

From the series “People of Israel”
Ashley Davidoff MD
TheCommonVein.net
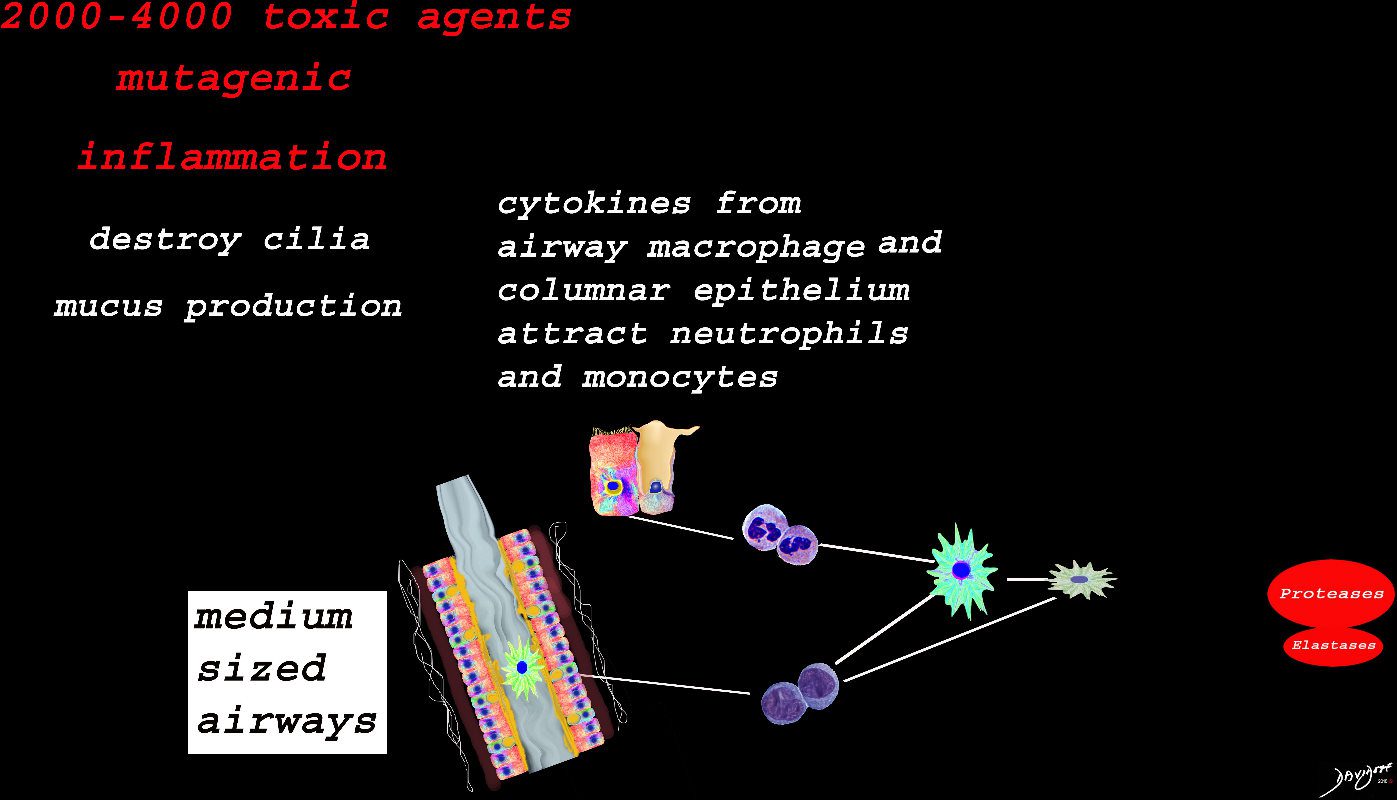
Inhaled smoke contains between 2000-4000 toxic substances. The cancer producing properties are well known. The smoke causes inflammation of the medium sized airways resulting in activation of the resident macrophage in the lumen of the airway, hyperemia of the mucosa, activation of the neutrophils, monocytes, nonresident macrophages, and fibroblasts. Cytokines are released which also induce the secretion of proteases and elastases among many others. Structurally there is destruction of the cilia, hypersecretion of mucus, hypertrophy of the muscularis and mild fibrosis. These findings are the hallmark of chronic bronchitis
Ashley Davidoff
TheCommonVein.net
The alveolus is lined by a simple epithelium – one cell layer thick. There are two types of lining cells; Type 1 pneumocytes are squamous cells that cover 90% of the surface of the inner lining of the lung , and type II cuboidal pneumocytes that are in fact much more numerous than Type I. They are involved in the production of surfactant . In the lumen there are resident macrophages which play a crucial role in the immune system. The mucosa is grounded by a basement membrane and a lamina propria, and connected to the lamina propria and basement membrane of the surrounding capillary. The alveolus is lined by a thin layer of surfactant. (teal blue)
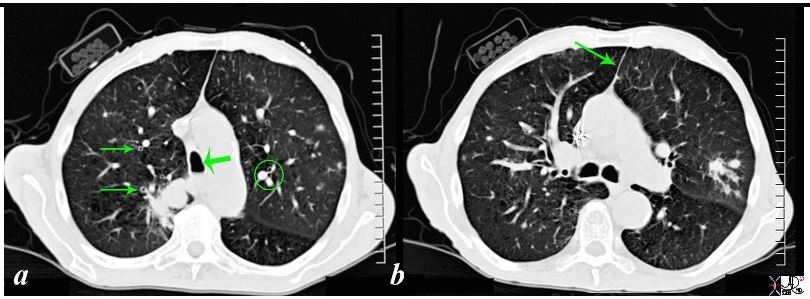
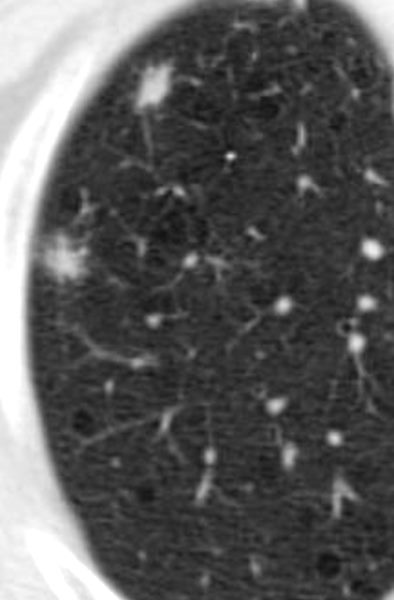
87831c02b02b.8s Among many of the associated and relevant findings in the include the thickened bronchi (arrows on the right in a) compared to the more normal appearing bronchi ringed in the left lung in a, a finding suggesting chronic bronchitis. Noted also is the unusual shape of the trachea (large arrow head in a) where the A-P dimension is significantly larger than the transverse diameter (termed saber trachea) together with a suggestion of an air fluid level in the dependent part of the trachea in a. The air fluid level suggests mucus or artifact in the trachea. The saber trachea together with the thin anterior junction line noted in b is suggestive of hyperinflated lungs that is hallmarks of emphysema. Other findings to note is the discrepancy in size of the arteries that travel with the bronchi – (ringed in a on the left), which is a sign seen in pulmonary congestion. Lastly the lack of subcutaneous tissue suggests a thin emaciated male. code lung cancer smoking anterior junction line bronchi thickened cigarettes shirt pocket mass emaciated saber trachea chronic bronchitis emphysema BAC bronchoalveolar carcinoma bronchioloalveolar carcinoma ground glass opacities GGO radiologists and detectives emaciated CT scan muscle wasting Sherlock Holmes alveolar infiltrate subsegmental
Ashley Davidoff
TheCommonVein.net
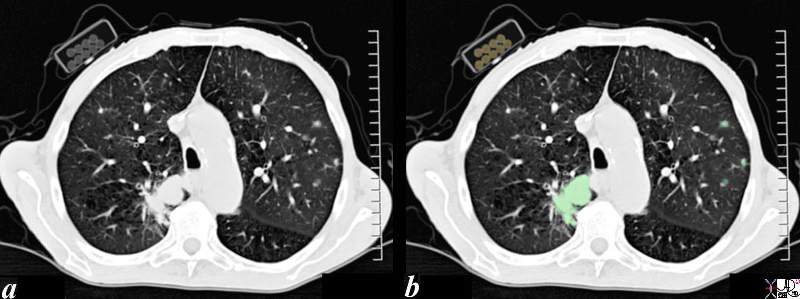
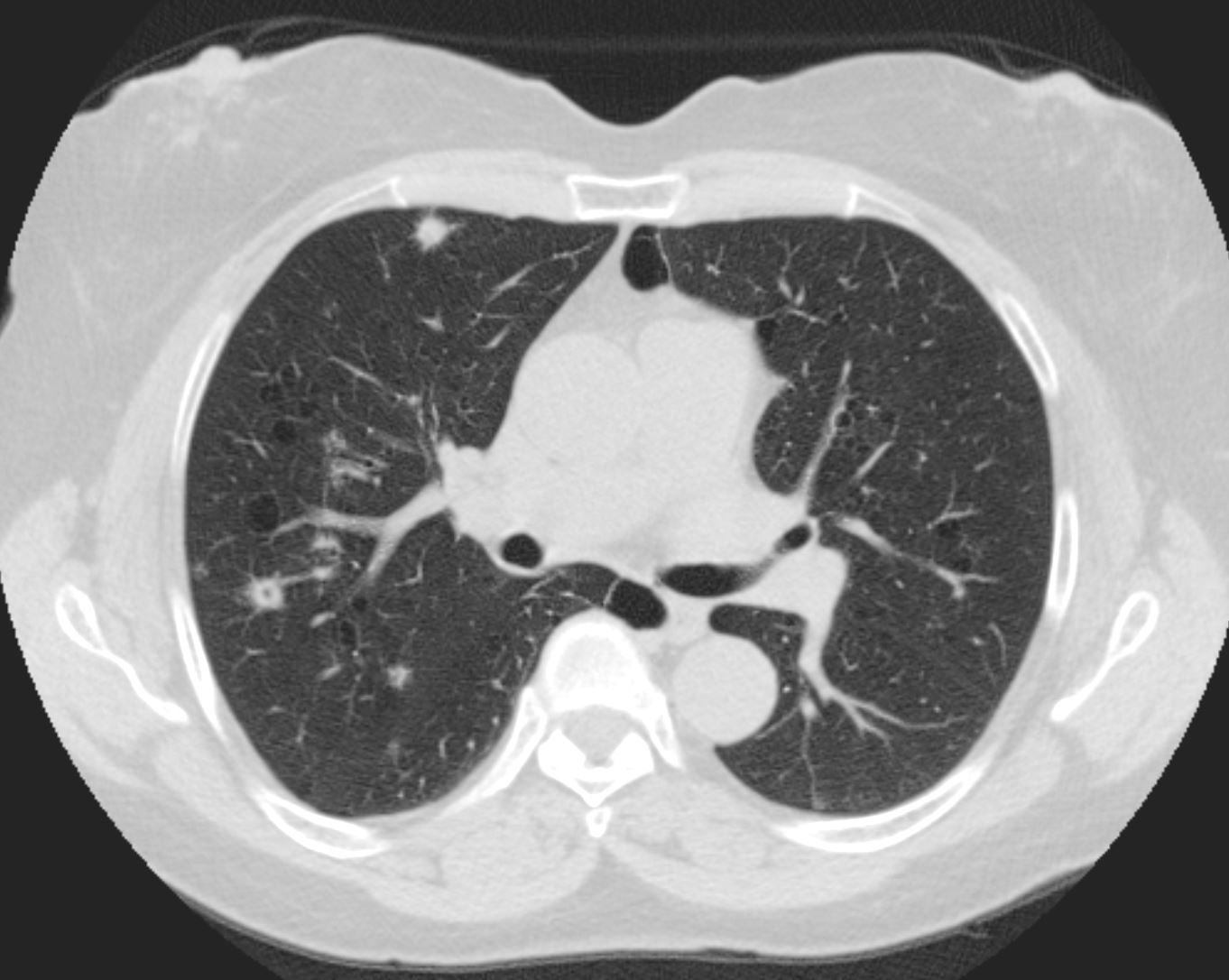
The CT scan through the chest of an 80 year old male shows a large lung mass in the posterior aspect of the right upper lobe (overlaid in green) and3 small nodules in the left upper lobe (overlaid in green). The patient is obviously a smoker and the incriminating pack of cigarettes is identified in his right shirt pocket containing 9 cigarettes. The lung cancer was shown to be an adenocarcinoma The pathology of the nodules may either represent metastatic disease or multicentric foci of bronchioloalveolar cell carcinoma. Associated finding of a thinned anterior junction line suggests hyperinflation and emphysema, and the thickened bronchial walls noted in the right lung suggest chronic bronchitis. Saber shaped trachea is also reminiscent of emphysema. The patient is emaciated, a finding that relates both to his chronic lung disease and his cancer.
Ashley Davidoff MD 87831c01b.8s
TheCommonVein.net

There is thickening of the medium sized airways and mucus in the lumen
Ashley Davidoff
TheCommonVein.net
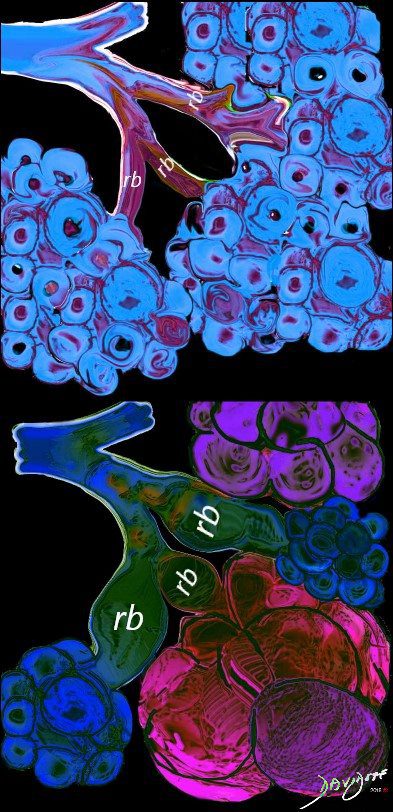
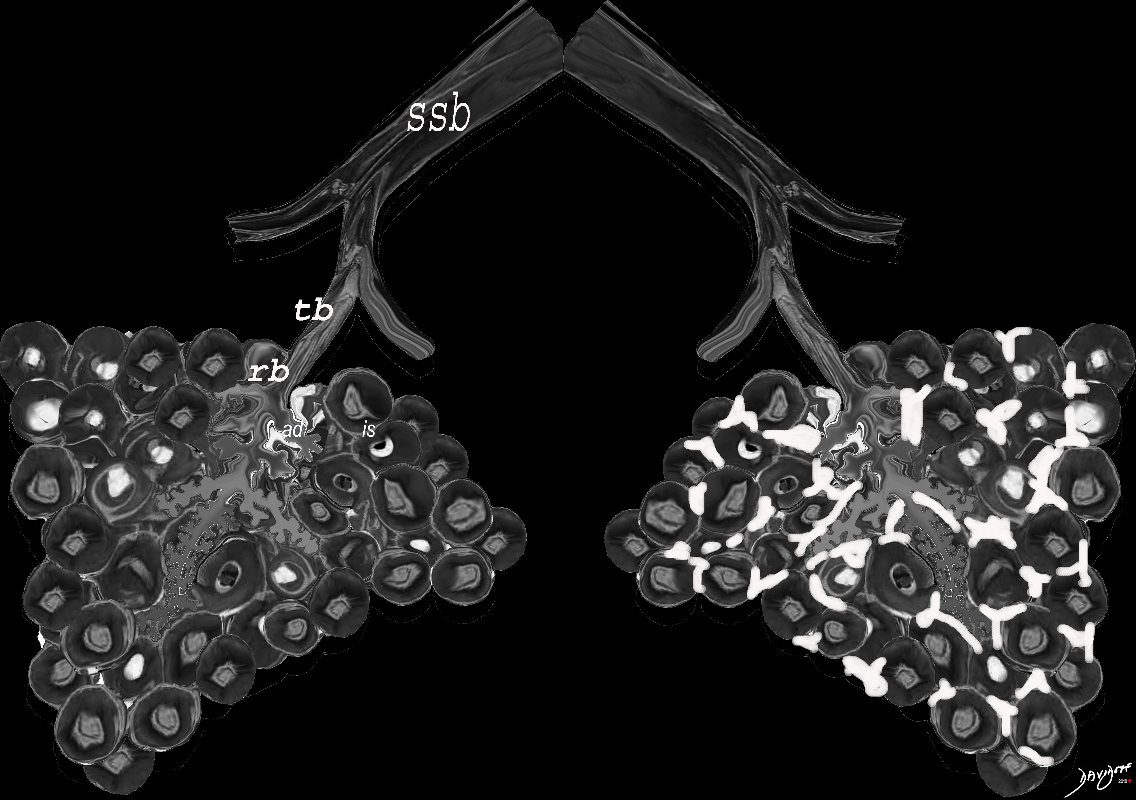
Small (Membranous) Airways (<1mm)
Respiratory Bronchiole, Alveolar Ducts and Alveolar Sacs
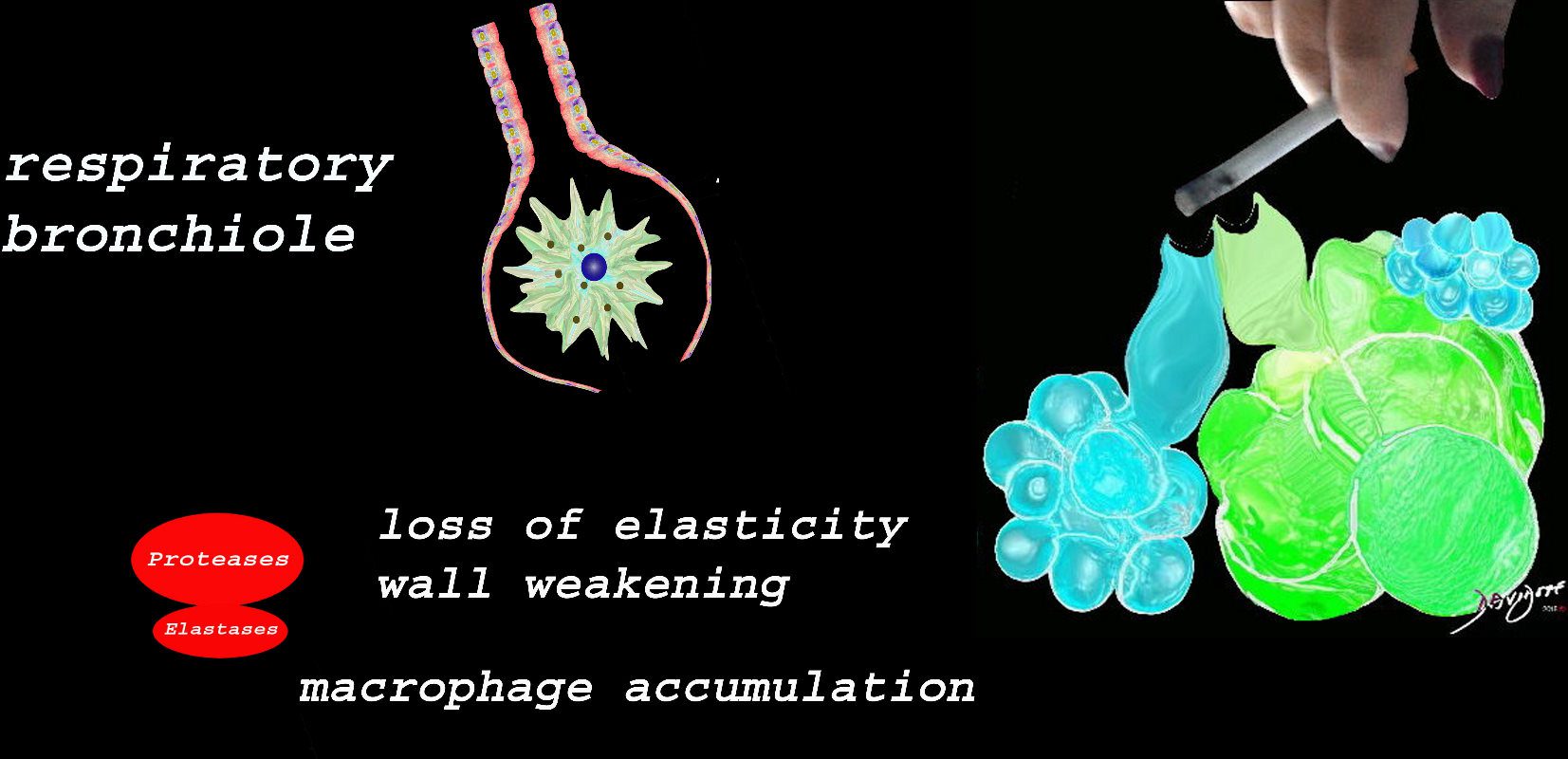
At the level of the membranous airways the effect is predominantly related to the loss of elasticity, and aberrant accumulation of smoking related macrophages.
The weakening and destruction results in emphysema and the abnormal accumulation of smoking related macrophages relates to DIP
Ashley Davidoff
TheCommonVein.net
Emphysema
NORMAL VS CENTRILOBULAR EMPHYSEMA STARTING AT THE RESPIRATORY BRONCHIOLE
Ashley Davidoff MD
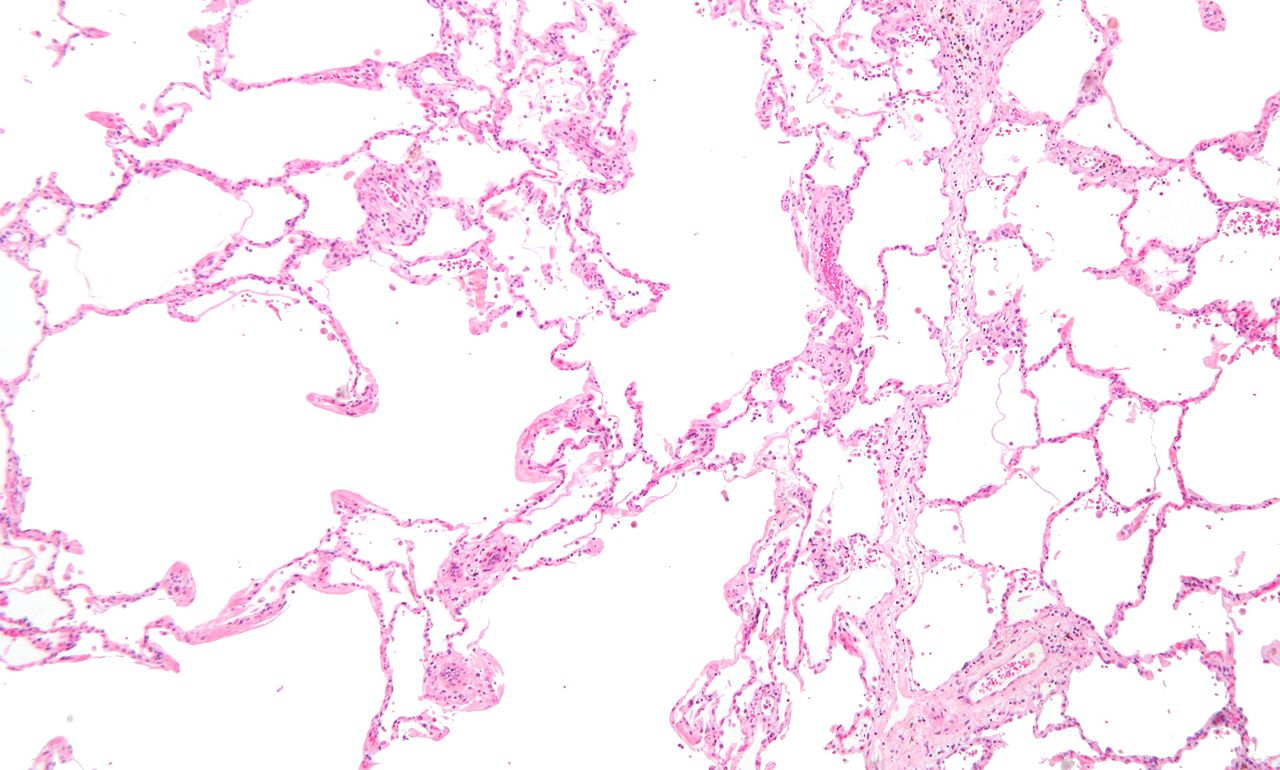
Micrograph showing emphysema (left – large empty spaces) and lung tissue with relative preservation of the alveoli (right)
Courtesy Nephron


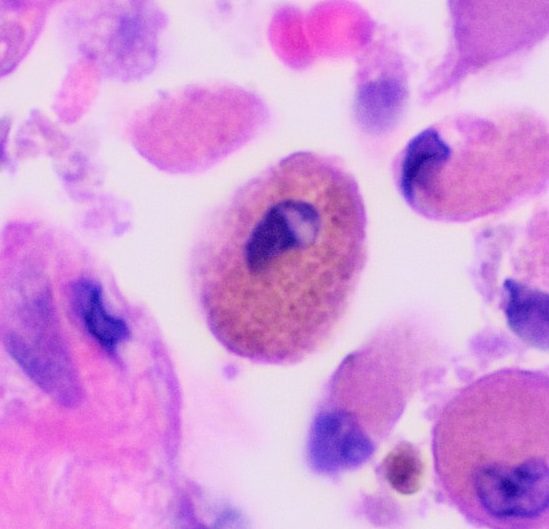
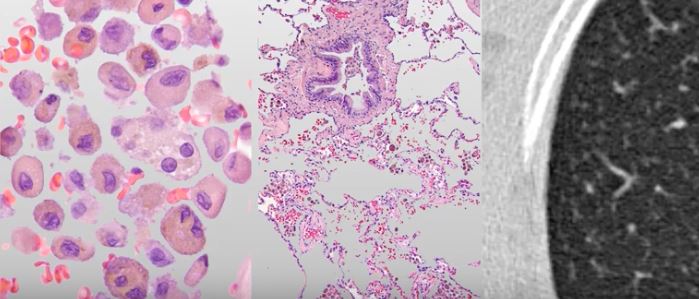
Respiratory Bronchiolitis
Present histologically in all active smokers, is characterised by the accumulation of pigmented “smoker’s macrophages” in respiratory bronchioles and neighbouring alveoli, containing granular, yellow-brown cytoplasmic pigments

Light brown granules in the macrophage is characteristic of the smokers macrophage
Ashley Davidoff
TheCommonVein.net
Courtesy Wiki
web lungs 437
dirty lung appearance
centrilobular lung nodules
ground glass
air trapping
- mild bronchiolar and peribronchiolar alveolar fibrosis that expands contiguous alveolar septa and leads to architectural distortion (RB ILD)
Radiology Key
At the Alveolar Level
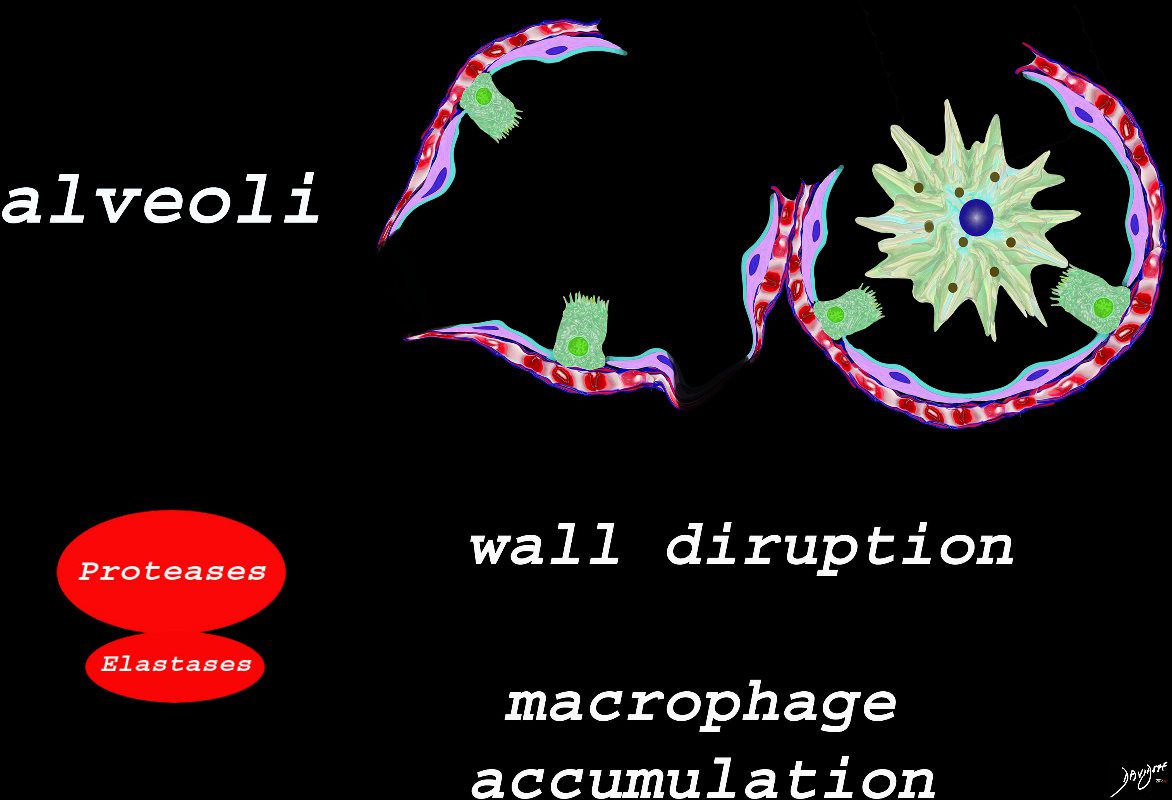
The effect of the proteases and and elastases cause destruction of the alveoli and loss of elasticity, and therefore overall function. The destruction leads to bullous disease
The accumulation of smokers macrophage, and in the case of Langerhans cell histiocytosis leads to space occupation of the alveoli also reducing function
Ashley Davidoff
TheCommonVein.net
lungs-00687-lo res
Desquamative interstitial pneumonitis (DIP)
-
- squams = misnomer
- infiltrates represent alveolar filling with pigmented (smokers) macrophages
- interstitial
- mucosa/submucosa vessels
- pneumonia = “inflammation of the lungs,”
lower lobes.
DIP
Noted are elevated numbers of macrophages within the alveoli of the lung. The alveolar macrophages have a characteristic light brown pigmentation and accumulate in the alveolar lumen and septa regions of the lower lobes of the lungs. The typical effects of the macrophage accumulation are inflammation and later fibrosis with stiffness of the lung
Wiki
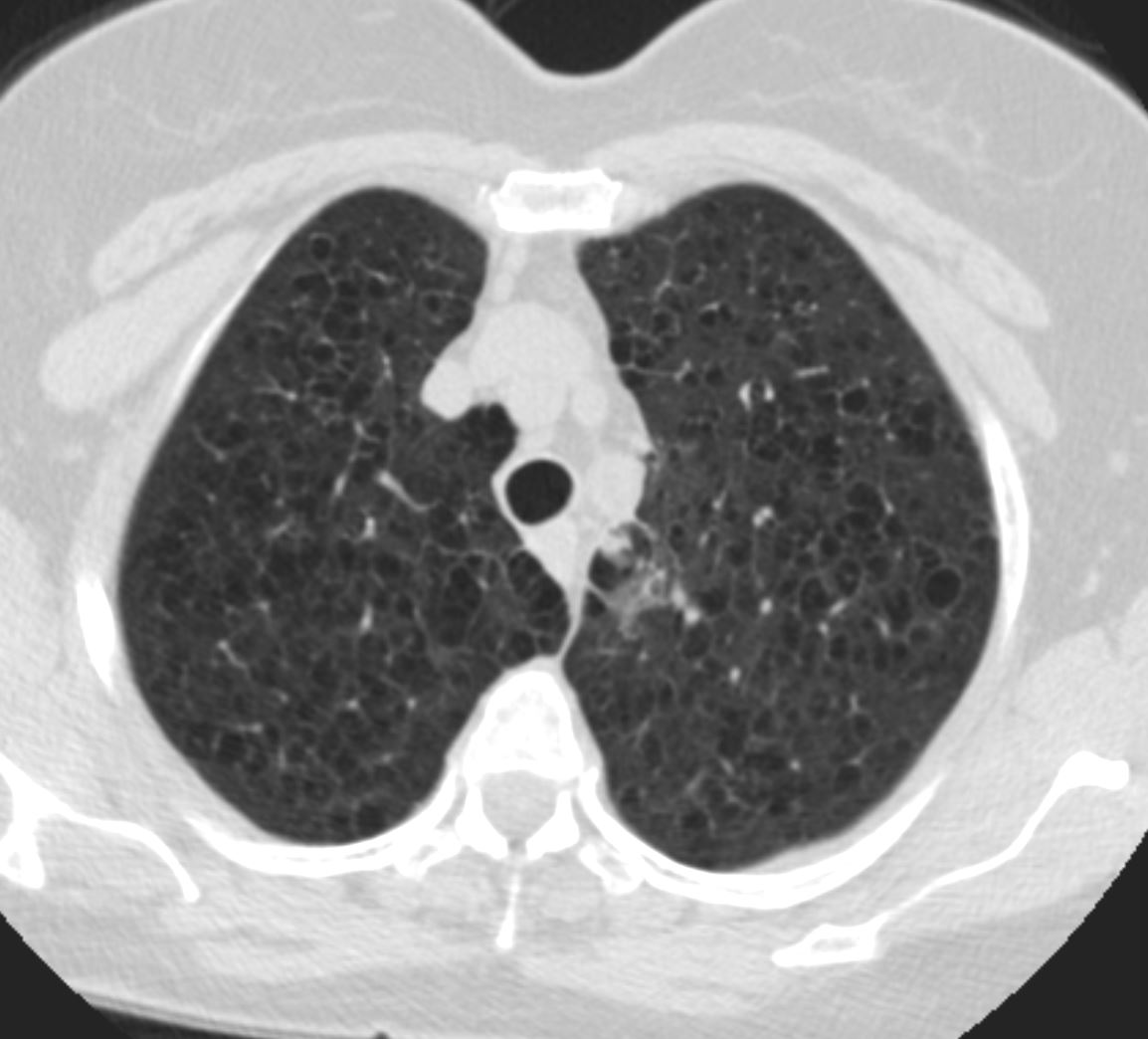
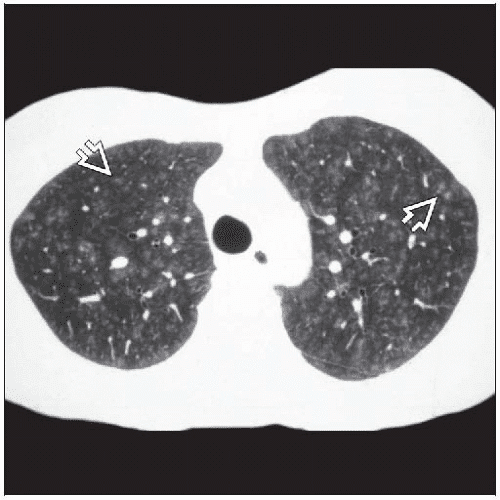
web lungs 436Typical example of high-resolution computed tomography (HRCT) findings in desquamative interstitial pneumonia (DIP). Coronal a) and axial b) computed tomography (CT) slices show bilateral basal and peripheral ground-glass opacity. Some superimposed fine linear opacities are also seen, especially on the left side (coronal slice a)), corresponding with thickened inter- and intralobular septa.
Hellemons M etal Eur Respir Rev 2020; 29: 190181. – September 30, 2020Filled and Half-Filled Alveoli – Differences in Appearance on CT
When the alveoli are fully filled with fluid, tumor, or pus for example, the overall net density will be white, and when adjacent to air filled airways, air bronchograms are visible (left side of image)
When the alveoli are only partially filled, the density of the fluid added to the density of the air results in an overall gray density, and when positioned next to air filled bronchi, there is insufficient contrast to create an air bronchogram and sufficient to enable visualization of the blood vessels. This is called ground glass opacification
Ashley Davidoff
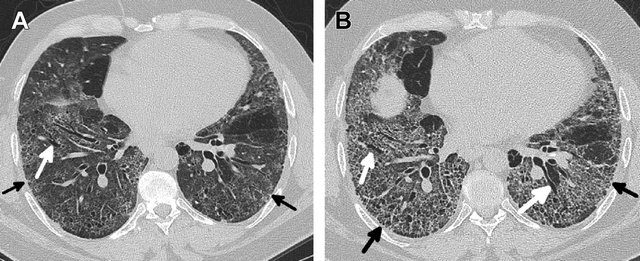
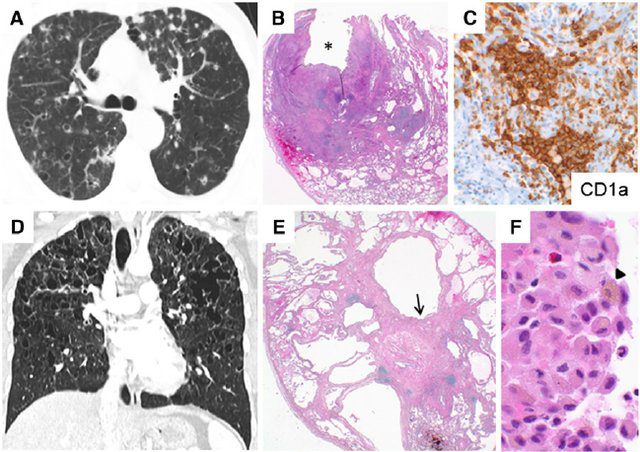
TheCommonVein.netProgression of DIP and pulmonary fibrosis in a 55-year-old male smoker. (A) Axial CT image through the lower lobes from 2012 shows lower lobe predominant ground glass opacity with scattered cystic changes. In addition, there is mild reticulation (black arrows) and bronchiectasis (white arrows), signifying underlying fibrosis. Open lung biopsy showed DIP and a NSIP of fibrosis. (B) Axial CT image from 2015 at the same level as the scan obtained in 2013 shows progressive fibrosis with worsening reticulation (black arrows) and bronchiectasis (white arrows). Explant showed DIP combined with severely fibrotic NSIP.
Kligerman S et al Clinical-Radiologic-Pathologic Correlation of Smoking-Related Diffuse Parenchymal Lung Disease 2016Ground Glass as a result of Interstitial Disease –
When there are extensive interstitial fibrotic changes in the interstitial compartments of the lung which include the and the interalveolar septa, and the supporting interstitium of the lung between the acini and small airways, the overall net density of the region of involvement will be gray, and when adjacent to the black air filled airways, a ground glass appearance will be apparent
Ashley Davidoff
TheCommonVein.net
lungs-00682-lo res- Pulmonary Langerhans cell histiocytosis (PLCH).
- previously called eosinophilic granuloma
- alveolar and bronchiolar infiltration of Langerhans cell
- immature histiocytes – myeloid dendritic cells
- proliferate in the bronchioles and alveolar interstitium, forming granulomas
- leading to destruction of bronchioles and the interstitial alveolar space
- granulomas can cavitate
- cysts with thick walls progressing to
- cysts with thin wills which can become confluent
- upper mid lung involvement
- lower lobe sparing
- costophrenic sparing
- can affect bone
- ambivalent nature
- Can get very sick needing lung transplant
- Can resolve spontaneously
- Lung disease can be associated with lytic bone disease
- Pulmonary Langerhans cell histiocytosis (PLCH).



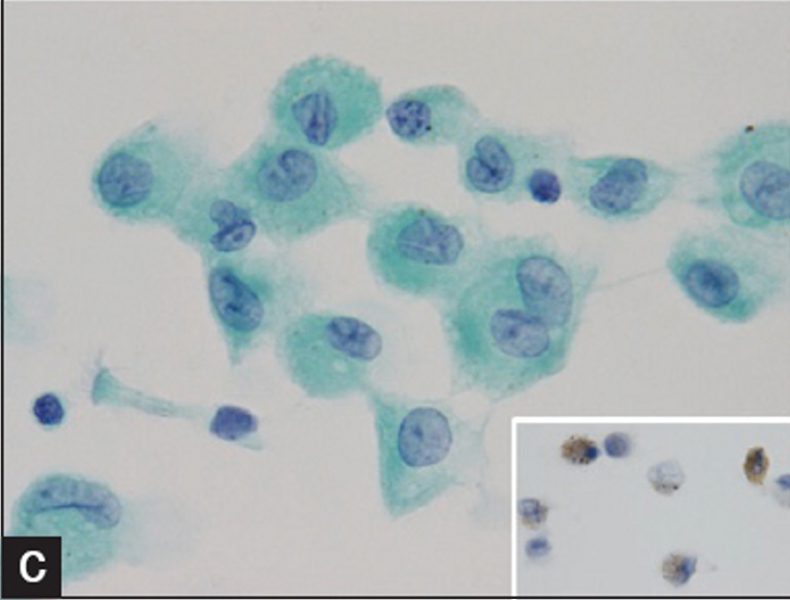
Courtesy IMAGES IN CYTOPATHOLOGY Myunghee Kang et al Cytologic features of pulmonary langerhans cell histiocytosis in bronchial washing: A report of two cases
surrounding interstitium in a patient with PLCH. (Courtesy of Professor
A. Pesci, University of Parma.)
TheCommonVein.net
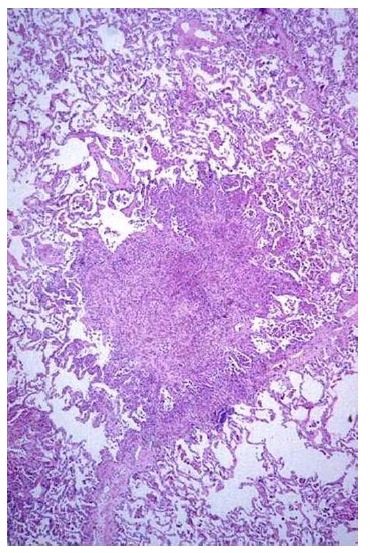
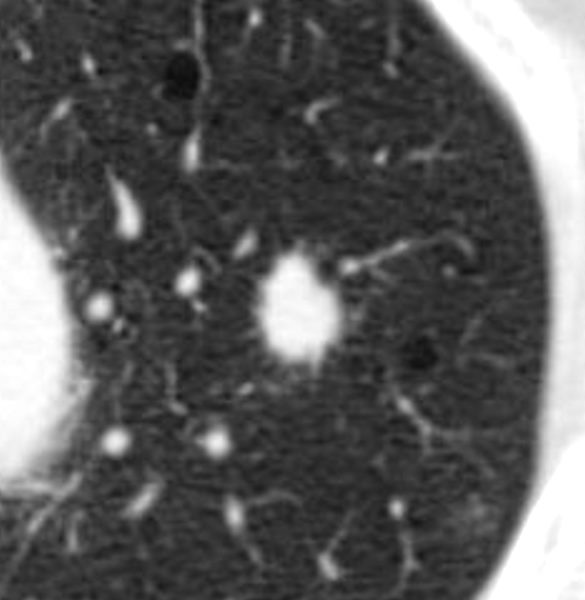
Langerhans Cell is a dendritic white cell with a wavy nucleus that creates granulomas and infiltrates the interstitium. It thus causes spiculated nodules that appear as spiculated nodules on CT
Ashley Davidoff
TheCommon Vein.net
TheCommonVein.net
Cavitaion
Gupta et al Diffuse Cystic Lung Disease: Part I American Journal of Respiratory and Critical Care Medicine 191(12) April 2015
(A) High resolution computed tomographic scan of the lung of a patient with pulmonary LCH showing the association of nodules (some of which are cavitary) and parenchymal cysts. (B) An advanced stage of the disease showing the presence of numerous cysts of various size, some of which are confluent.
Tazi, A et al
Adult pulmonary Langerhans’ Cell Histiocytosis
BMJ – Thorax Volume 55, Issue 5