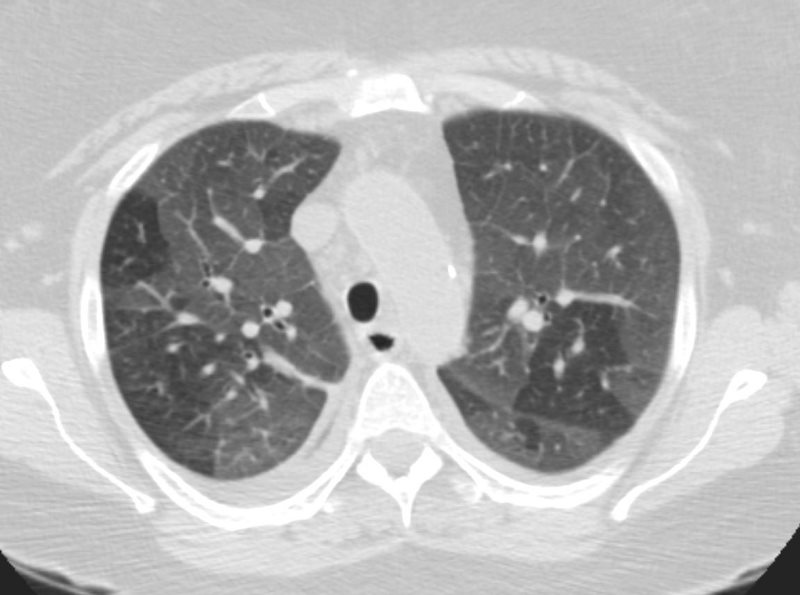
NSIP
CT scan through the lower lobes showing basilar ground glass opacification with peri bronchial thickening and traction bronchiectasis
Courtesy Pathology Outlines
http://www.pathologyoutlines.com/ -
NSIP
CT scan through the chest shows relatively symmetrical and peripherally positioned ground glass infiltrates with a region of subpleural sparing (red arrowhead)
Courtesy Pathology Outlines
http://www.pathologyoutlines.com/NSIP
CT scan through the lower lobes showing basilar ground glass opacification with peribronchial thickening and traction bronchiectasis
Courtesy pathology Outlines
http://www.pathologyoutlines.com/Ground glass bronchiectasis and bronchiolectasis and question subpleural sparing 58M probable NSIP
Ashley Davidoff TheCommonVein.netGround glass bronchiectasis and bronchiolectasis and question subpleural sparing 58M probable NSIP
Ashley Davidoff TheCommonVein.net
-
-
- ILD
-
- Neoplasm
-
41F adenocarcinoma lepidic growth 008 3mths later
Ashley Davidoff
TheCommonVein.net -

Single Focus of Ground Glass Opacity without Solid Elements
Ground glass opacity in the secondary lobule reflects alveolar process and is one of the presenting appearances of unifocal or multifocal BAC. It is a slow growing in situ disease that may not change in size over two years, but continued surveillance is necessary.
Courtesy: Ashley Davidoff, M.D
Multicentric BAC and Adenocarcinoma
The CT is from a 51-year-old male who is a smoker, who shows a ground glass opacity (GGO), mixed with a solid mass (arrow in (a) and multicentric BAC in a lower cut (b), characterised by three areas in the right lower lobe of partial alveolar opacification. Ground glass appearance is the result of partial opacification of the alveoli. Two of the GGOs measure close to 2 cm each and the third more anterior measures about 8mm. In this instance, a PET scan was positive in the area (green ring in d). It is likely that the solid component in image a represents the transformation of BAC – (really a carcinoma in situ) into adenocarcinoma.
Courtesy: Ashley Davidoff, M.D.87755.8s The CT is from a 51 year old male who is a smoker who shows three areas areas of ground glass opacity in the right lower lobe, two that measure close to 2cms each and a third more anterior that measures about 8mms. This case represents multicetric BAC.(now known as adenocarcinoma with lepidic growth) lung cancer GGO ground glass opacity multicentric malignant BAC bronchioloalveolar carcinoma bronchiolocarcinoma CTscan Courtesy Ashley Davidoff MD TheCommonVein.net
-
- Circulatory
-
CHF
-
-
DIFFUSE GROUND DISEASE WITH REGIONS OF NORMAL LUNG
CHF, INTERSTITIAL EDEMA KERLEY A and B
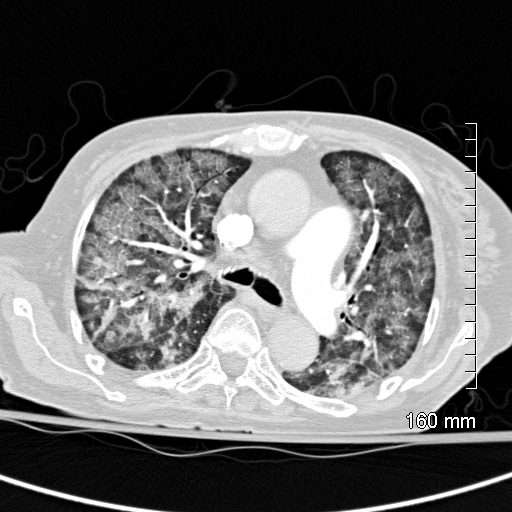
Ashley Davidoff MD TheCommonVein.netCHF – Alveolar Edema
CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern
Ashley Davidoff MD TheCommonVein.net 131742Hemorrhage
-
-
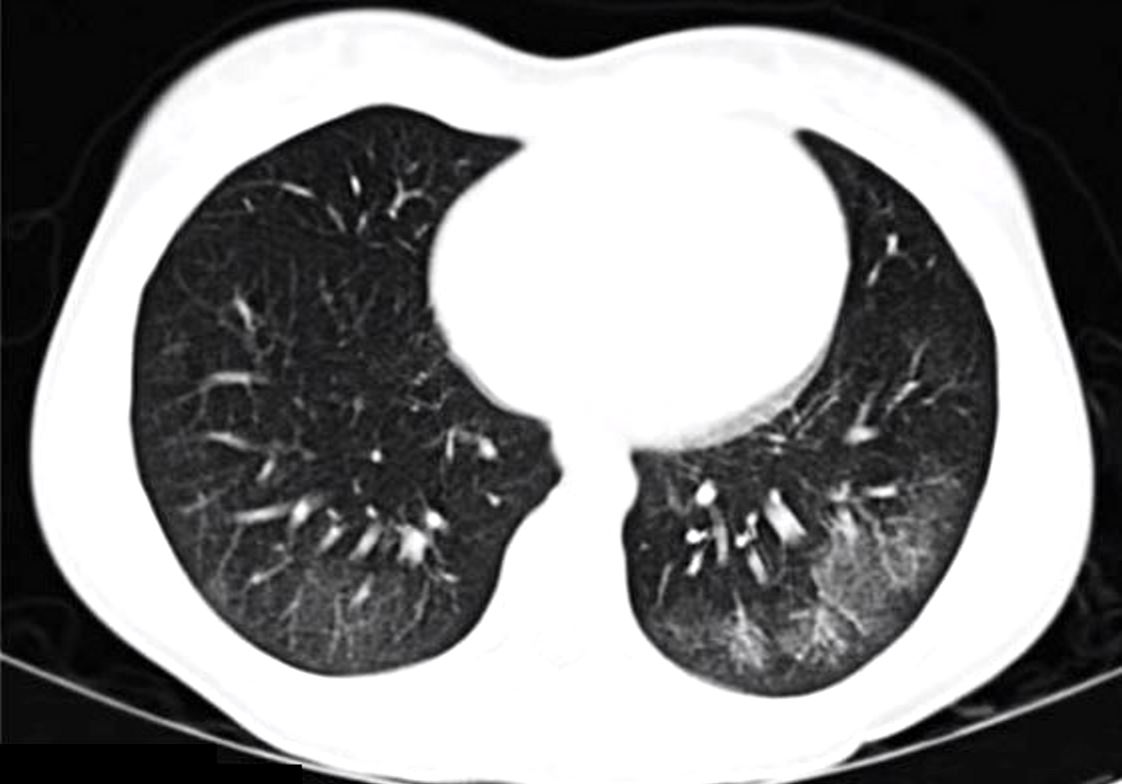
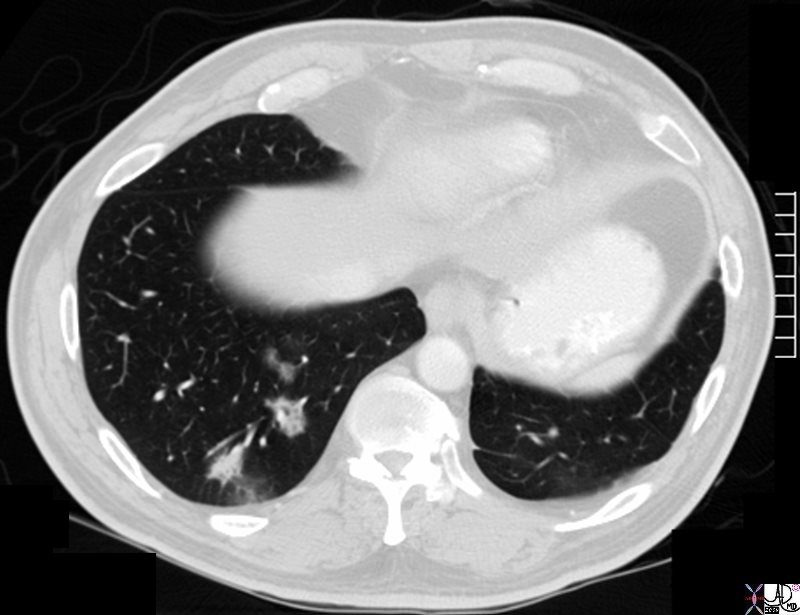
60 year old female who presents with hemoptysis. Ct scan shows a focal region of ground glass change in the superior segment of the left lower lobe, abutting the fissure, likely reflecting hemorrhage
Ashley Davidoff MD TheCommonVein.netCongestion
-
-
26 male SOB s/p RFA ablation for atrial fibrillation lung pulmonary let upper lobe pulmonary vein thrombosed secondary lobule interlobular septa are thickened secondary lobuledueto congestion and hemorrhage dx pulmonary vein thrombosis secondary to radiofrequency ablation therapy iatrogenic CTscan Courtesy Ashley Davidoff MD Scott Tsai MD ground glass changes pulmonary infarction venous infarction
TheCommonVein.net - Idiopathic
- Systemic Disease
-
-


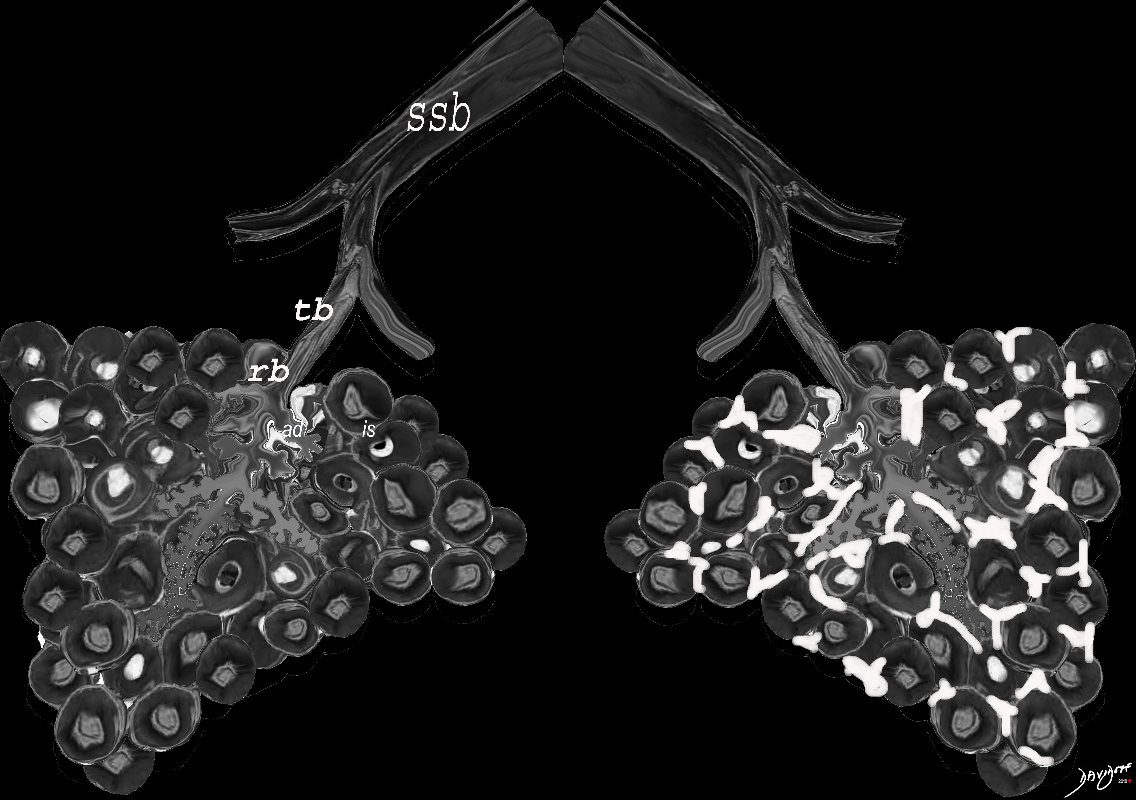
- Ground Glass as a result of Interstitial Disease –
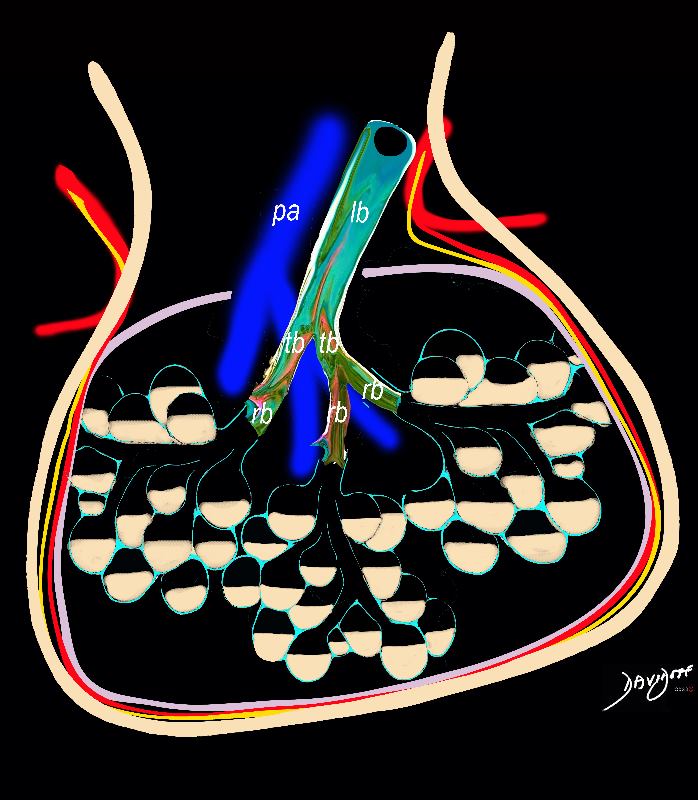
When there are extensive interstitial fibrotic changes in the interstitial compartments of the lung which include the and the interalveolar septa, and the supporting interstitium of the lung between the acini and small airways, the overall net density of the region of involvement will be gray, and when adjacent to the black air filled airways, a ground glass appearance will be apparent
Ashley Davidoff
TheCommonVein.net
ssb = subsegmental bronchiole
tb = terminal bronchiole
rb = respiratory bronchiole
as = alveolar duct
as = alvelar sac
is = anteralveolar septum
lungs-00682-lo res - Disease in the airways
- alveoli
- interalveoalar septa
- interstitium
-
Links and References
- TCV