
In a Nutshell
- Clinical Presentation
- Distant history of silica exposure (sandblasting, glass manufacturing, mining), generally appears 10-30 years after exposure
- Chronic, insidious cough and dyspnea on exertion
- Crackles, wheezing, and rhonchi may be present on lung exam
- Imaging Features
- Size
- Nodular opacities 1-10mm diameter,
- well defined and uniform, may be calcified
- Shape
- subpleural nodules coalesce,
- “candle wax” lesions or
- “pseudoplaques”
- subpleural nodules coalesce,
- Position
- Size
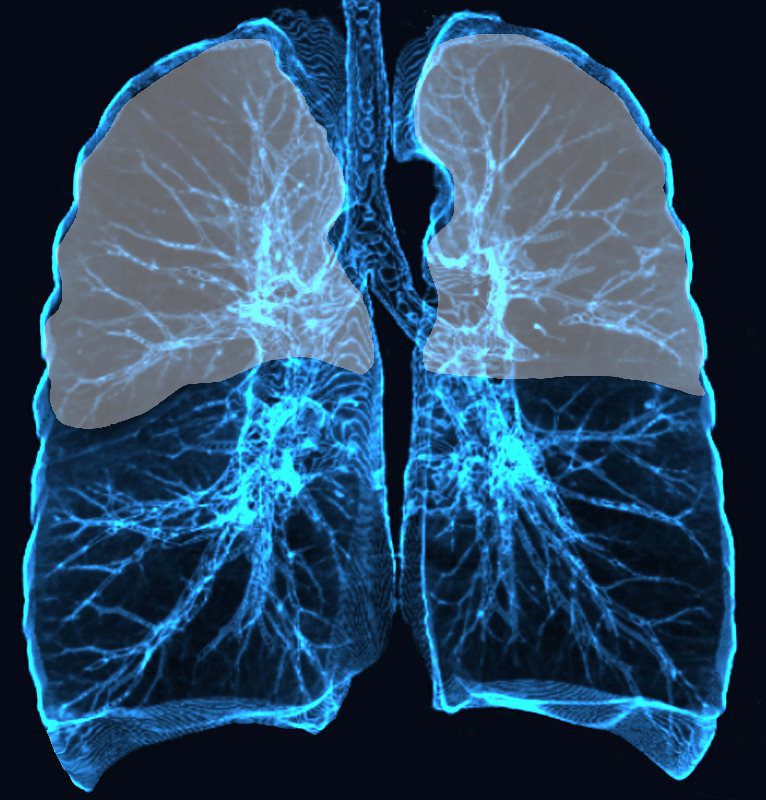
Upper and mid lung field distribution
Ashley Davidoff MD TheCommonvein.net lungs-0772
-
-
- Upper lobes and posterior lung field opacities
- perilymphatic distribution
- subpleural nodules
- Associated Foindings
- Hilar and mediastinal lymphadenopathy
- Calcified lymph nodes: “eggshell calcifications”
-
- Potential Complications
- Progressive massive fibrosis
- Increased risk of mycobacterial infections
- Chronic necrotizing aspergillosis
- Rheumatic disease: systemic sclerosis, rheumatoid arthritis
- Remember
- Acute silicosis (silicoproteinosis) is a slightly different pathology characterized by rapid development of cough, dyspnea, fatigue, and weight loss that can present a few weeks to years after high concentrations of silica exposure.
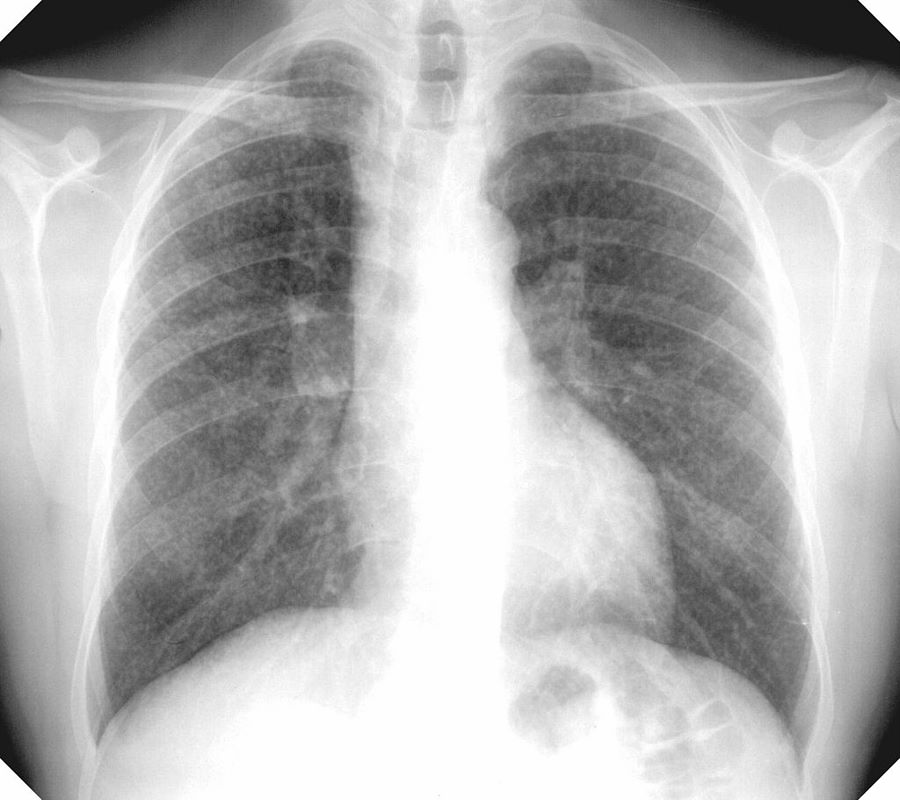
Reticulo-Nodular Pattern on CXR

CXR (PA view) shows interstitial reticulonodular and coalescing opacities in the lungs bilaterally consistent with a diagnosis of classic complicated silicosis. Differential diagnosis includes coal worker’s pneumoconiosis and talcosis.
Case courtesy of Dr Ian Bickle, Radiopaedia.org, rID: 33227
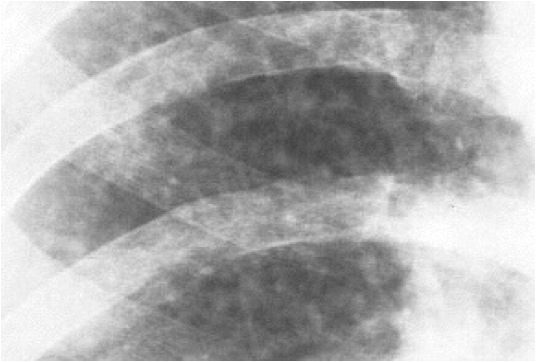
Chest X-ray showing uncomplicated silicosis
Courtesy Gumersindorego
Courtesy DrSHaber
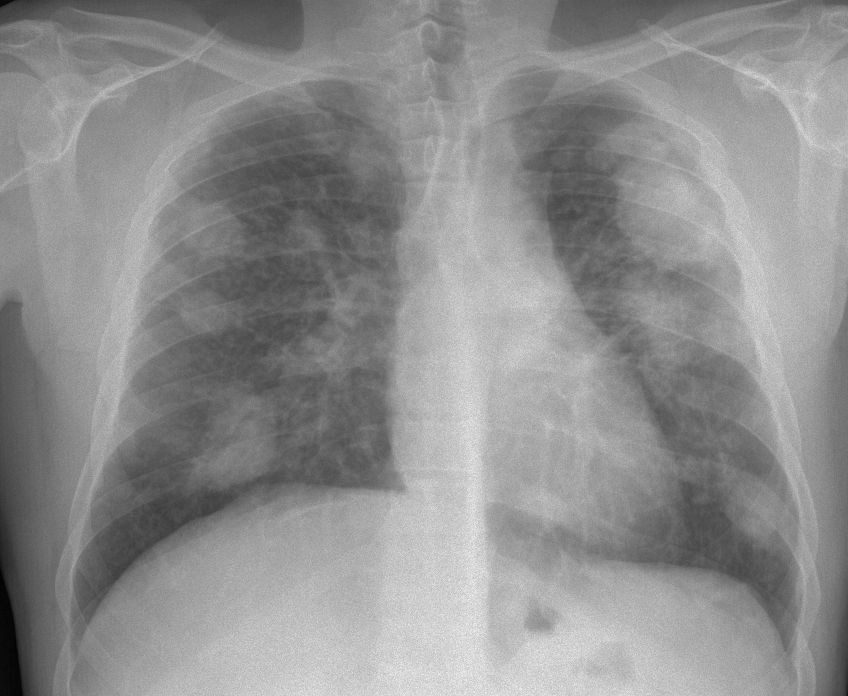
Chest X-ray showing complicated silicosis
Courtesy Gumersindoreg
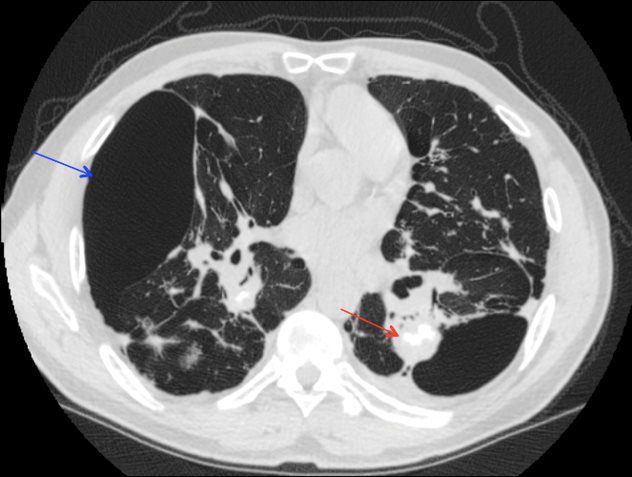
Massive Pulmonary Fibrosis
65 year-old male with known history of COPD on nocturnal O2, pulmonary HTN, and past occupation in marble quarry presents to ED with 5 days of cough and dyspnea.
In ED, patient HR 131 and RR 28 with O2 sat in 80s on RA. VBG shows pH 7.38 and pCO2 55 mmHg
Clinical Follow Up
Following BiPAP placement in the MICU, patient’s respiratory status showed marked improvement. Final diagnosis was acute COPD exacerbation in the setting of underlying silicosis with progressive massive fibrosis.
Patient was treated with albuterol, ipratropium, and prednisone for COPD exacerbation. Patient was progressively weaned to RA while maintaining O2 sat >95% through day of discharge.

Courtesy Maegan Lu, Jonathan Scalera, MD

Courtesy Maegan Lu, Jonathan Scalera, MD
Courtesy Maegan Lu, Jonathan Scalera, MD
Case from the Literature of Massive Pulmonary Fibrosis

Coronal CT at the level of bronchi shows soft-tissue masses with irregular borders and significant bullous disease in bilateral lungs consistent with a diagnosis of classic complicated silicosis. Differential diagnosis includes coal worker’s pneumoconiosis and talcosis.
Case courtesy of Dr Michael P Hartung, Radiopaedia.org, rID: 71691
References and Links