
- Bronchovascular Nodules- medium sized vessels
- Bronchovascular –
- Secondary lobule
- arteriole
- venule
- bronchiole
- Secondary lobule
- Cavitating
- Lymphovascular Nodules
- Along Bronchovascular Bundle
- Along Fissures
- Secondary Lobule
- interlobular septa
- centrilobular
- Fissural Based Nodules
- Miliary Nodules
- Pleural Based Nodules
- Solid Nodules
- Single
- solid
- calcified
- ground glass
- semisolid
- Cluster
- galaxy
- Single
Bronchovascular – at the bronchial level
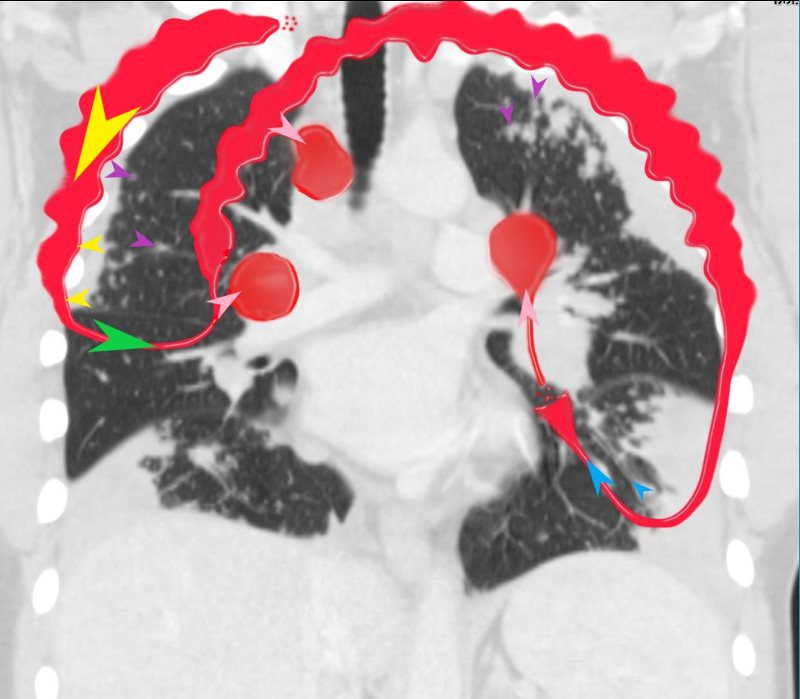
“S” of SARCOIDOSIS
In this diagram the arrows show the direction of flow of the lymphatics. Pleural lymphatics (yellow arrows), Fissural lymphatics, green arrows), flow from the interlobular septa (purple arrows) and along the bronchovascular bundles (blue arrows) all flow toward the lymph nodes in the hila and mediastinum (pink arrows).
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The “S” drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD
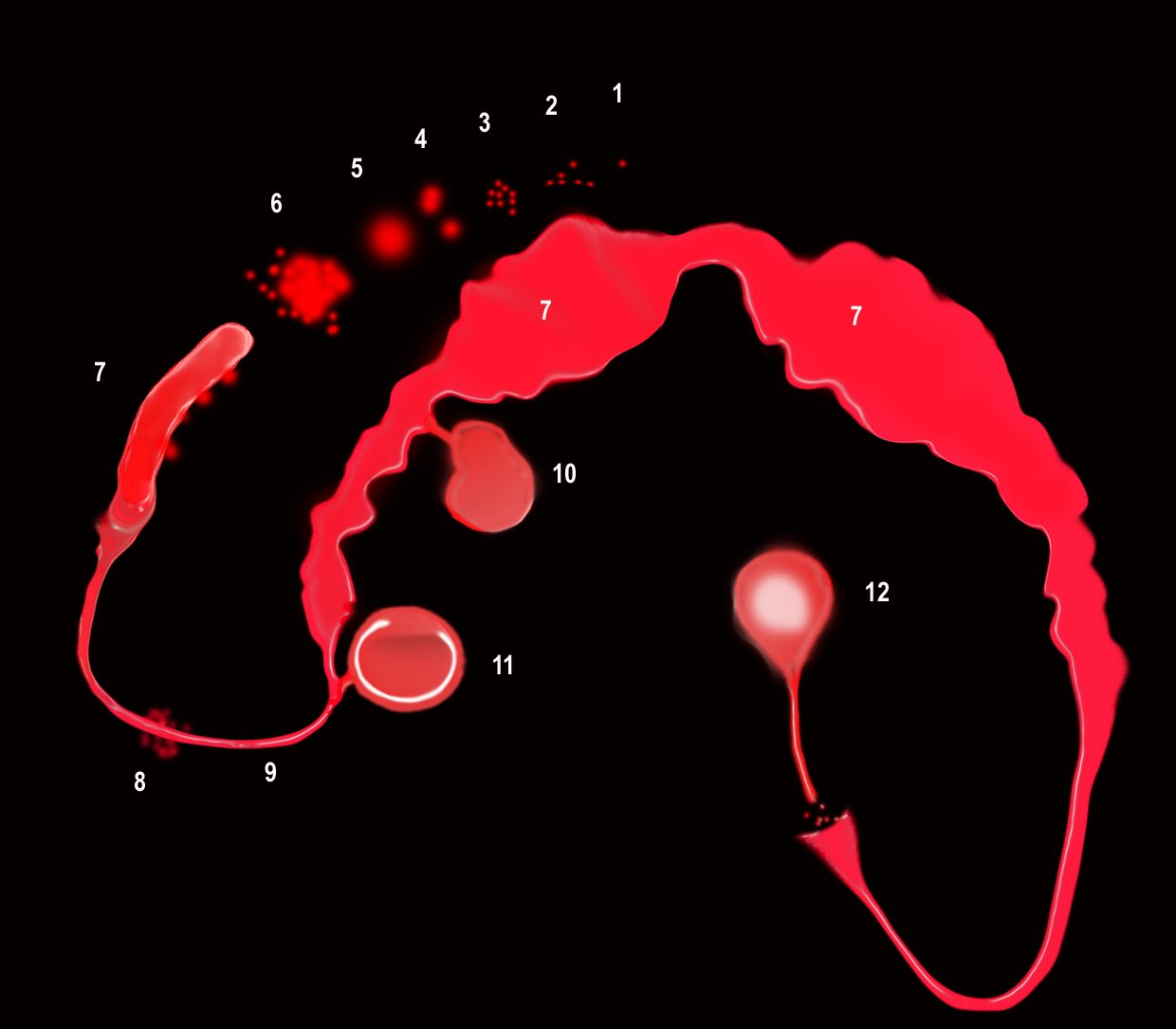
“S” of SARCOIDOSIS
The granulomas start as micronodules in close association with the lymphatics (1) spread in the intralobular septa and centrilobular bronchioles ((2) cluster and conglomerate to form macro nodules (4,5) sometimes manifesting as the galaxy sign (6). As they cluster and conglomerate they can cause conglomerate masses along the pathway (7) most commonly centrally as the lymphatics become confluent in the hila (7)
The lymphovascular bundles may be accompanied by nodularity (8) or just by thickening (9).
The lymph nodes in the mediastinum become significantly enlarged and fleshy (10). They often calcify (12) sometimes on the calcify on the rim of the node (eggshell calcification (11)
Sarcoidosis is a nodular granulomatous disease which predominated in the upper lobes and has its epicenter in the lymphoid tissue of the lungs.
The “S” drawn on the thoracic cage outlines the lymphatic distribution of the lungs, starting in the pleura involving the lymphatic system in the pleura, interlobular septa, bronchovascular bundles and lymph nodes.
The granulomas start out as micronodules and there is a tendency for these to coalesce, sometimes forming large granulomatous masses
When the disease affects the interlobular septa, it causes thickening and nodularity in the septa of the secondary lobule.
When it involves the lymphatics in the pleura or fissures it causes nodularity and thickening.
When it involves the lymphatics around the terminal bronchioles it results in centrilobular micronodules, and when it involves the larger airways it causes thickening and nodularity
Lymph nodes in the hila are characteristically large and flesh like (sarcoid = meat) The Pawnbrokers sign (aka Garland sign or the 1,2,3 sign) describes the enlarged right paratracheal node with bilateral hilar adenopathy.
Parenchymal nodules and micronodules sometimes coalesce to form a central confluent mass with surrounding micronodules, described as the galaxy sign.
Ashley Davidoff MD
Pleural Based
Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD
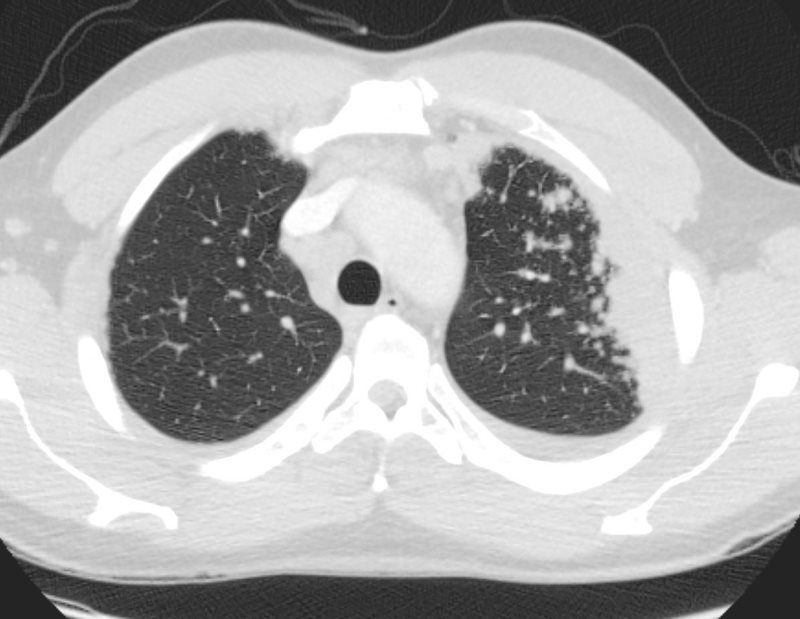
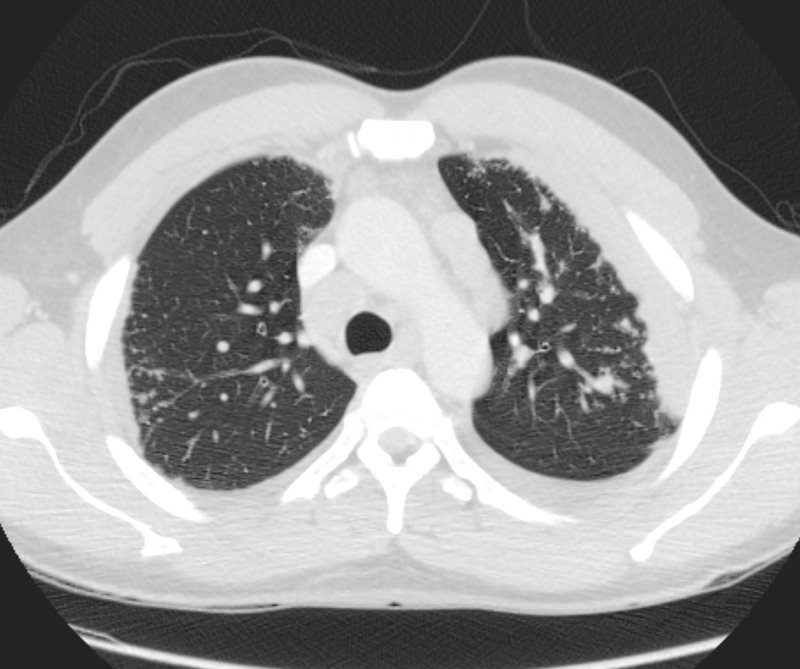
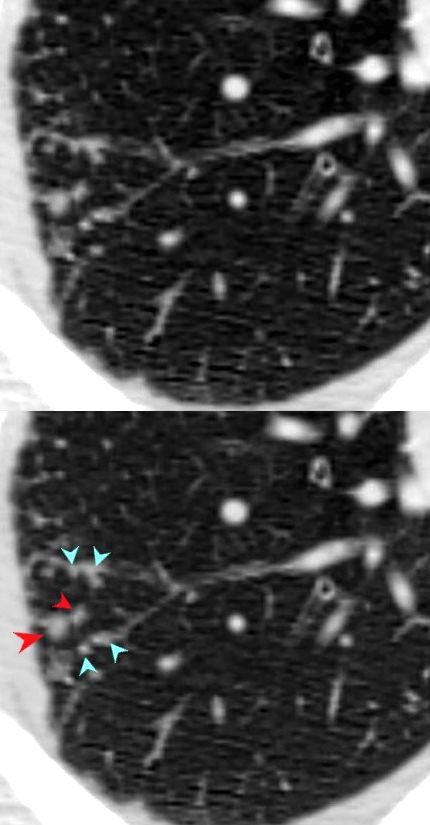
SARCOIDOSIS – CHARACTERISTIC NODULES
Ashley Davidoff MD
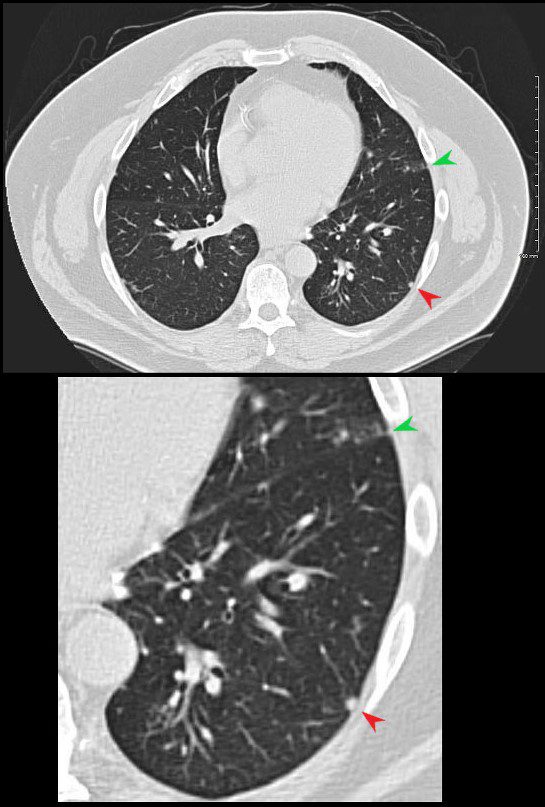
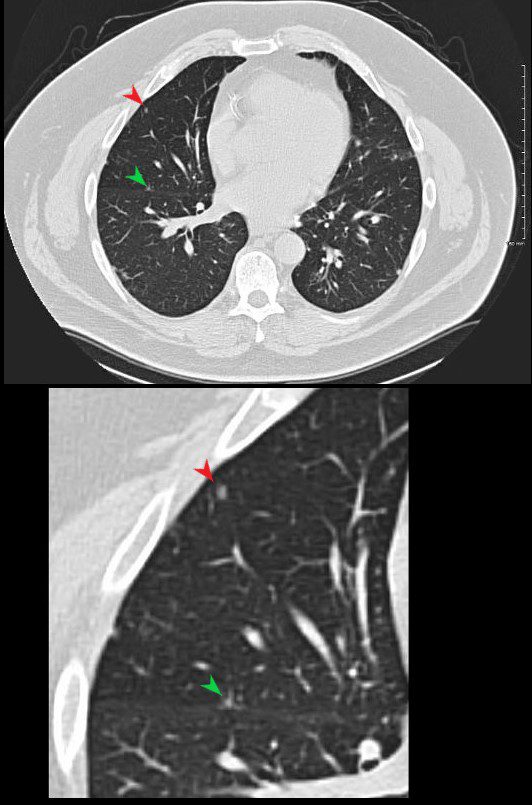
Fissural Based
Ashley Davidoff MD

70-year-old female with micronodules along the fissures
Ashley Davidoff MD
TheCommonVein.net
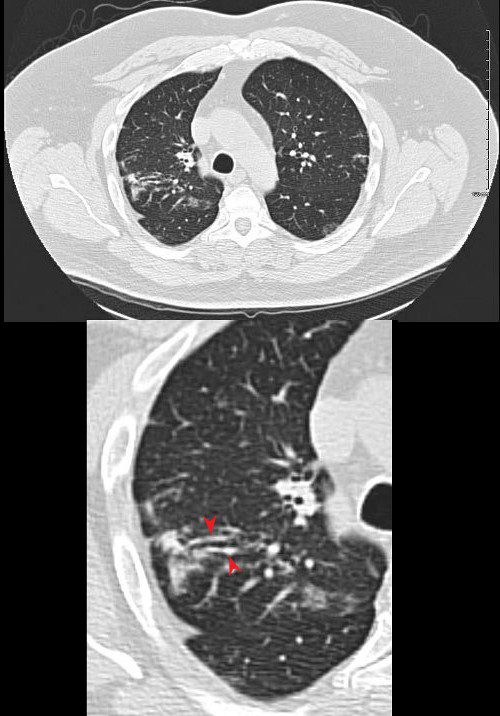
Centrilobular Nodules and Interlobular Septa
Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD
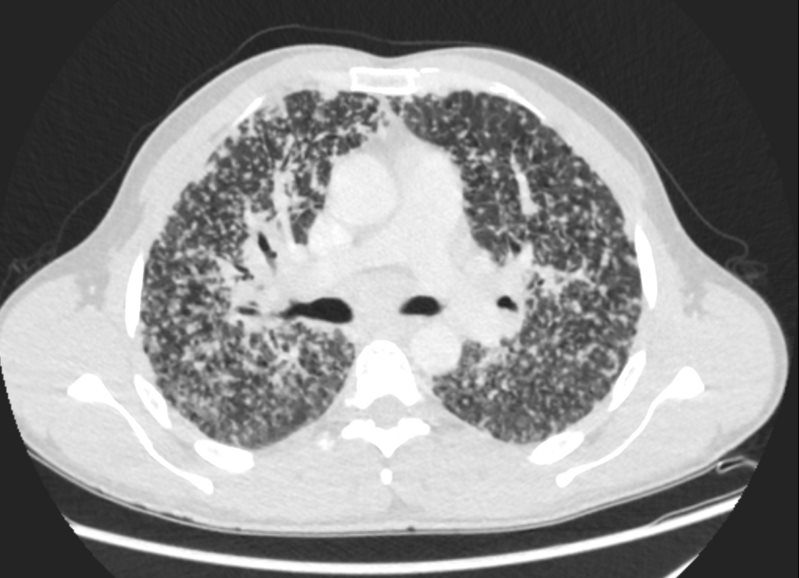
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
Ashley Davidoff MD
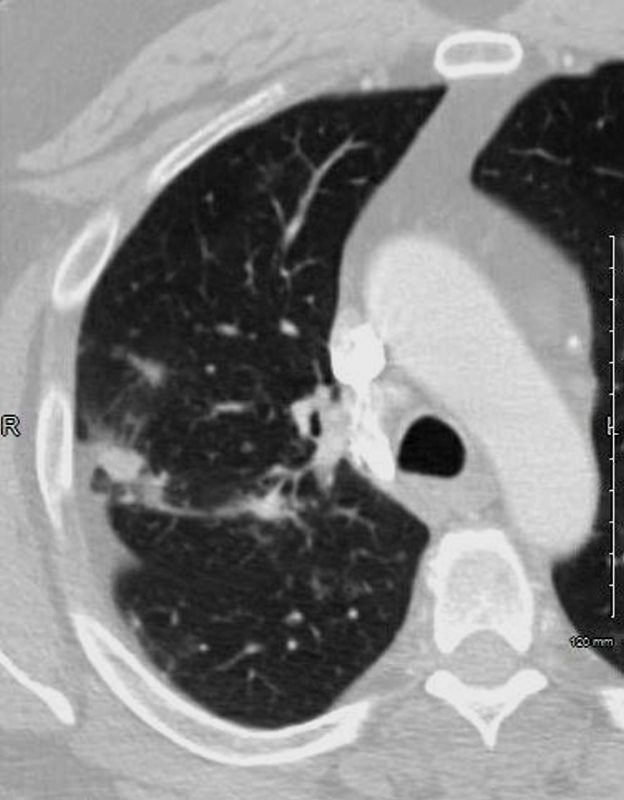
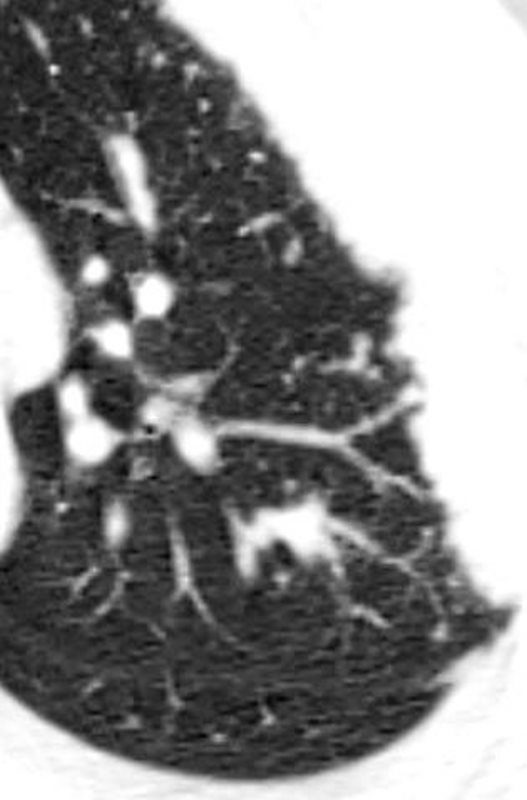
Bronchovascular – at the medium sized bronchial level
Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD
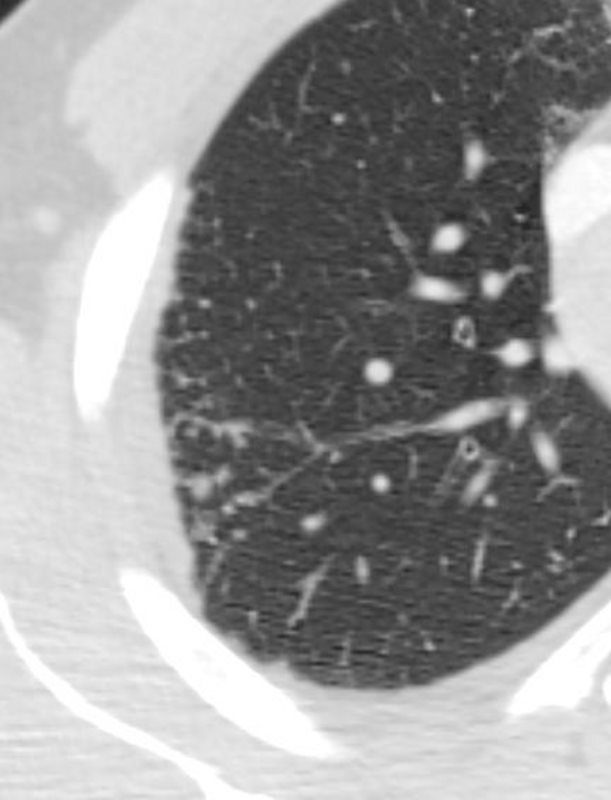
Micronodules
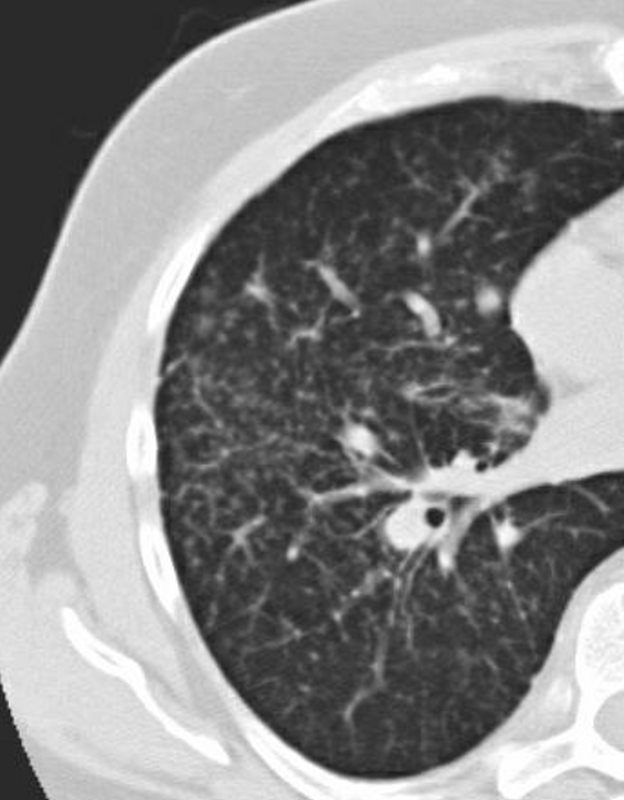
51-year-old male with Stage 2II Sarcoidosis and egg shell calcification of lymph nodes
Ashley Davidoff MD
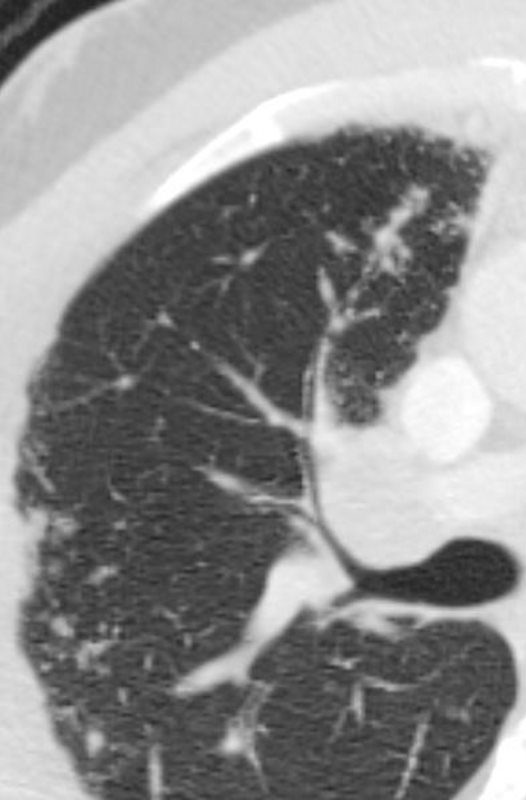
Larger Nodules
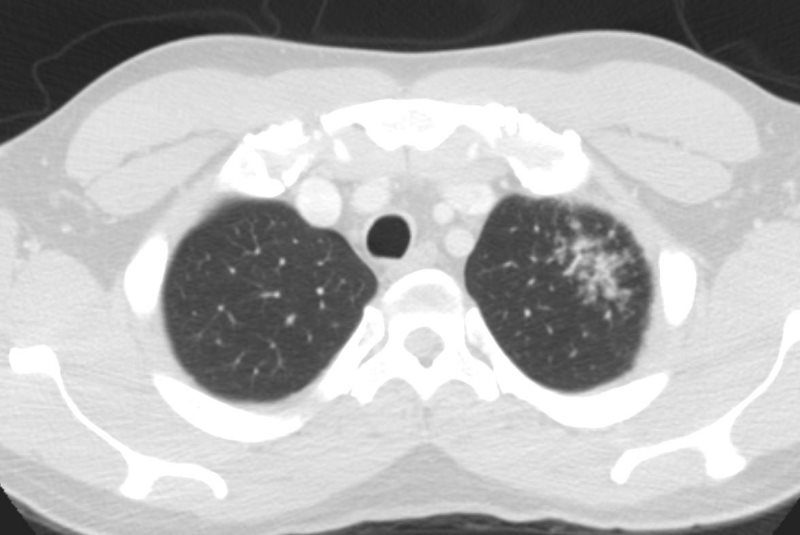
Ground Glass
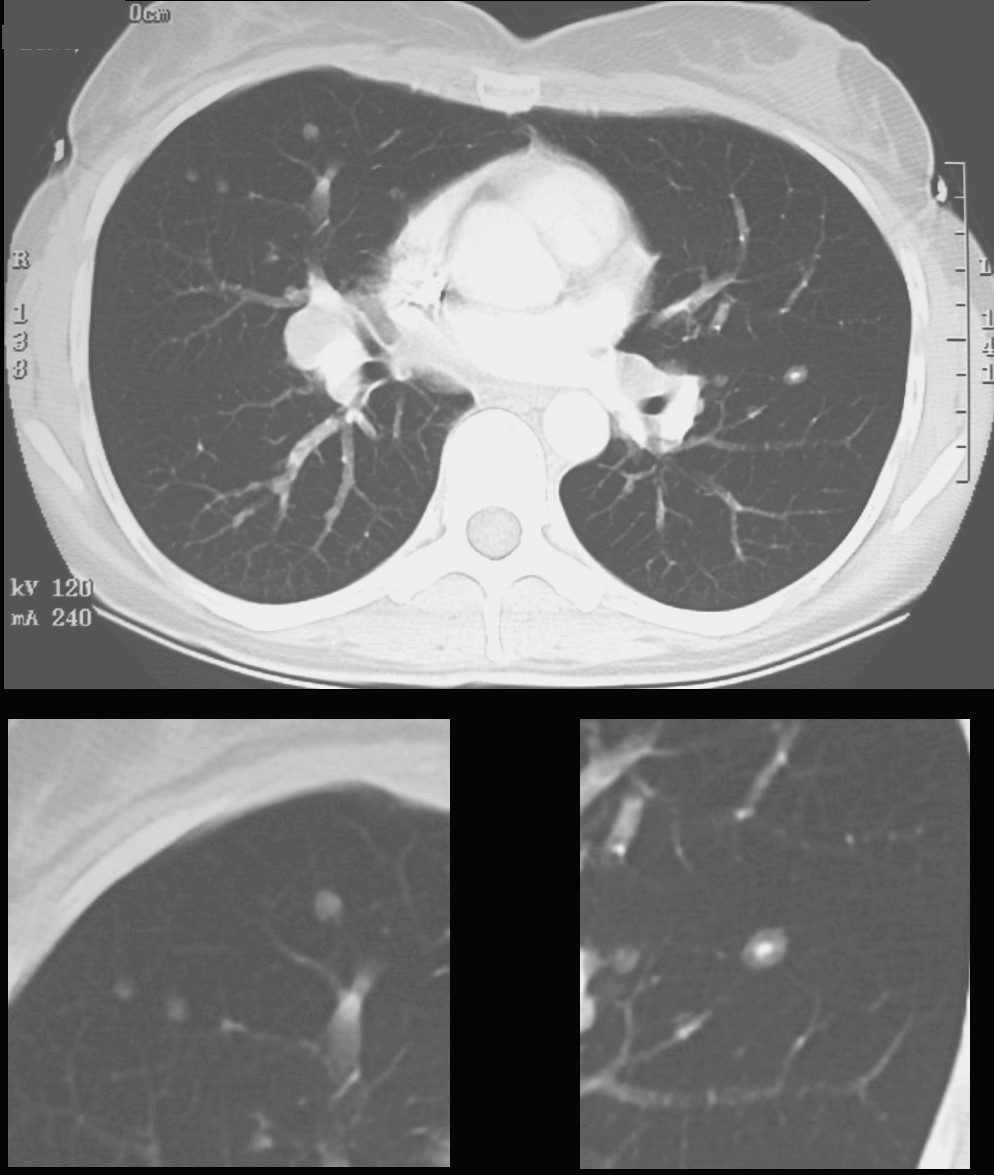
CT scan shows a 6mm nodule with central calcification in the ligula and ground glass nodules in the middle lobe
Ashley Davidoff
TheCommonVein.net
70060c
51-year-old male with Stage II Sarcoidosis and egg shell calcification of lymph nodes
Ashley Davidoff MD
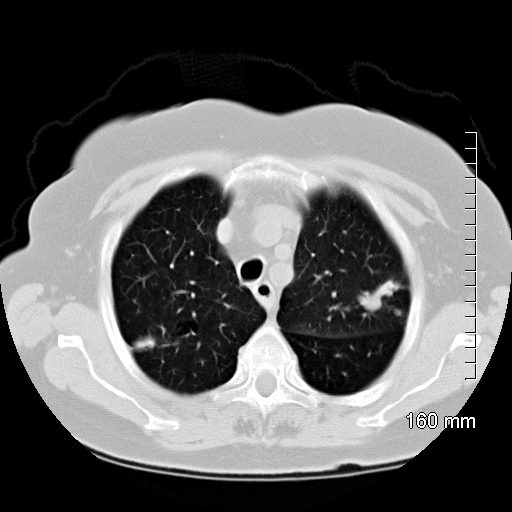
51-year-old male with history of sarcoidosis
The axial images show a variety of characteristic changes including;
Ground glass opacity
Stellate or flame shaped nodules
Semisolid nodules
Ashley Davidoff MD
TheCommonVein.net
-
Solid
-
Single Stellate

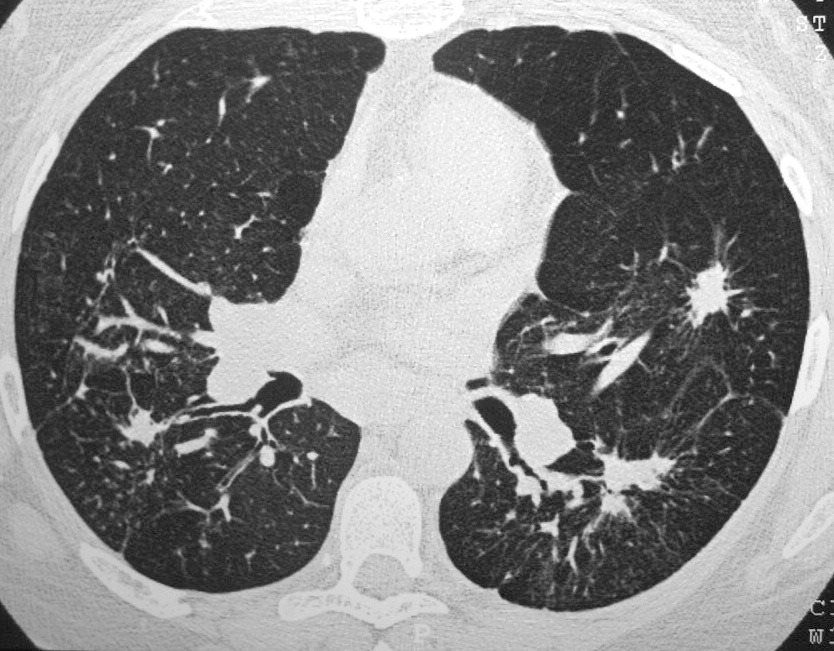
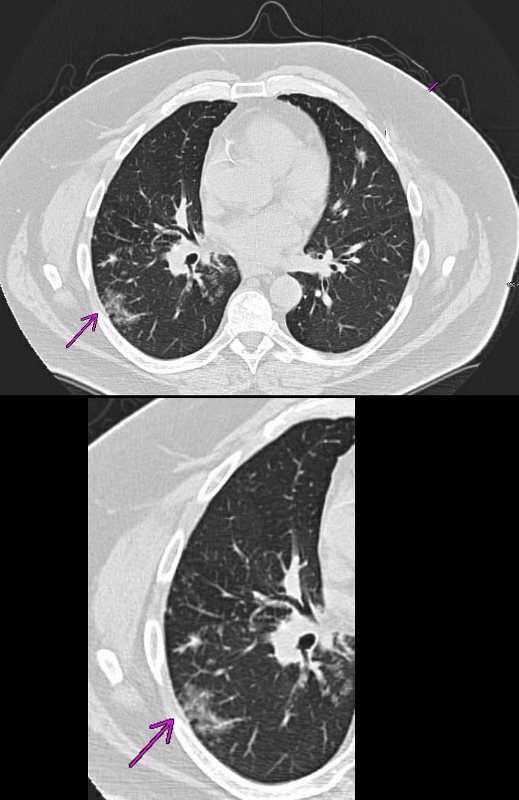
SARCOIDOSIS with STELLATE NODULES
42 year old female with known history of sarcoidosis characterised by confluent granulomas, with spiculated nodules, retractile fibrosis and moderate adenopathy
Ashley Davidoff MD81 F with sarcoidosis
Irregular spiculated solid nodule
Ashley Davidoff
TheCommonVein.net81 F with sarcoidosis
Mixed solid and ground blass nodule
Ashley Davidoff
TheCommonVein.net81 F with sarcoidosis
Irregular solid bilobed nodule
Ashley Davidoff
TheCommonVein.netCT – 3 MAJOR REGIONS OF NODULAR CHANGE ON THE LATERAL cxr
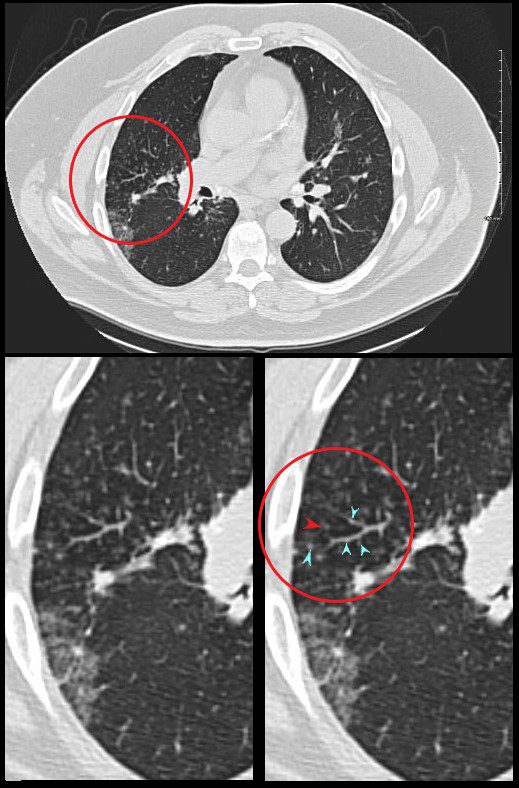
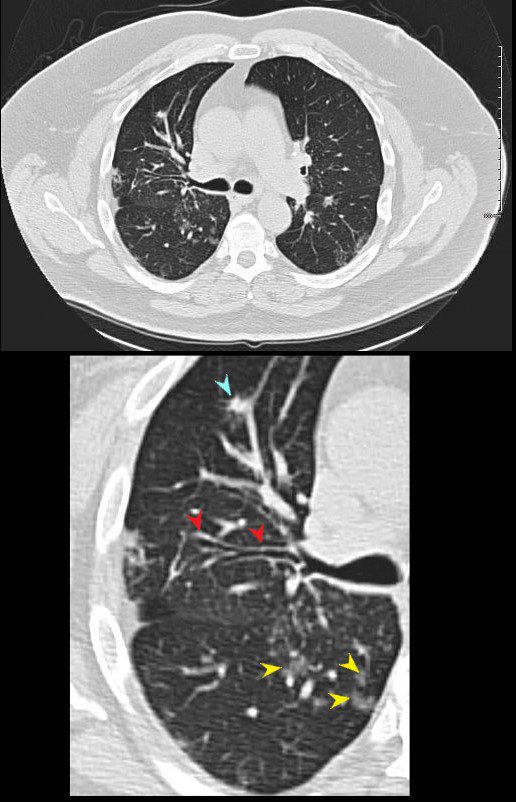
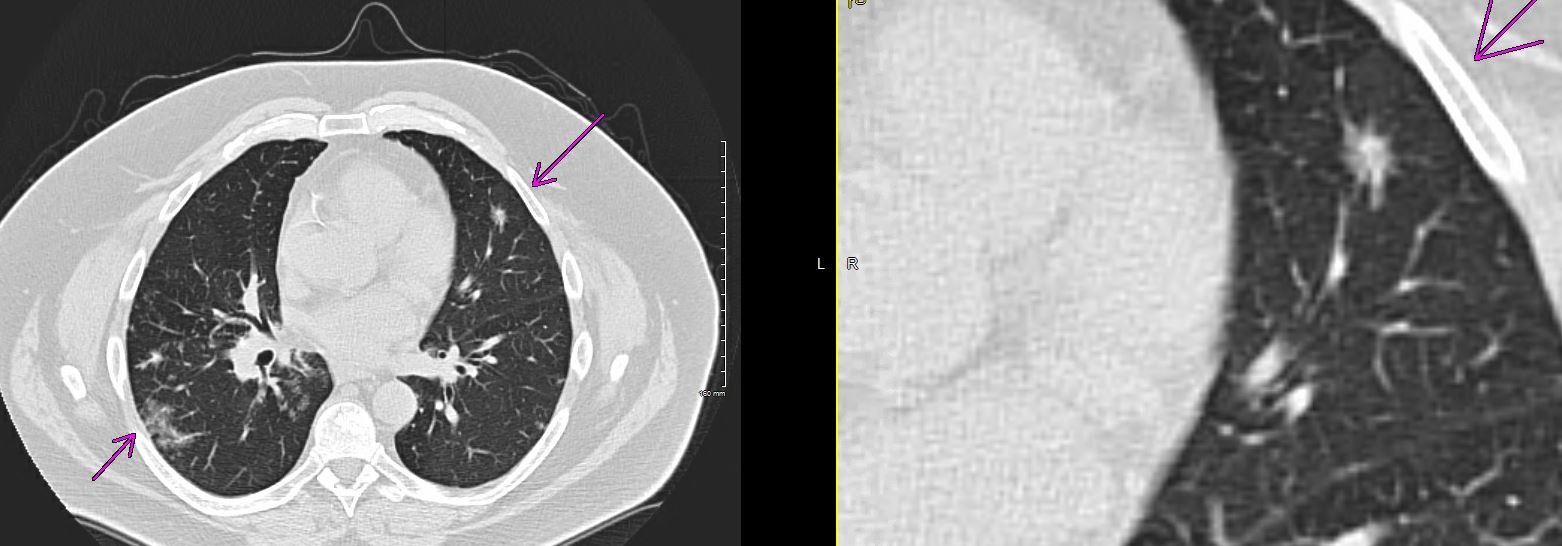
SARCOIDOSIS – CHARACTERISTIC NODULES
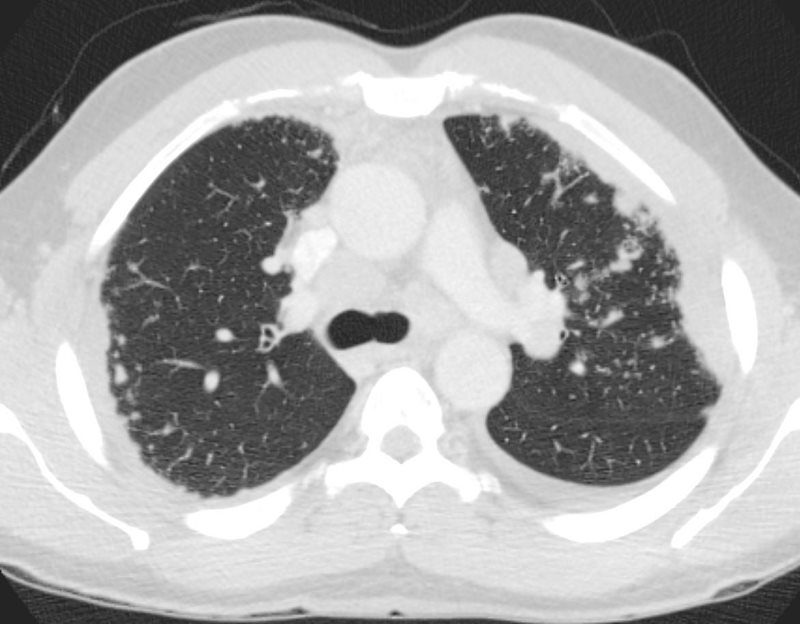
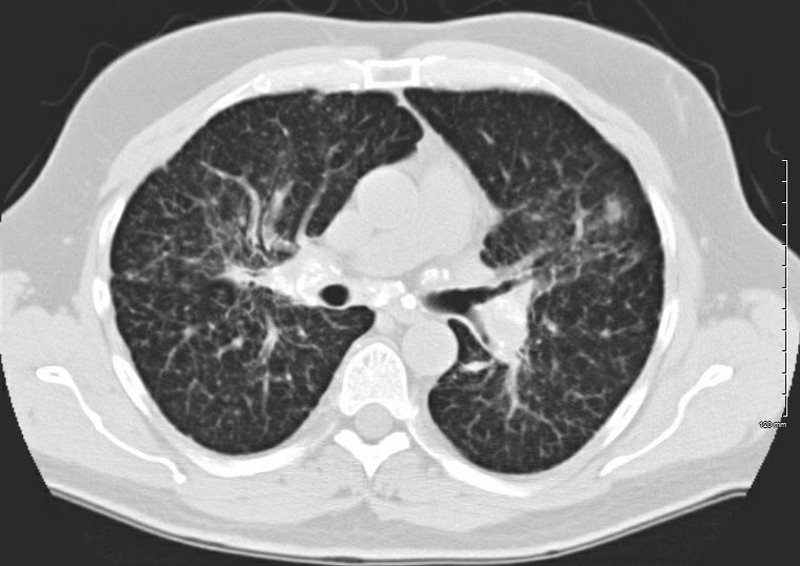
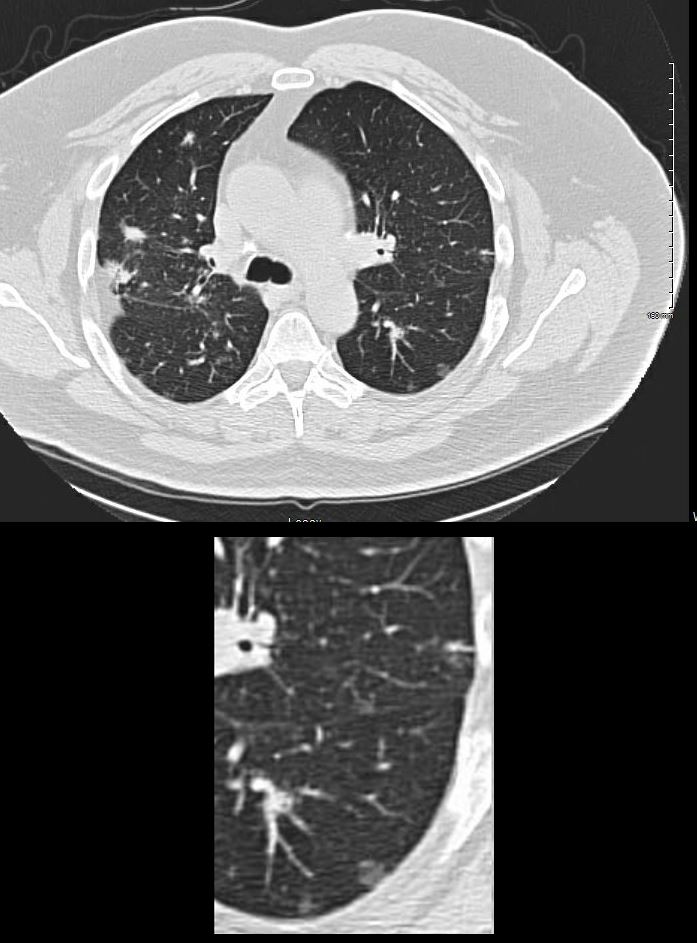
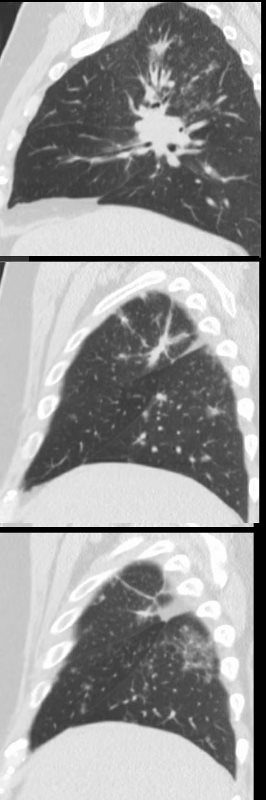
51-year-old male with history of sarcoidosis
The frontal CXR shows subtle nodular changes in the right upper peripheral lung field (red circles) and the lateral examination shows 3 regions of nodular changes (red arrowheads)
The CT examination scout film confirms 3 major regions of nodular change in the posterior and superior segment of the RUL along the confluence of the right major and minor fissure and in the posterior segment of the left upper lobe peripherally.
The axial images show a variety of characteristic changes including;
Ground glass opacity
Stellate or flame shaped nodules
Semisolid nodules
Fissural based nodules
Subpleural nodules
Micronodules along the
lymphovascular and
bronchovascular bundles of the secondary lobule
Calcified nodule some of which are surrounded by soft tissue of the granuloma
There are small calcified nodes in the mediastinum, but no significant pathological adenopathy
No obvious cardiac nor splenic involvement is noted
Ashley Davidoff MDSARCOIDOSIS – CHARACTERISTIC NODULES
51-year-old male with history of sarcoidosis
Ashley Davidoff MD
TheCommonVein.net
-
Conglomerate – Galaxy Sign
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
48-year-old previously well presented with dyspnea and initial CXR showed an infiltrate at the right base, and clinically resolved. He presented a year later with right chest pain and low grade ever and the CXR showed patchy opacities in the LUL and in the RLL
A subsequent CT showed LUL nodular opacities and subpleural rim of consolidation in the LUL and more prominently at both lung bases, associated with significant mediastinal adenopathy. Lymphovacscular nodularity was noted in the bronchovascular bundles as well as in the interlobular septa, consistent with sarcoidosis
CXR and CT 4 years later showed almost complete resolution of the parenchymal findings and the CT findings except for minimal reticulation and scarring in the subpleural regions
Ashley Davidoff MD

SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
48-year-old previously well presented with dyspnea and initial CXR showed an infiltrate at the right base, and clinically resolved. He presented a year later with right chest pain and low grade ever and the CXR showed patchy opacities in the LUL and in the RLL
A subsequent CT showed LUL nodular opacities and subpleural rim of consolidation in the LUL and more prominently at both lung bases, associated with significant mediastinal adenopathy. Lymphovacscular nodularity was noted in the bronchovascular bundles as well as in the interlobular septa, consistent with sarcoidosis
CXR and CT 4 years later showed almost complete resolution of the parenchymal findings and the CT findings except for minimal reticulation and scarring in the subpleural regions
Ashley Davidoff MD

CT WITH SUBPLEURAL NODULES AND MULTIPLE VARIABLY SIZED LEFT APICAL SOLID NODULES
Ashley Davidoff MD The CommonVein.net
SARCOIDOSIS, STAGE IV, PTX, ENCASEMENT
50-year-old male presents with history of Stage 4 sarcoidosis acute chest pain and dyspnea
The initial CXR shows a left sided pneumothorax, diffuse nodular pattern with confluent perihilar infiltrates and a left pleural effusion
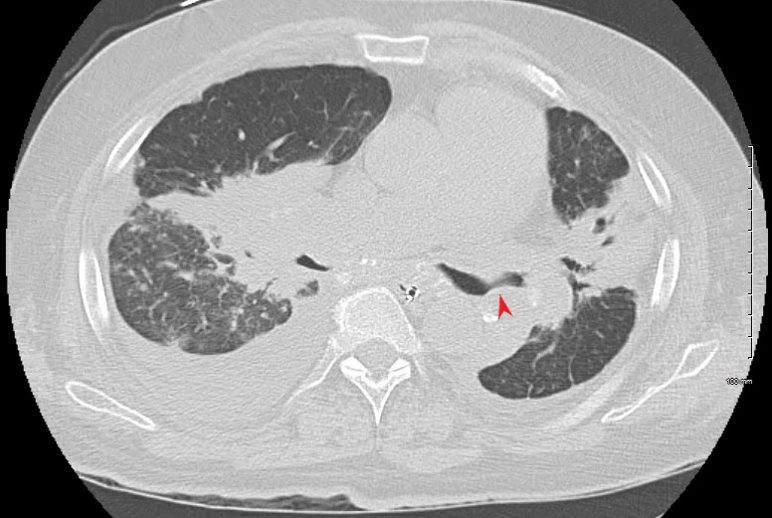
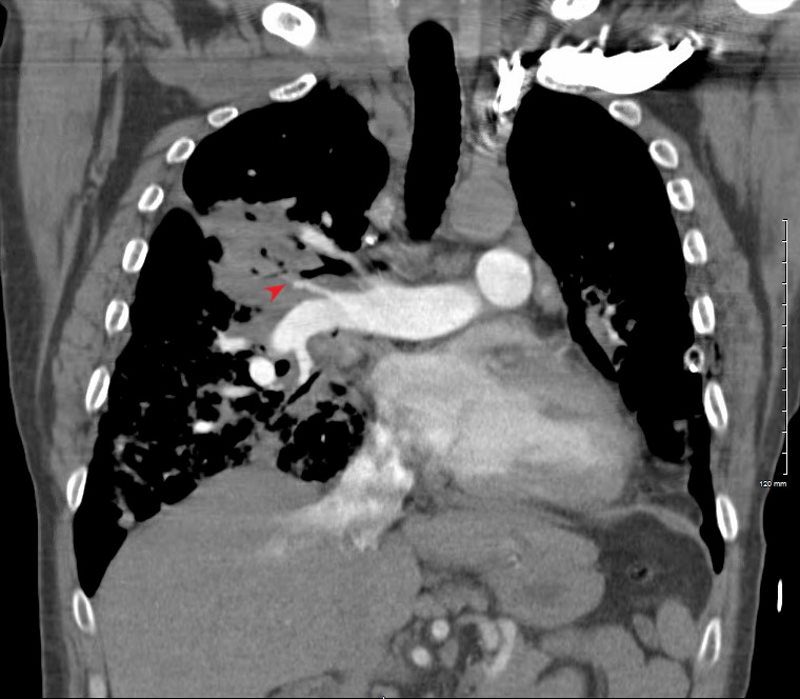
A chest tube was placed and a chest CT showed confluent fibrotic masses in the hilar regions totally surrounding the bronchovascular bundles with encasement of the middle lobe artery. In addition, multiple lymphovascular micronodules are demonstrated. The pulmonary artery measures 32.7mm indicating pulmonary hypertension.
A CXR during this admission shows re-expansion of the pneumothorax. Left lung volume is reduced.
The patient presents 2 years later, again with progressive dyspnea and chest pain and CT PA shows encasement of the airways, right middle lobe pulmonary artery and left lower pulmonary vein by the fibrotic broncho vascular masses, and non-occlusive, subacute pulmonary embolus of the LPA. There are moderate bilateral pleural effusions, calcified lymph nodes, with ongoing pulmonary hypertension with right ventricular enlargement, right atrial enlargement, tricuspid regurgitation and pulmonary hypertension. At this time the patient is intubated.
He again presents 1 month after with chest pain and dyspnea. At this time, he has a tracheostomy. The scout frontal view shows persistent encasement of the left upper lobe bronchus and significant reduction on the volume of the left lung with elevated left hemidiaphragm.
CT PA has similar findings with a large right pleural effusion and unresolved large non occlusive thrombus in the left pulmonary artery.
Ashley Davidoff MD
50-year-old male presents with history of Stage 4 sarcoidosis acute chest pain and dyspnea
The initial CXR shows a left sided pneumothorax, diffuse nodular pattern with confluent perihilar infiltrates and a left pleural effusion
A chest tube was placed and a chest CT showed confluent fibrotic masses in the hilar regions totally surrounding the bronchovascular bundles with encasement of the middle lobe artery. In addition, multiple lymphovascular micronodules are demonstrated. The pulmonary artery measures 32.7mm indicating pulmonary hypertension.
A CXR during this admission shows re-expansion of the pneumothorax. Left lung volume is reduced.
The patient presents 2 years later, again with progressive dyspnea and chest pain and CT PA shows encasement of the airways, right middle lobe pulmonary artery and left lower pulmonary vein by the fibrotic broncho vascular masses, and non-occlusive, subacute pulmonary embolus of the LPA. There are moderate bilateral pleural effusions, calcified lymph nodes, with ongoing pulmonary hypertension with right ventricular enlargement, right atrial enlargement, tricuspid regurgitation and pulmonary hypertension. At this time the patient is intubated.
He again presents 1 month after with chest pain and dyspnea. At this time, he has a tracheostomy. The scout frontal view shows persistent encasement of the left upper lobe bronchus and significant reduction on the volume of the left lung with elevated left hemidiaphragm.
CT PA has similar findings with a large right pleural effusion and unresolved large non occlusive thrombus in the left pulmonary artery.
Ashley Davidoff MD

50-year-old male presents with history of Stage 4 sarcoidosis acute chest pain and dyspnea
The initial CXR shows a left sided pneumothorax, diffuse nodular pattern with confluent perihilar infiltrates and a left pleural effusion
A chest tube was placed and a chest CT showed confluent fibrotic masses in the hilar regions totally surrounding the bronchovascular bundles with encasement of the middle lobe artery. In addition, multiple lymphovascular micronodules are demonstrated. The pulmonary artery measures 32.7mm indicating pulmonary hypertension.
A CXR during this admission shows re-expansion of the pneumothorax. Left lung volume is reduced.
The patient presents 2 years later, again with progressive dyspnea and chest pain and CT PA shows encasement of the airways, right middle lobe pulmonary artery and left lower pulmonary vein by the fibrotic broncho vascular masses, and non-occlusive, subacute pulmonary embolus of the LPA. There are moderate bilateral pleural effusions, calcified lymph nodes, with ongoing pulmonary hypertension with right ventricular enlargement, right atrial enlargement, tricuspid regurgitation and pulmonary hypertension. At this time the patient is intubated.
He again presents 1 month after with chest pain and dyspnea. At this time, he has a tracheostomy. The scout frontal view shows persistent encasement of the left upper lobe bronchus and significant reduction on the volume of the left lung with elevated left hemidiaphragm.
CT PA has similar findings with a large right pleural effusion and unresolved large non occlusive thrombus in the left pulmonary artery.
Ashley Davidoff MD

-
-
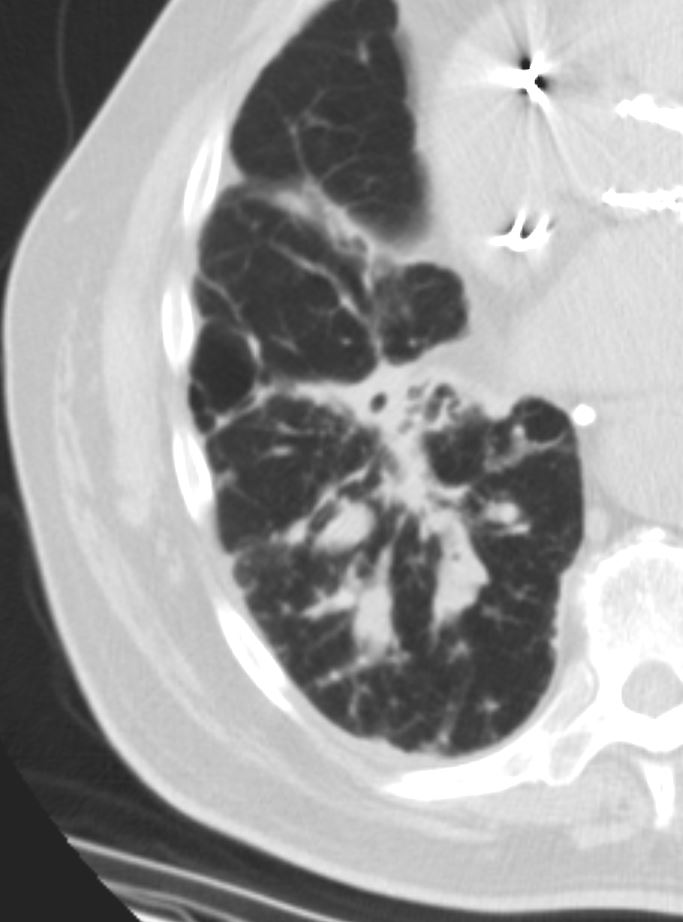
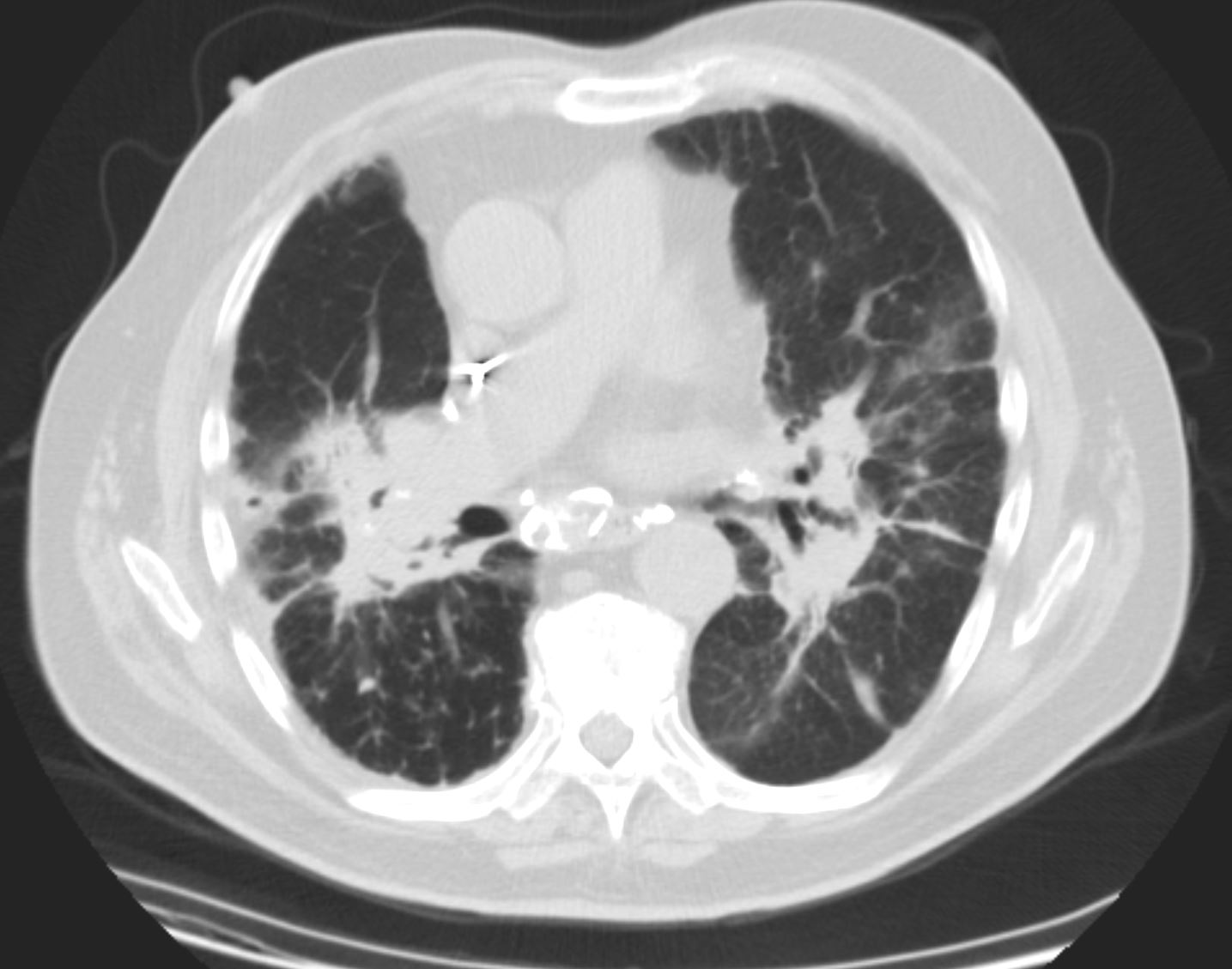
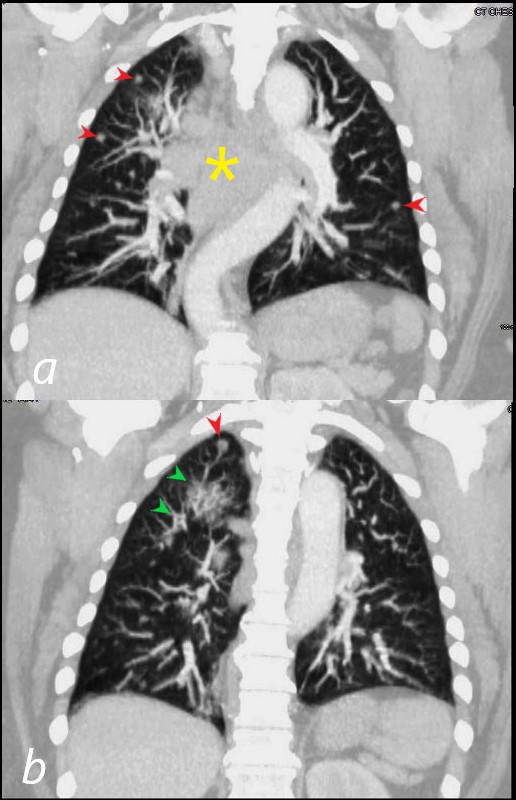
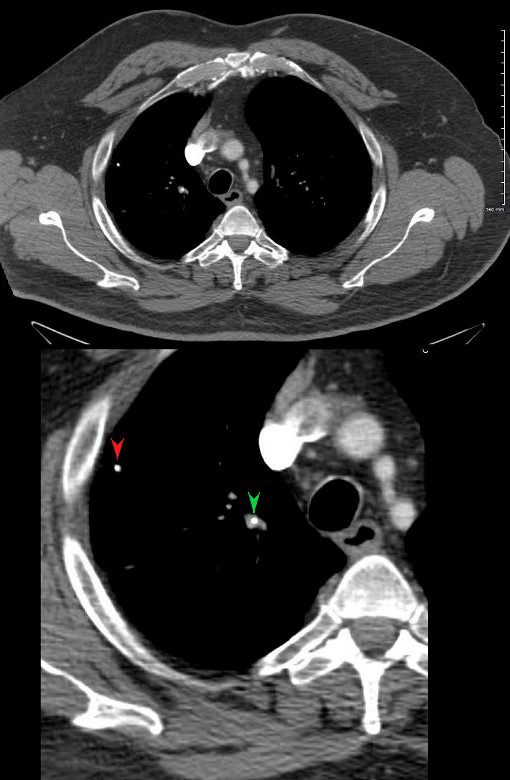
UPPER LOBE LUNG NODULES (red arrows) AND BRONCHIOLECTASIS (green arrow)-MEDIASTINAL ADENOPATHY (yellow asterisk) (Ref TCV Sarcoidosis and Takotsubo Heart)
Ashley Davidoff MD -
Cluster of Solid Nodules
-
CT WITH SUBPLEURAL NODULES AND MULTIPLE VARIABLY SIZED LEFT APICAL SOLID NODULES
Ashley Davidoff MD -
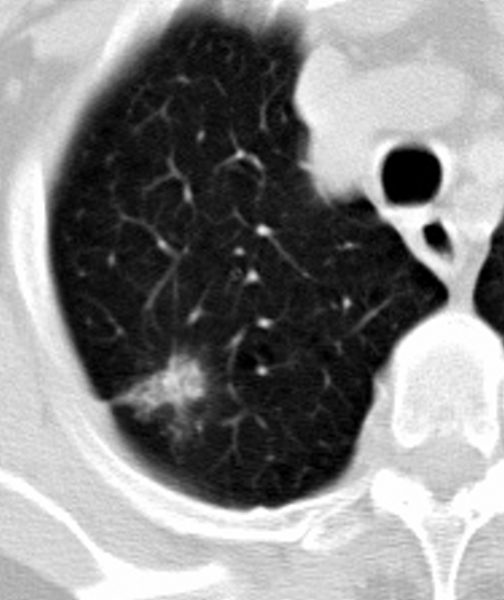
Stellate or Flame Shaped
-
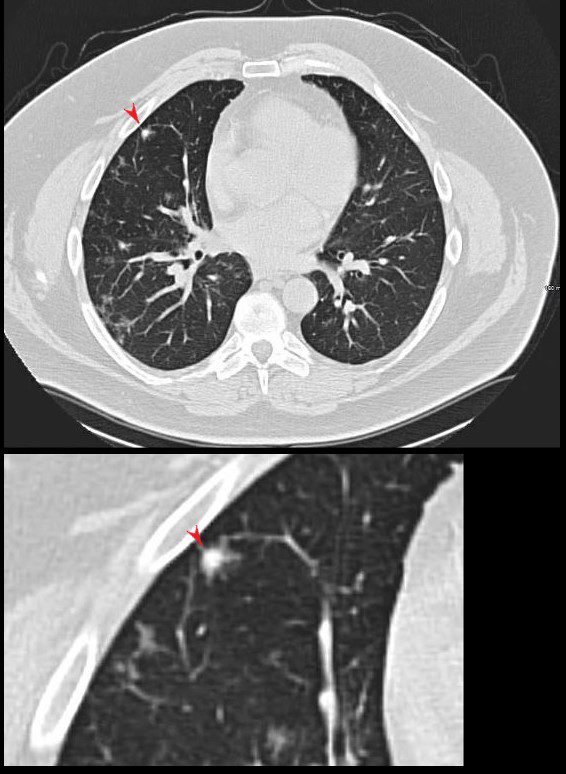
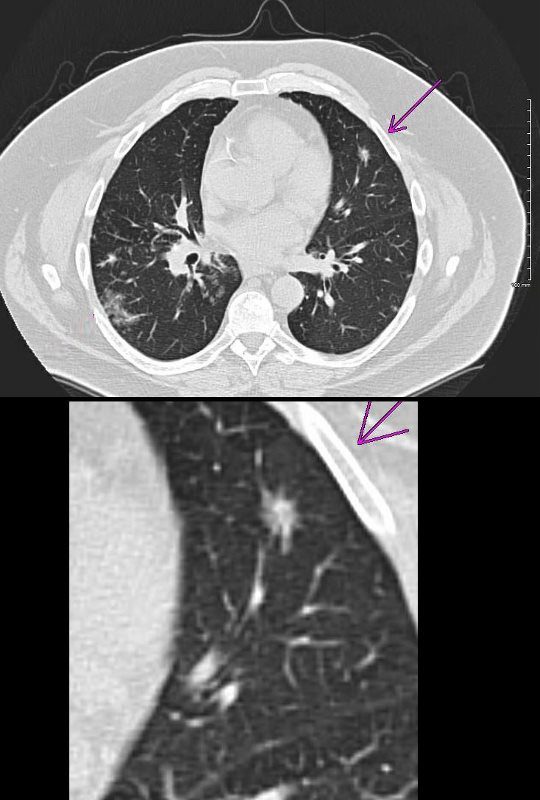
STELLATE OR FLAME SHAPED NODULE
Ashley Davidoff MDSTELLATE OR FLAME SHAPED NODULE
Ashley Davidoff MD
-
Calcified
Ashley Davidoff MD
Semi Solid
Ashley Davidoff MD
Ground Glass
Ashley Davidoff MD
Galaxy

Ashley Davidoff MD
Ashley Davidoff MD
CT WITH SUBPLEURAL NODULES AND MULTIPLE VARIABLY SIZED LEFT APICAL SOLID NODULES
Ashley Davidoff MD
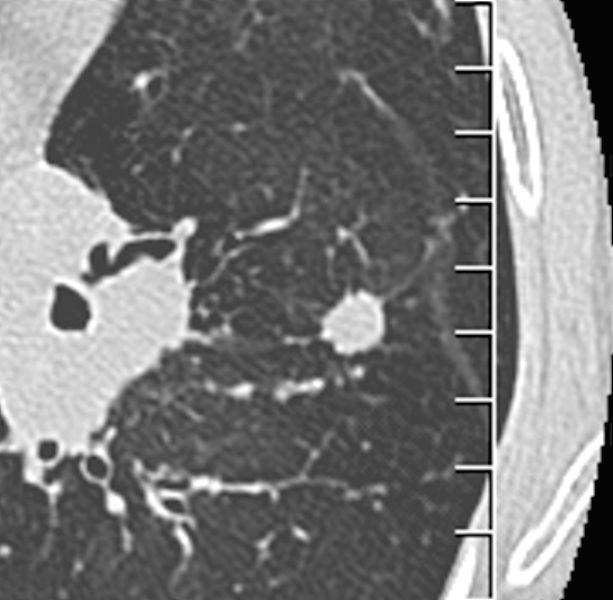
Calcified
CT scan shows a 6mm nodule with central calcification in the ligula and ground glass nodules in the middle lobe
Ashley Davidoff
TheCommonVein.net
70060c
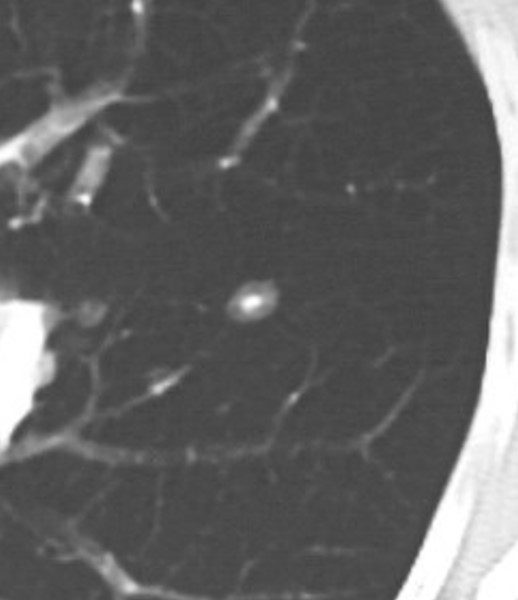
CT scan shows a 6mm nodule with central calcification
Ashley Davidoff
TheCommonVein.net
70060b
Miliary
Ashley Davidoff MD
-
Links and References
- TCV
- TCV