
Introduction
Size of the Lung
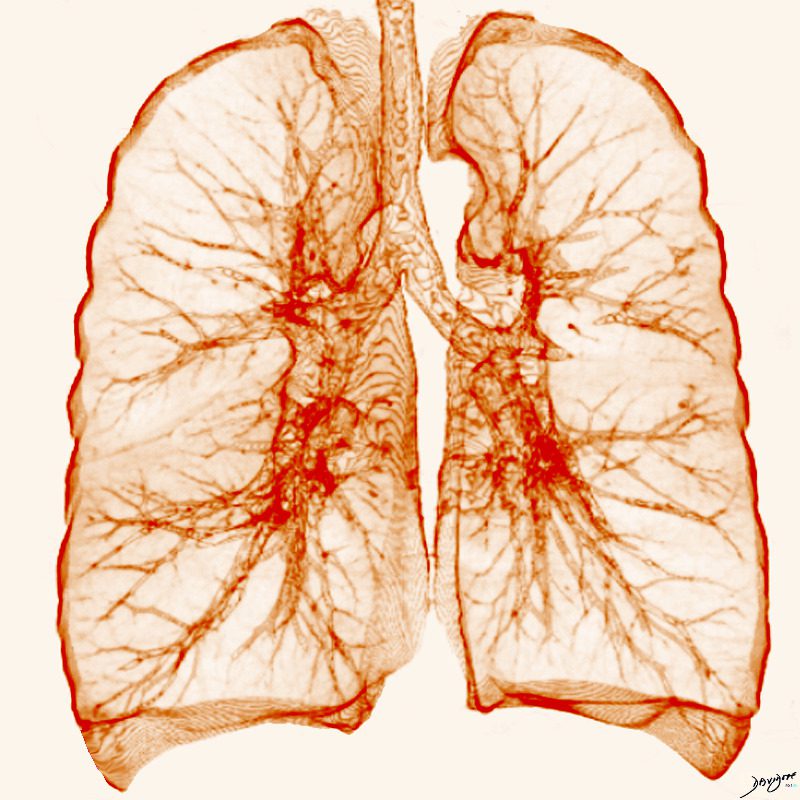
Ashley Davidoff MD TheCommonVein.net lungs-0702
Summary
- Alveoli
- 300 million alveoli 20,000 acini
- Alveoli
- major component of the lung
- make up approximately
- 50% of lung volume.
- Found outer 1/3
- situated dominantly in the periphery
- tubular transport systems are located centrally by the hilum .
- During inspiration the
- radius of the alveolus
- doubles
- from about 0.05 mm
- to 0.1 mm
- make up approximately
- major component of the lung
- Height = 24cms
- Weight = 900-1200 grams (40-50% is blood)
- Right = 630gms
- Left = 570 grams
- Volume
- Total –
- 6300ml in adult men and
- 4200ml in adult women.
- End-expiration,
- 2500mls,
- Maximal inspiration
- 6000mls
- End-expiration,
- Taking a rate of
- 10-15 breaths per minute
- (about 17,000 breaths per 24 hours)
- results in approximately
- 10,000 liters of air inspired per day.
- 20,000 liters expiration and Inspiration
- Total –
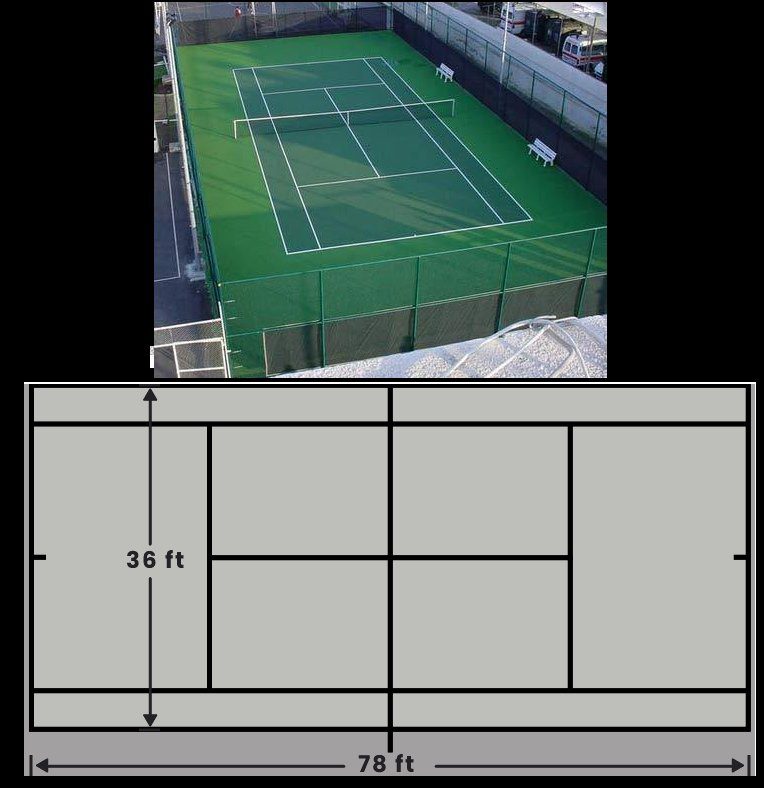
- Surface area
- 80 square meters, about the size of a tennis court.
The lungs are one of the more voluminous organs in the body but in terms of weight are relatively light for their size, since they mostly are filled with air. Additionally, their size can change dramatically since the difference in volume between a deep inspiration and deep expiration can be as much as 3.5 liters.
Surface anatomy
Within the thorax the lungs extend superiorly passed clavicle into the base of the neck, with a craniocaudal length in inspiration of approximately 24 cms. Posteriorly, on a chest X-Ray they reach to the 10 rib. Cranially they extend to the first thoracic vertebrae and inferiorly to the dome of the diaphragm and costophrenic sulci more inferiorly.
In patients with COPD or an acute asthmatic attack the lung volumes are expanded and the lungs will be seen beyond the 6th rib anteriorly and the 10th rib posteriorly.
Weight
In the living and breathing adult, the lungs weigh approximately 900 to 1200 grams, of which nearly 40% to 50% is blood. The weight will depend on how much blood is running through the lungs. At rest it is 5L/min, but during exercise with up to 25L/min flowing through the lungs, at any one time during exercise the lungs will be that much heavier.
At rest the lungs together weigh about the same as the liver, which is 1/3 the volume of the lungs.
In the adult, the right lung weighs about 630 grams and the left weighs 570 grams. The left lung is smaller, since the heart, which is dominantly a left sided structure, occupies part of the left chest.
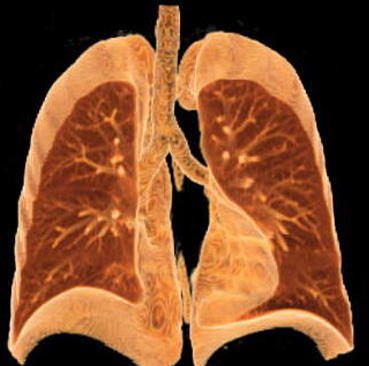
A coronally reconstructed CT image showing the effect of the normal left sided position of the heart on the volume of left lung. Note how much smaller the left lung is compared with the right.
Ashley Davidoff MD. TheCommonVein.net 32623
Diameters of the Bronchi
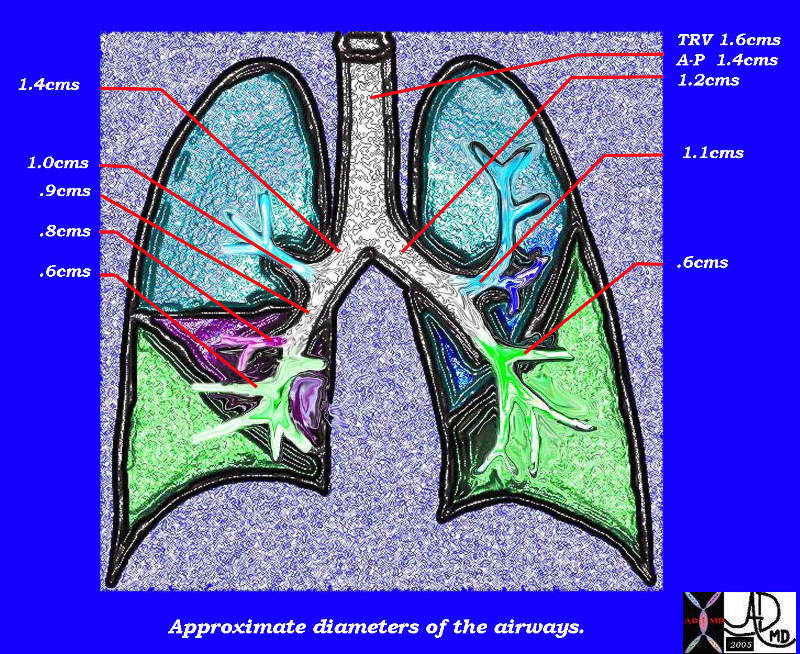
This diagram of the airways reveals the approximate diameters of the airways. Note that the left main stem bronchus is thinner than right whose length is truncated by the take off of the right upper lobe bronchus.
Ashley Davidoff MDTheCommonVein.net
32686b05L05b
Volumes
The total volume of the lungs is about 6300ml in adult men and 4200ml in adult women. At end-expiration, the volume of air within the lungs is about 2.5 L, whereas at maximal inspiration it may be 6 L. Taking a rate of 10-15 breaths per minute (about 17,000 breaths per 24 hours) results in approximately 10,000 liters of air inspired per day. Of course an equal amount has to be expired per day as well, and so there is the back and forth movement of about 20,000 liters per day.
Alveoli make up approximately 50% of entire lung volume. The outer 1/3 of the lung contains 50% of the alveoli. Thus alveoli are the major component of the lung and they are situated dominantly in the periphery while the tubular transport systems are located centrally by the hilum .
The lung and the kidney have structural similarities in that the outer third of the kidney called the cortex, contains most of the key functioning and filtering aspects of the kidney whereas the inner and more central medulla houses the tubular system. The similarity is such that some refer to the lung as having an outer cortex and an inner medulla.
Surface area
There are about 20,000 acini and 300 million alveoli in the normal lung. During inspiration the radius of the alveolus doubles from about 0.05 mm to 0.1 mm. The total surface area of the lung is about 80 square meters, about the size of a tennis court. The extent and volume of air that is moved across the alveoli is simply stunning.
As we have already seen about 5-10 liters of air is moved through the tracheobronchial tree per minute at rest. During exercise up to 100 liters of air can be moved through the airways per minute and about 3 liters of oxygen and 3 liters of carbon dioxide moved across the membrane. There are many factors that allow for the exchange to take place but the lung does its part by providing a large patent surface area by virtue of its alveolar structure.
Each organ system that requires a large working surface area for optimal function has adapted and evolved different structural tricks to accommodate need.. For example the small bowel has primary mucosal folds called called valvulae conniventes increase the surface area by about 3 times. The valvulae themselves have microscopic folds called villi which further increase the working surface by about 10 fold. Each villus has has about 1000 microvilli which increase the surface area by about another 20 fold. Overall the surface area of the 14-20 foot tube also has a surface area of a tennis court.
The kidneys also have devised a mechanism to increase surface area of their side by side epithelial surfaces that act as a filtering mechanism. On the one side, the capillaries bringing blood increase their surface area by convoluting into a ball, while on the other side the receiving membrane of the urinary system becomes a semispherical cup called Bowman’s capsule. The larger the surface area of this membrane, the more effective and efficient the function.
The lungs create the same increased space by bubbling, or ballooning out in the form of the alveoli. The gastrointestinal tract and kidney have more time to do their work. The lungs need all the time they can get since most of the exchange is done during inspiration and even more effectively between inspiration and expiration. The air that is inspired must present itself to the functional surface at large almost immediately, and the exchange has to take place before expiration starts when the air is whisked away to prepare for the next load.
Applied Anatomy
In the clinical realm, there are certain diseases that make the lungs abnormally large and those that reduce the size of the lungs or segments of the lungs.
The lungs will usually take up the available space in the chest so that if one part of the lung is collapsed or surgically removed then the remaining lung will take up the space. Similarly, if one lung is blocked or becomes smaller, then the other becomes hyperinflated resulting in shape and size changes t accommodate the deficiency.
In the COPD group, including emphysema, there is air trapping so that what goes in does not come out because of the structural changes in the lung, resulting in hyperinflation and large lungs. In an acute asthmatic attack there is air trapping making the lungs larger in volume than normal. The diaphragm gets pushed down and becomes flattened. Atelectasis is also part of the disease because thickened mucus, plugs the smaller airways and therefore air cannot get in and subsegmental and collapse occurs. Less commonly the mucus may block the airways at segmental and lobar level with significant consequences to an already compromised system. The diaphragm on the same side of the collapse becomes elevated to the degree that depends on the size of the collapse. The larger the collapse the greater the volume loss in the lungs, the greater the space that needs to be filled in, and hence the greater the elevation of the diaphragm. The concept of filling in space is also witnessed when a patient has had resection of part of the lung. The space usually is filled in by the remaining segments of the ipsilateral lung, but if there is insufficient ipsilateral lung to do the job, (fill in the space) it may be filled in by contralateral lung.
Ashley Davidoff MD TheCommonVein.net 41987L
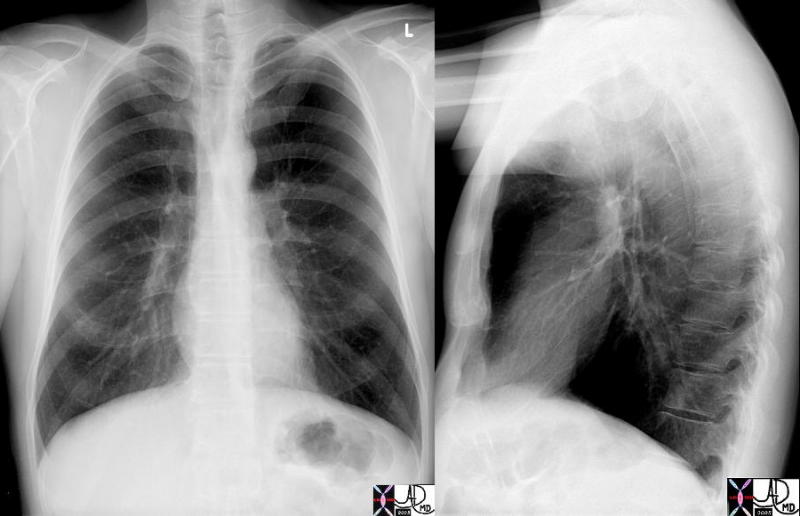
In this patient there is hyperinflation of the lungs, characterized by visualization of more than 10 posterior ribs, increase in the retrosternal airspace, flattening of the diaphragms. The shape of the chest is reminiscent of a pigeon’s chest in that it bulges out, and hence the condition is called pectus carinatum (pigeon chest or a barrel chest.
Ashley Davidoff MD TheCommonVein.net 41987c
Small Lung Due to Elevated Hemidiaphragm
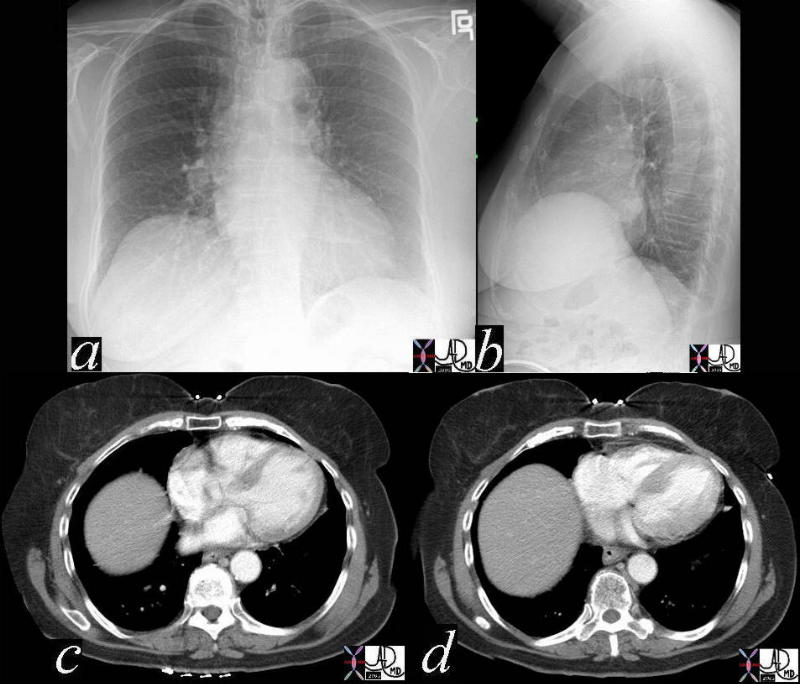
In this patient, the right hemidiaphragm is elevated. Elevation of the right hemidiaphragm may be caused by the atelectasis in the right lung, nerve damage to the right phrenic nerve which supplies the right diaphragm, disease of the right diaphragm itself, or a process under the diaphragm pushing it up. In all instances there is a relative reduction of the lung volume of the right lung. Mostly, when the lungs are otherwise healthy, this has no clinical significance.
Ashley Davidoff MD TheCommonVein.net 41981c
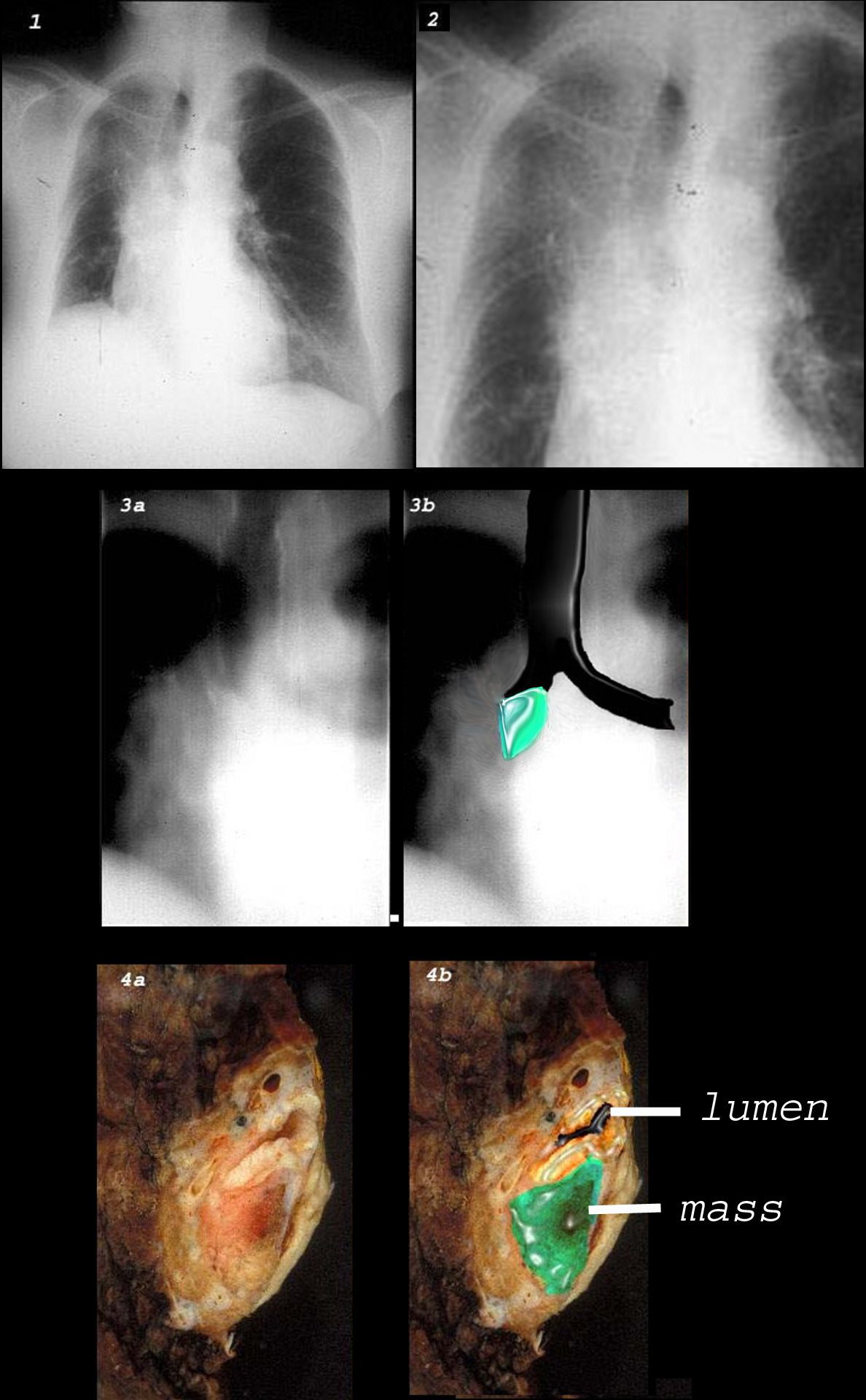
This combination of images shows the manifestations of a malignant mass in the hilum causing compression of the right mainstem bronchus. There is elevation of the right hilum on the CXR, associated with collapse of the anterior segment of the RUL seen as a vague density in the P-A . The tomogram (3a) shows an abrupt cut off of the right mainstem bronchus while the overlay in 3b shows the occlusion of the right mainstem bronchus, the implied tumor overlaid in green. Images 4a and 4b are the correlative gross pathology images showing the tumor in green pushing and occluding the right mainstem
Ashley Davidoff MD TheCommonVein.net 32292cw

3D reconstruction of a normal patient (above) and of a patient with compressive atelectasis (below) The image below is from an 88 year old male with bilateral complex effusions with compressive atelectasis of the lower lobe and portion of the lingula
Ashley Davidoff MD TheCommonVein.net 74238c02