
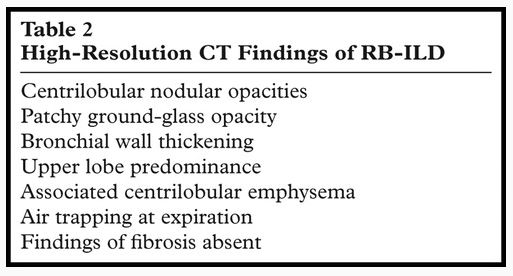
- Buzz words
- Respiratory bronchiolitis
- All smokers
- Usually symptomatic and no clinical significance
- Respiratory bronchiolitis ILD
- <common
- little fibrosis
- improves with cessation
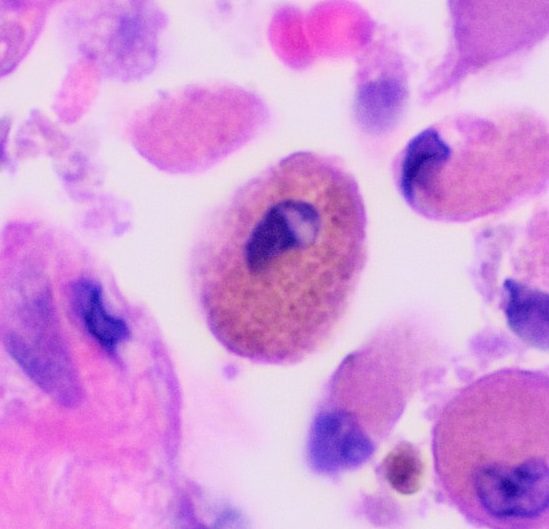
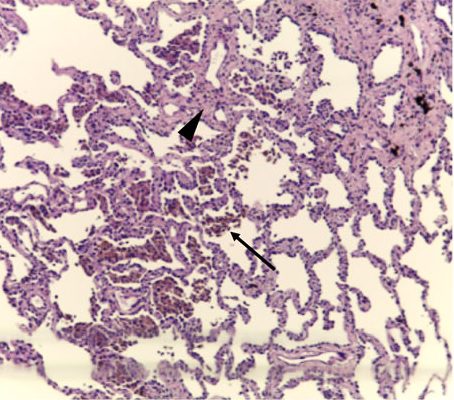
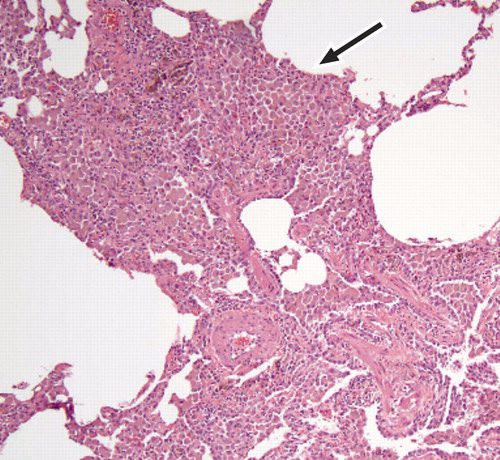
- macrophages
- accumulation of yellow-brown pigmented
- within the lumens of
- respiratory bronchioles and
- alveolar ducts, associated with a
- patchy submucosal and
- peribronchiolar chronic inflammation.
- mild bronchiolar and peribronchiolar alveolar fibrosis that expands contiguous alveolar septa and leads to architectural distortion as well as centrilobular emphysema.
-

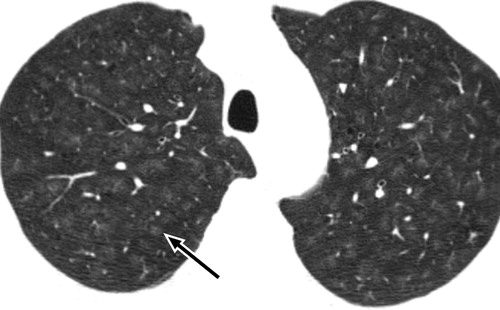
Respiratory Bronchiolitis ILD
Attili, A.K etal Smoking-related Interstitial Lung Disease: Radiologic-Clinical-Pathologic Correlation RadioGraphics Vol. 28, No. 5
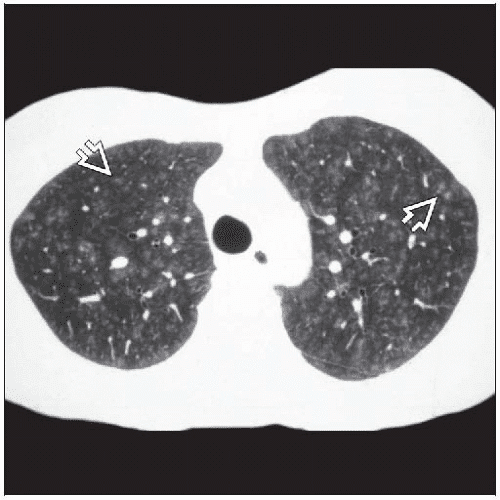
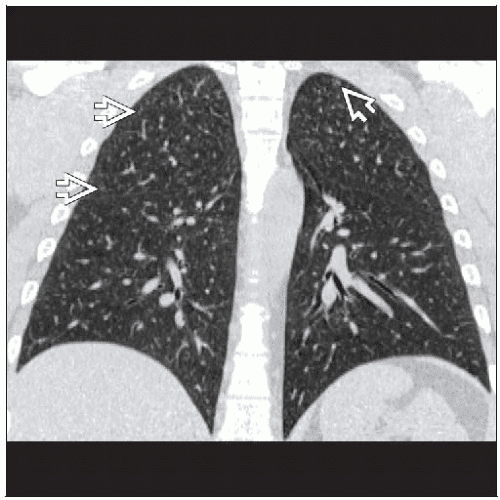
- Respiratory bronchiolitis
Etiology Cigarette Smoke
Difference between RB , RB ILD and desquamative interstitial pneumonia (DIP) is that RB has centrilobular findings while RB ILD has centrilobular changes and ground glass changes and DIP has centrilobular findings ground glass changes and cysts.
Courtesy Wiki
web lungs 437
Prior permission from The Radiological Society of North America.
Sieminska A, et al Respiratory bronchiolitis-interstitial lung disease Orphanet Journal of Rare Diseases volume 9: 106 (2014)
Courtesy Wiki
web lungs 438
Courtesy Radiology Key
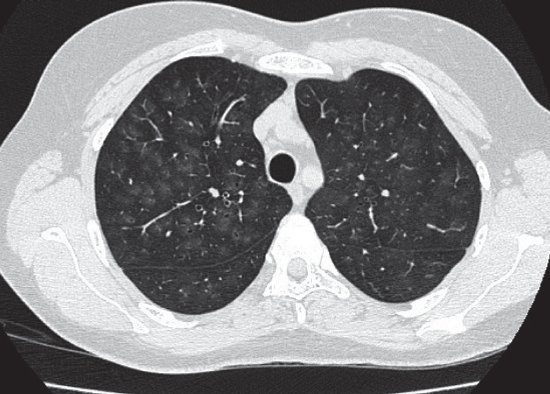
Smoking-Related Interstitial Lung Disease
January 2015Deutsches Ärzteblatt International 112(4):43-50 Hagmeyer L et al
Attili, A.K etal Smoking-related Interstitial Lung Disease: Radiologic-Clinical-Pathologic Correlation RadioGraphics Vol. 28, No. 5 2008
Attili, A.K etal Smoking-related Interstitial Lung Disease: Radiologic-Clinical-Pathologic Correlation RadioGraphics Vol. 28, No. 5 2008
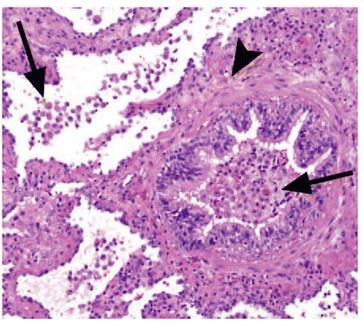
- Histopathology characterized by
-
- pigmented macrophages and
- respiratory bronchioles and alveoli
- mild interstitial inflammatory
- alveolar septa in the peribronchial may be mildly thickened
- no significant fibrosis
-
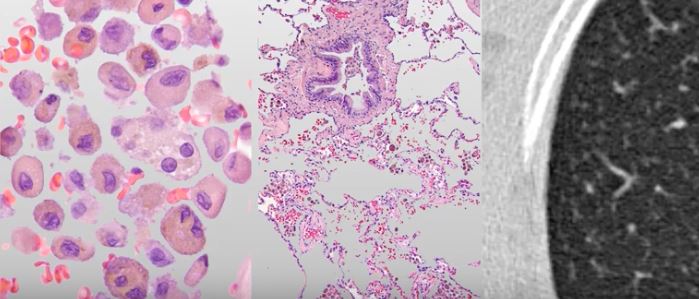
DIP is similar to RB-ILD,
-
- DIP and RB-ILD are a spectrum
- differing in compartments involved
- DIP not bronchiolocentric.
- hyperplasia of the alveolar type II cells
- distribution pattern more homogeneous a
- mild peribronchial fibrosis
Buzz
Use your words
respiratory bronchiolitis = inflammation of the respiratory bronchioles.
dirty lung appearance
centrilobular lung nodules
ground glass
air trapping
emphysema
Respiratory Bronchiole
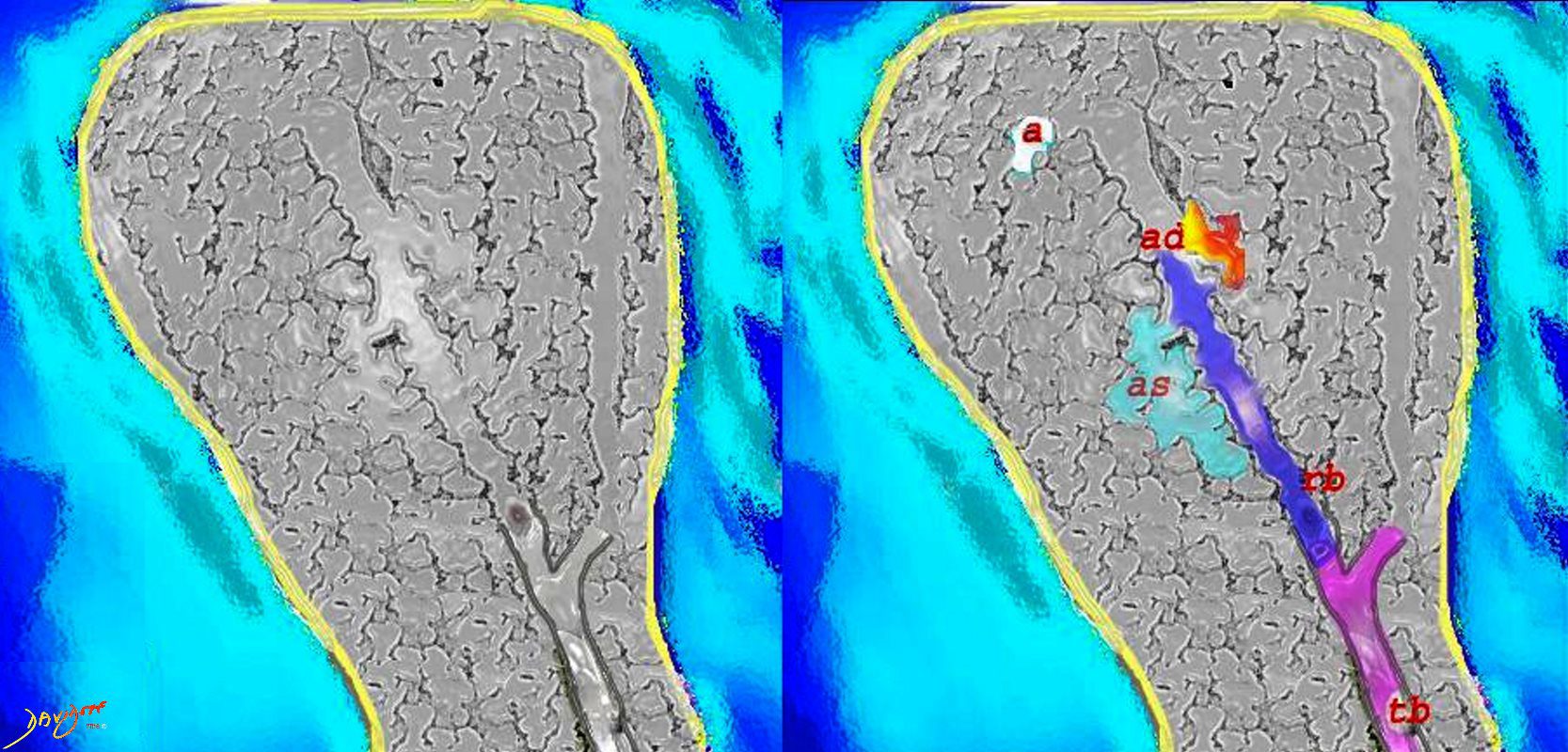
Courtesy Ashley Davidoff MD
lungs-0028-low res
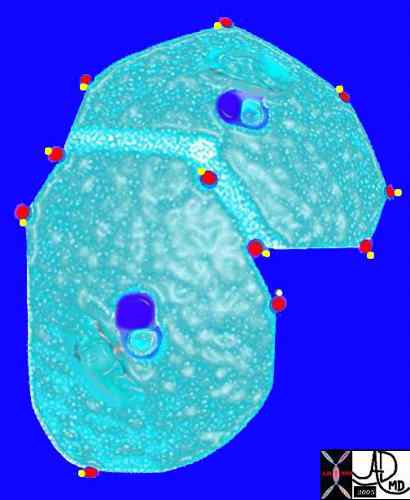
Pulmonary venules (red) and lymphatics (yellow). lie in the periphery of the lobule
42440b03
Davidoff Art Courtesy Ashley Davidoff MD
Secondary Lobule
Inhalation – Upper Lobes
centrilobular ground glass nodules
-
Videos