
Left Upper Lobe Atelectasis Luftsichel Sign

Left Upper Lobe Atelectasis
Female patient with central squamous cell carcinoma of the lung with left upper lobe collapse and hyperinflation of the left lower lobe resulting in a Luftsichel sign
Ashley Davidoff MD TheCommonVein.net 152Lu

Left Upper Lobe Atelectasis
Female patient with central squamous cell carcinoma of the lung with left upper lobe collapse and hyperinflation of the left lower lobe resulting in a Luftsichel sign
Ashley Davidoff MD TheCommonVein.net 152Lu
The Lucent Apex, Ill Defined (Luftsichel Sign ) Consolidation/Atelectasis, and the Relatively Lucent periphery of the Consolidation
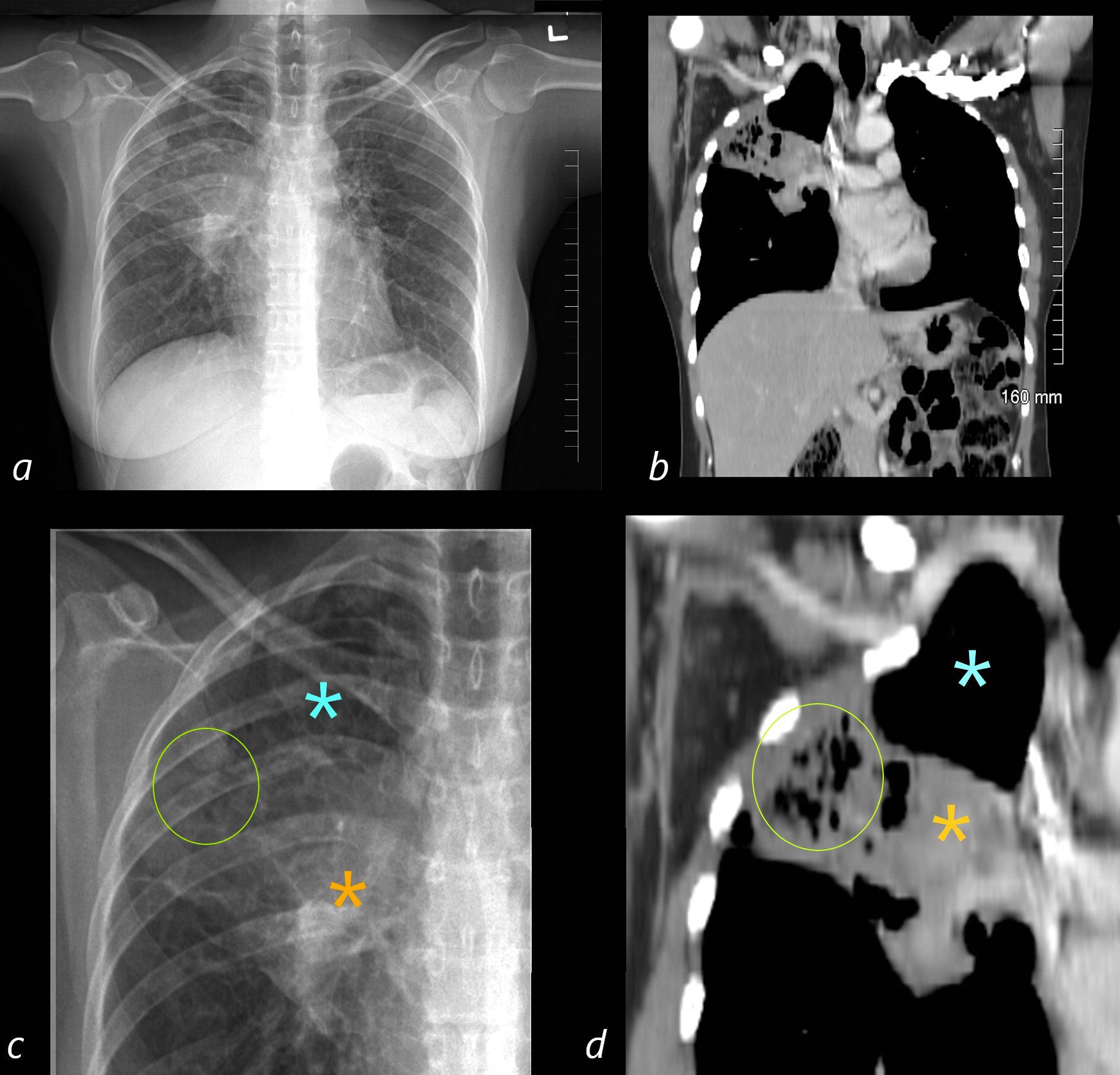
50 year old female with a history of asthma represents with productive cough.
The ill defined atelectasis in the RUL.
The CXR in the PA projection (a ) shows an ill defined density in the right upper lobe of the lung, with a relatively lucent right apex (blue asterisk in c ) . This image aims to explain the radiological findings integrating the appearance on the CXR and the appearance on CT
Why a lucent apex on CXR?
There is almost complete right upper lobe collapse seen on subsequent CT imaging and the lucent apex (blue asterisk on the magnified view of the CXR, c) correlates with the lucent hyperinflated RLL which reaches to the apex (blue asterisk on the magnified view of the CT, d also see image135097)
Why a lucent periphery of the consolidation?
In the periphery of the atelectatic right upper lobe there are aerated bronchiectatic airways circumscribed with green circle in the magnified view of the chest (c) and confirmed on the CT (green circle d). The overall lucency of this region reflects a relatively low density rather than the expected soft tissue density of the atelectasis
The soft tissue density medially?
The medial aspect of the atelectasis is consolidated and hence displays the characteristic soft tissue density in the magnified view of the CXR (orange asterisk c) and similarly on the CT (orange asterisk d)Ashley Davidoff MD TheCommonVein.net
“Partial Luftsichel Sign”
Frontal CXR in a Patient with Central Carcinoid Tumor Obstruction of the Lingular Airways and Lingular Atelectasis with Correlative Sagittal CT to Explain the Findings in the Left Apex
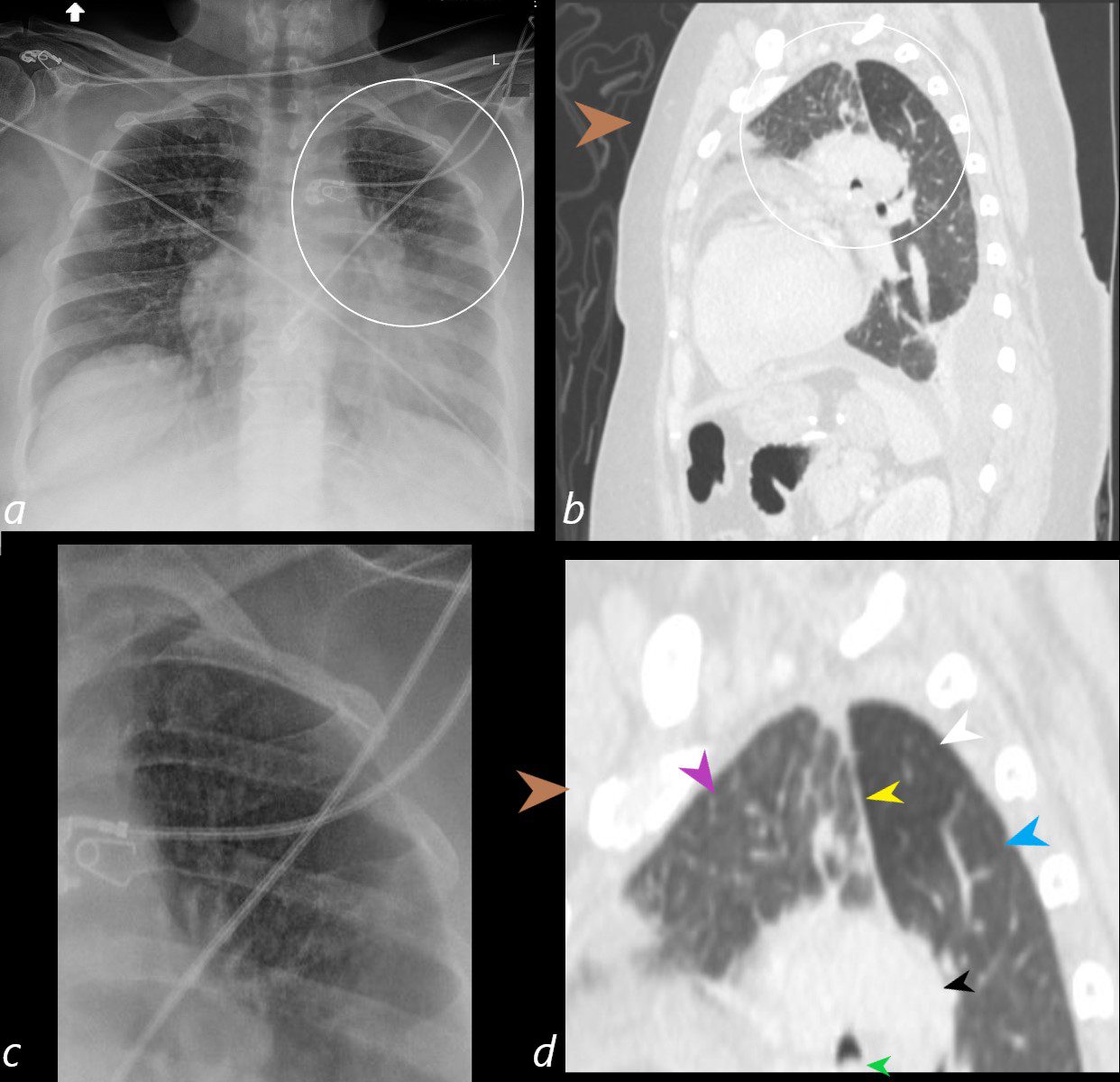
58-year-old female presents with a cough Frontal CXR shows silhouetting of the left heart border with hazy or veiling opacity extending out from the left hilum and fading out inferiorly. The left apex (ringed in white, a, and magnified in c) is lucent and reflects a combination of the normal aerated left upper lobe segments and the hyperinflated left lower lobe as explained in the sagittal correlates (b and d) The aerated left upper lobe segments are anterior (purple arrowhead d) and are separated by the superiorly and anteriorly displaced major fissure (yellow arrowhead). The left lower lobe is superiorly displaced and consists of a focally hyperinflated apical subsegment (white arrowhead), and other apical and lower lobe segments (light blue arrowhead). The central portion of the atelectatic lingula is noted (black arrowhead) and just a subtle hint of the tumor in the left mainstem bronchus is appreciated (green arrowhead)
Ashley Davidoff MD TheCommonVein.net 257Lu 136109c02L
The word Luftsichel is German for “air crescent.” The finding is seen in the setting of left upper lobe collapse. Due to the absence of a minor fissure on the left, as the left upper lobe collapses, the major fissure assumes a vertical position roughly parallel to the anterior chest wall.4 As volume loss progresses, the fissure continues to migrate more anteriorly and medially until the atelectatic lobe is contiguous with the left heart border, effectively obliterating its contour on the frontal radiograph (Figs. 17A–C). With movement of the apical upper lobe segment anteromedially, the superior segment of the left lower lobe hyperinflates and fills the vacated apical space.4,52 Occasionally this segment will insinuate itself between the aortic arch and the collapsed left upper lobe creating a sharp outline, or periaortic lucency, described as the Luftsichel.3,4,52