Pathology of Lymphangitis Carcinomatosis in the Right Upper Lobe
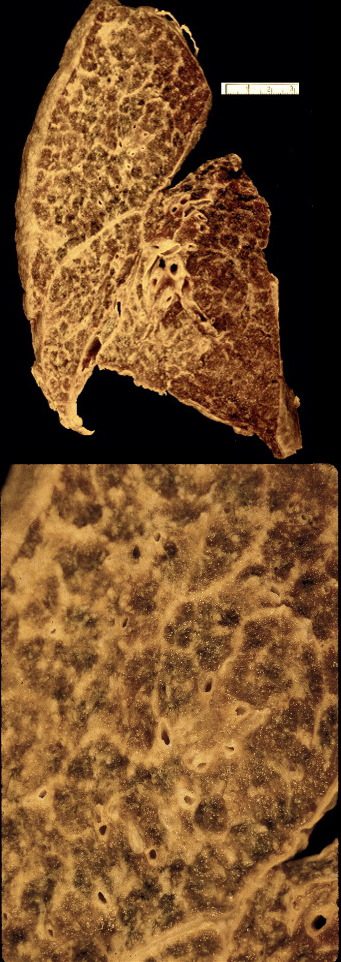
Gross pathology specimen in the coronal plane of the right lung shows extensive irregular thickening of the interlobular septa secondary to lung cancer and lymphangitis carcinomatosis
Ashley Davidoff MD TheCommonVein.net 32326c01
Ashley Davidoff MD
TheCommonVein.net
32199cw
keywords
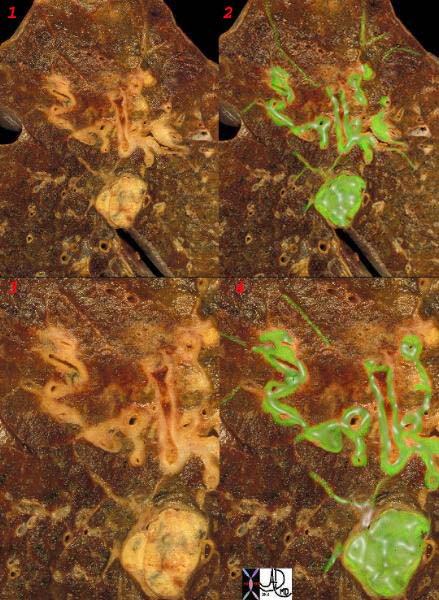
lungs pulmonary parenchymal mass neoplasm primary lymphatics distended metastases lymphangitis gross pathology
Ashley Davidoff MD
TheCommonVein.net
32226c1
keywords
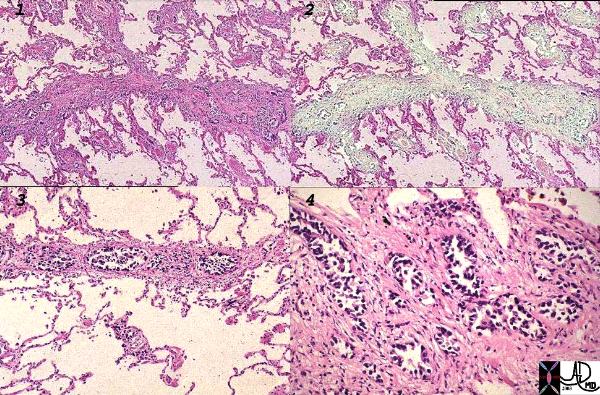
lungs pulmonary neoplasm primary prostate lymphatics distended metastases lymphangitis histopathology
Ashley Davidoff MD
TheCommonVein.net
32269b see 680249
keywords
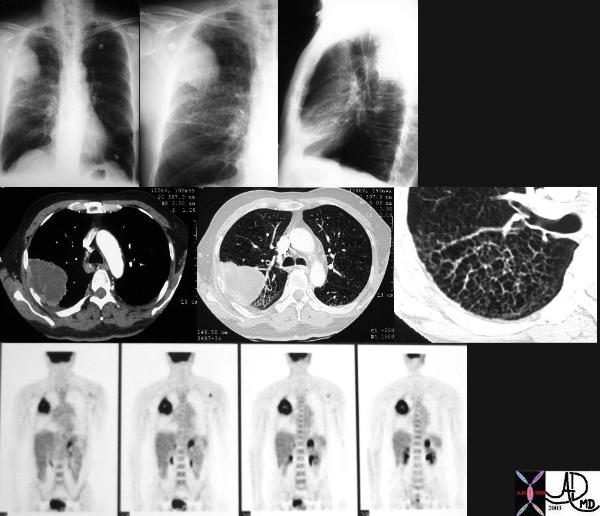
lungs pulmonary mass RUL neoplasm malignant primary lymphatics lymphangitis imaging plain film CXR CTscan PETscan

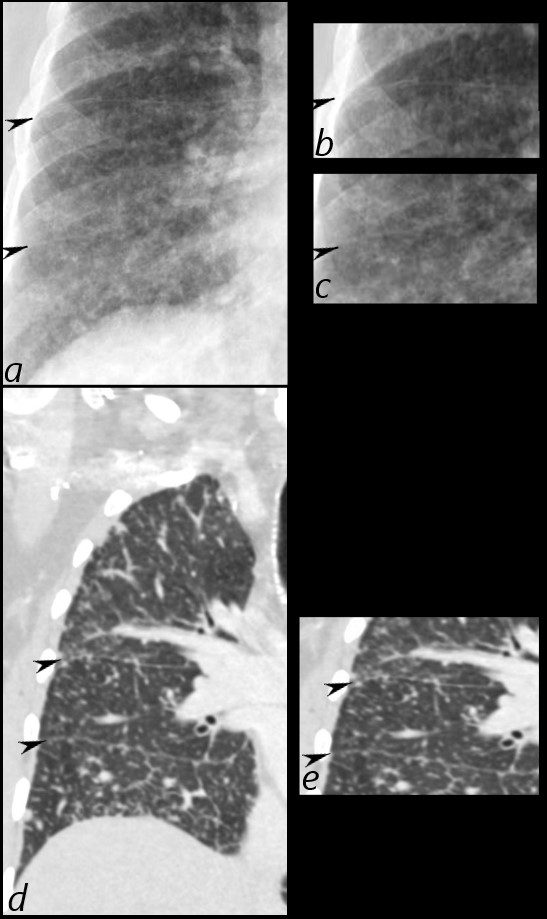
The CT scan of the centrally positioned small cell carcinoma has structural implication as a result of its central location close to large arteries, veins, airways and lymphatics. In this case the centrally placed tumor (dark green in image b) is pushing on the right mainstem bronchus (shown with white arrow) and the lymphatics with peribronchial thickening (image d light green) and extension into the interlobular septa (bright green in d) Subcarinal nodal involvement and left hilar involvement (light green in b)together with small right effusion (a,b) are also noted suggesting advanced disease.
Ashley Davidoff
TheCommonVein.net
87711c01.8s
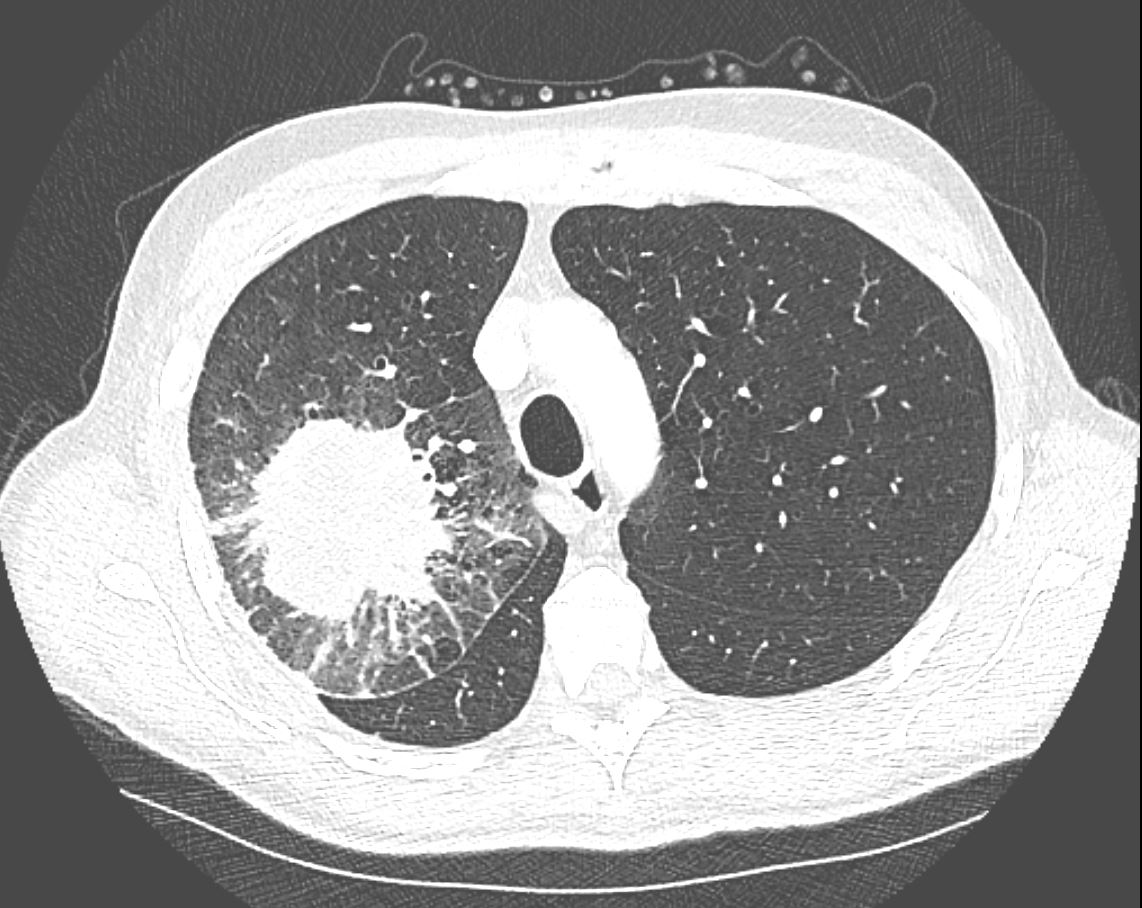
CT in the axial plane demonstrates a large, spiculated mass in the right upper lobe with surrounding halo likely reflecting hemorrhage or lymphatic edema around the mass. In addition, there is evidence of irregular interlobular septal thickening likely reflecting lymphatic invasion and indicating lymphangitis carcinomatosa. There is irregular thickening of the major fissure suggesting involvement.
Ashley Davidoff MD TheCommonVein.net 135865
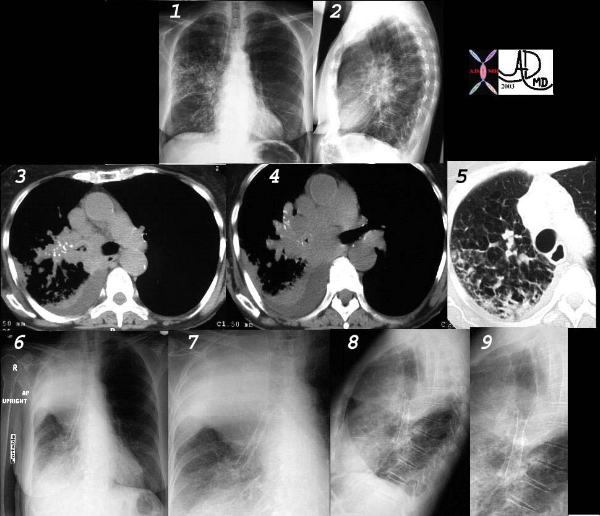
This collage of CT and plain film represents the radiological history of a patient with poorly differentiated small cell carcinoma, with extensive parenchymal involvement of the RUL and RML, and of the airways of RML and RLL. Images 1 and 2 show an interstitial and pneumonic pattern which was persistent over time. The CT shows extensive endobronchial disease involving right main stem (3,4) as well as almost all segments of RLL. This was confirmed by bronchoscopy.
Lymphangitic disease seems to be the dominant finding in the RUL on the lung windows. (5).
Following stent placement through a “pinhole” lesion, the patient occluded the RUL airways with tracheal shift and hyperinflation of the left lung (6,7,8,9). Clinically however, she improved greatly.
Courtesy Ashley Davidoff MD.
TheCommonVein.net
32426cl

Courtesy Ashley Davidoff MD.
TheCommonVein.net
32426_02cl
Courtesy Ashley Davidoff MD.
TheCommonVein.net
32426_03cl keywords
lung bronchus lyphatic infiltrate mass obstruction atelectasis thickening interlobular septa neoplasm malignant primary malignancy small cell carcinoma imaging radiology CTscan
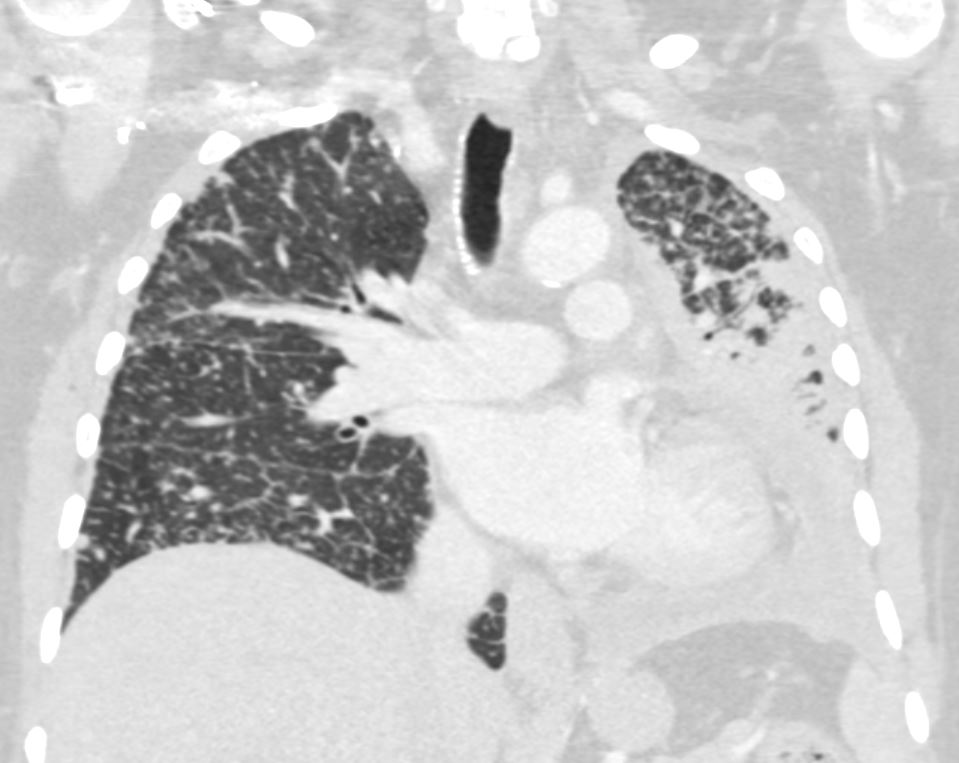
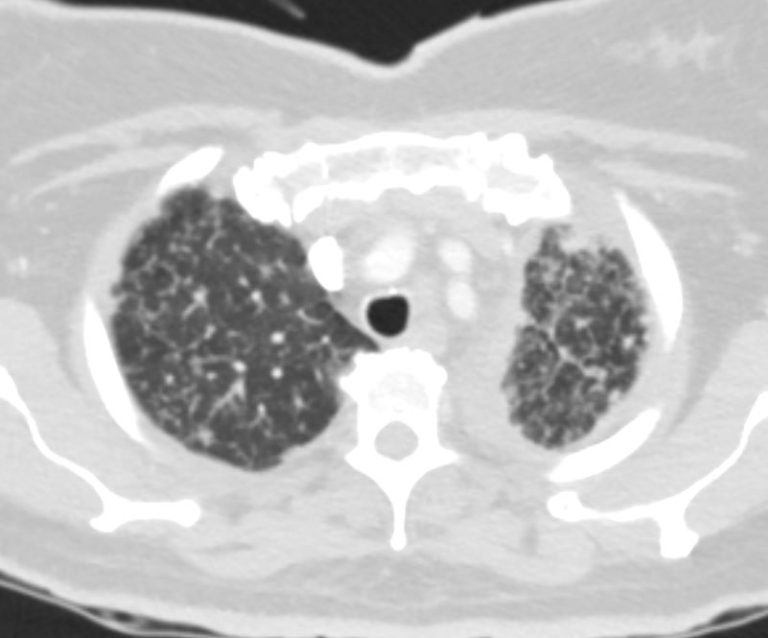
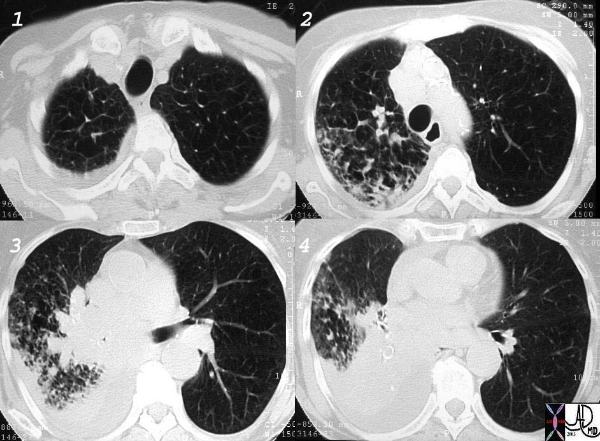
Bilateral Lymphangitis Carcinomatosis in a Patient with Adenocarcinoma

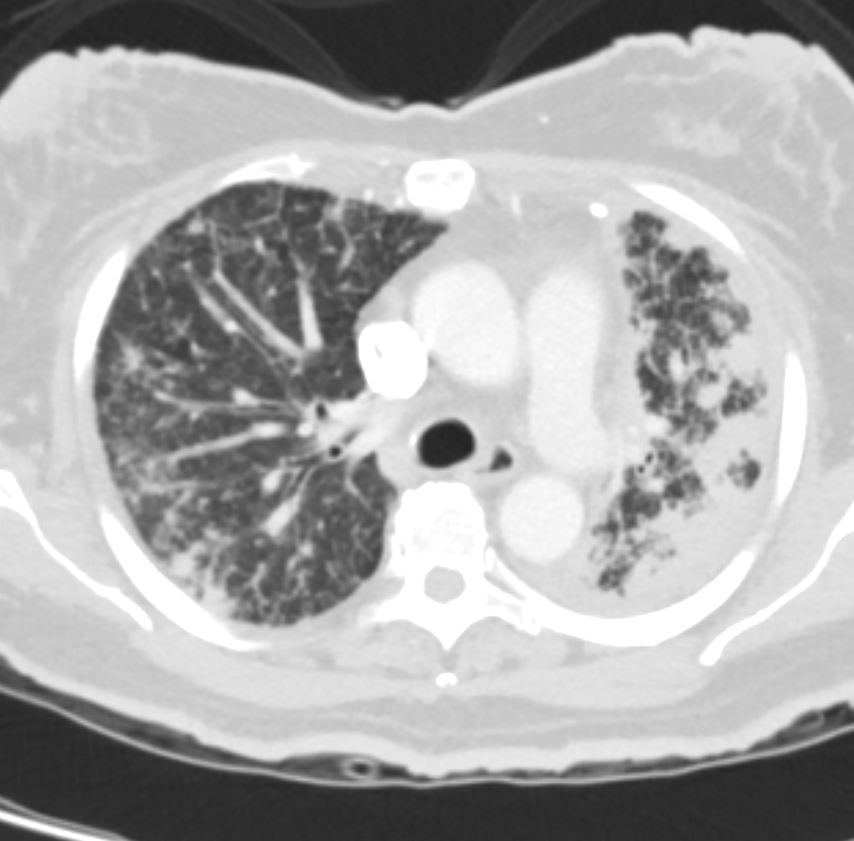
50 year old female with primary adenocarcinoma of the left lung with diffuse bilateral lymphangitic spread of disease characterized by lymphovascular distribution.
The nodularity on the fissures characterize the lymphatic distribution and the nodules are likely of a mixed nature, some being in the interlobular septa, and some in a centrilobular distribution .
Ashley Davidoff MD
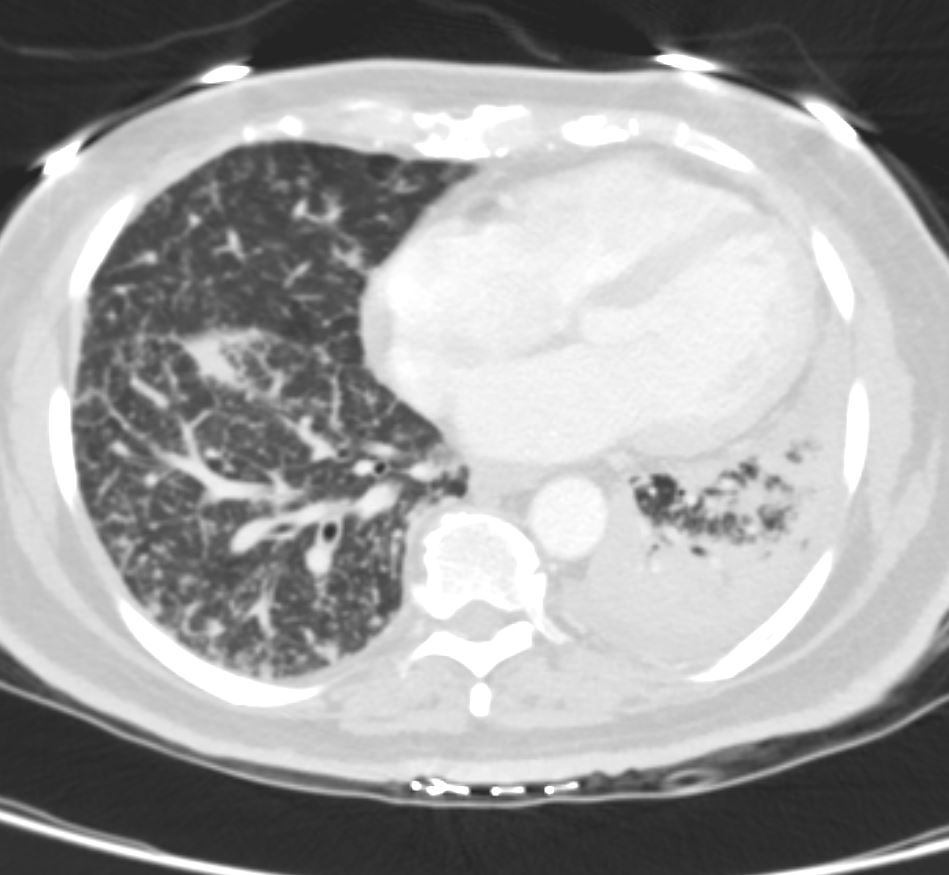
50 year old female with primary adenocarcinoma of the left lung with diffuse bilateral lymphangitic spread of disease characterized by lymphovascular distribution.
The nodularity on the fissures characterize the lymphatic distribution and the nodules are likely of a mixed nature, some being in the interlobular septa, and some in a centrilobular distribution .
Ashley Davidoff MD