
SLE and Lungs
Systemic lupus erythematosus (SLE) commonly involves the lung, but chronic pulmonary fibrosis is rare.
Lung manifestation in SLE more commonly result from acute injury to the alveolar-capillary unit, leading to acute lupus pneumonitis and/or alveolar haemorrhage
Histological findings in acute lupus pneumonitis and massive pulmonary haemorrhage syndrome are quite similar, and include interstitial pneumonitis, hyaline membranes, alveolar necrosis, oedema, microvascular thrombosis and focal polymorphonuclear infiltration of arterioles and venules without evidence of vasculitis. Alveolar septal fibrosis may follow repeated episodes of pulmonary haemorrhage, suggesting that there is a continuum between acute and chronic ILD
Acute Manifestations
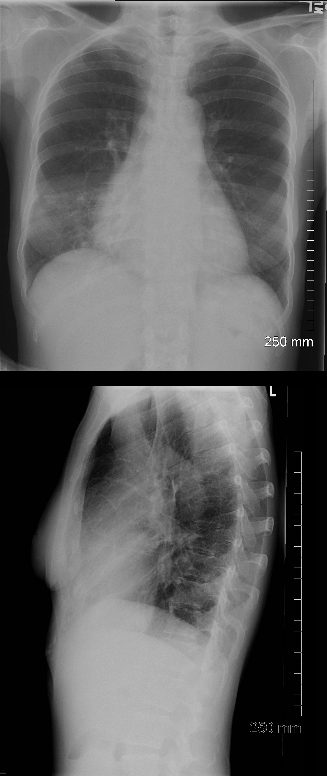
PA and lateral chest X-ray of a 54 year old female with SLE shows bibasilar ground glass infiltrates.
The heart is slightly enlarged and the region of the IVC on the lateral examination is also enlarged
Ashley Davidoff MD
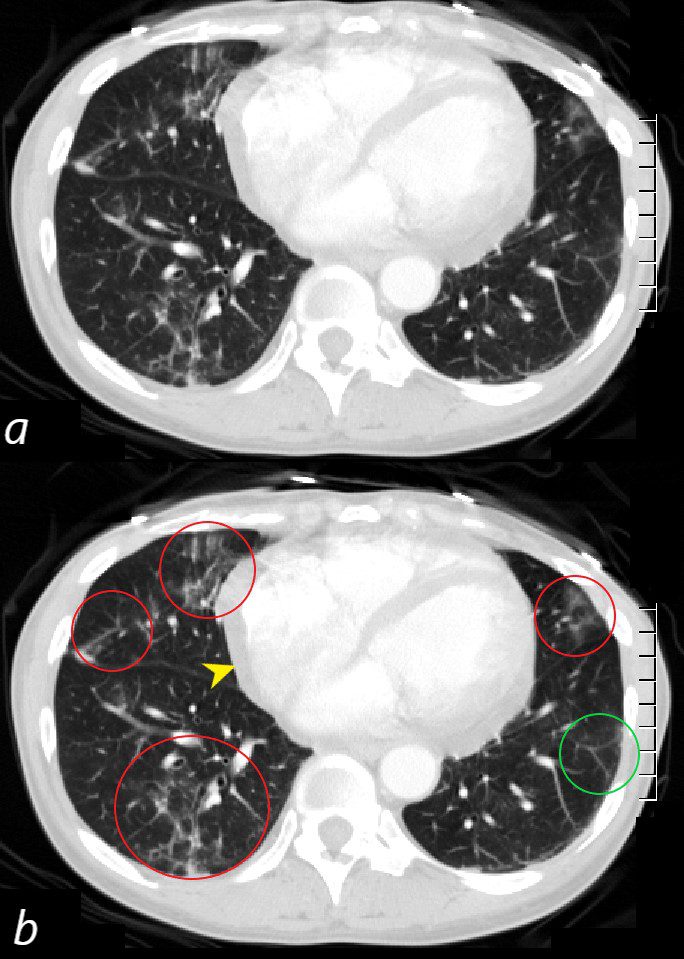
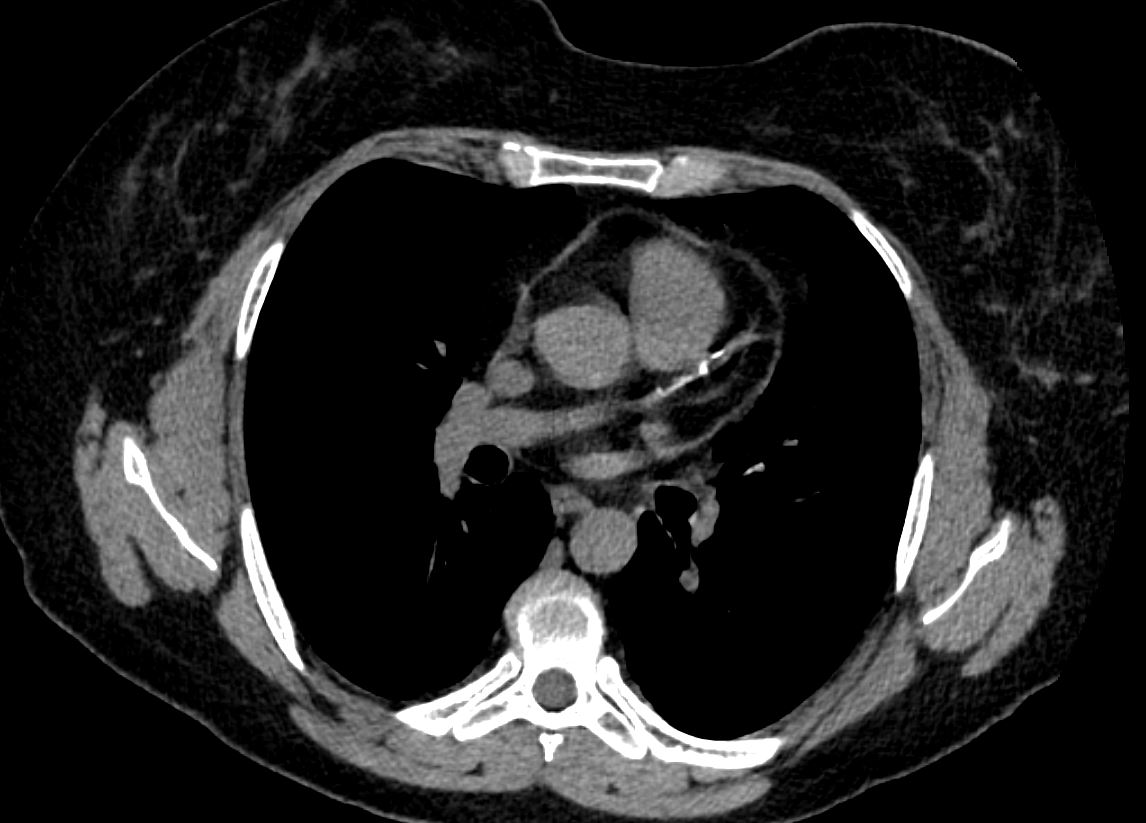
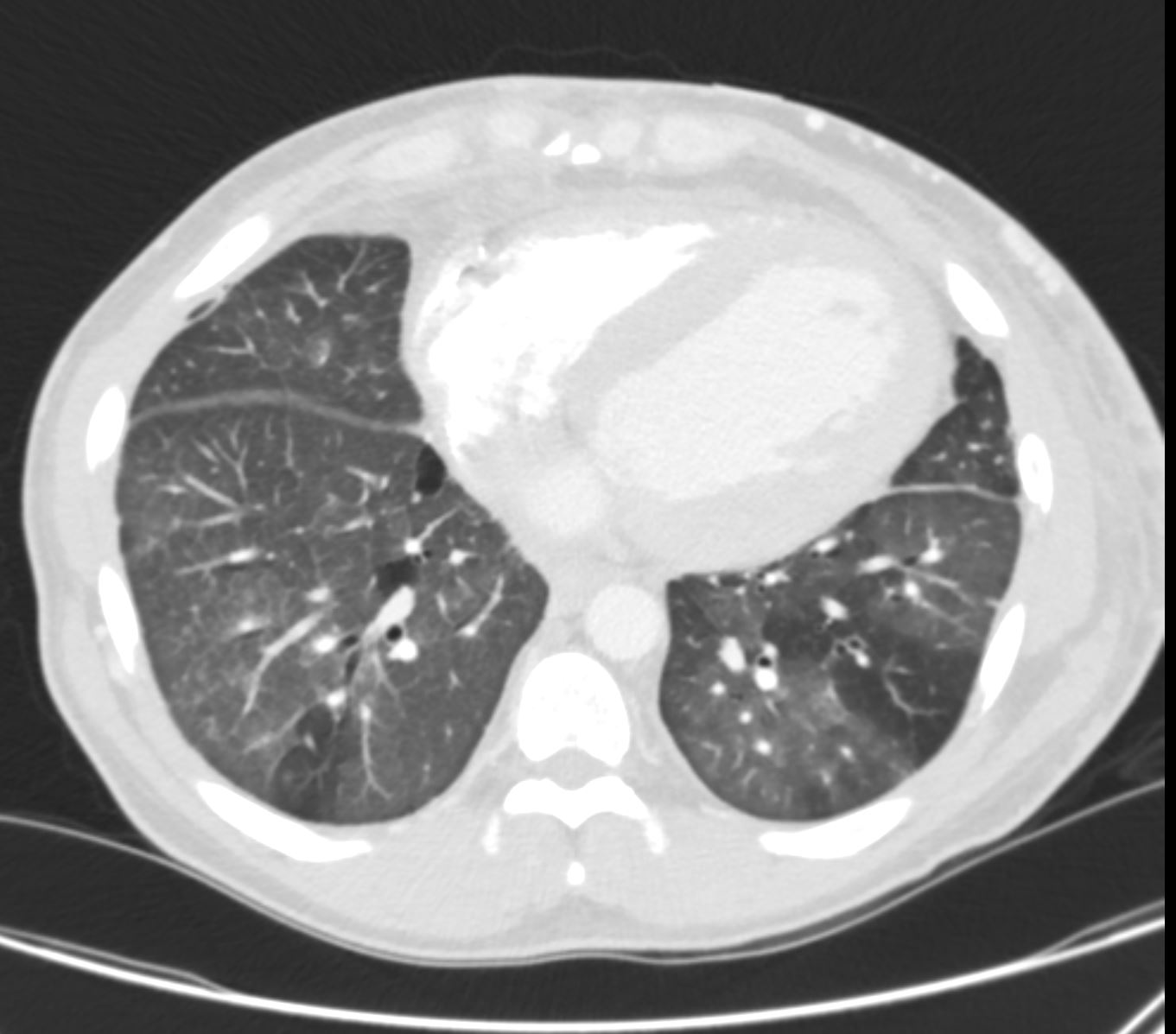
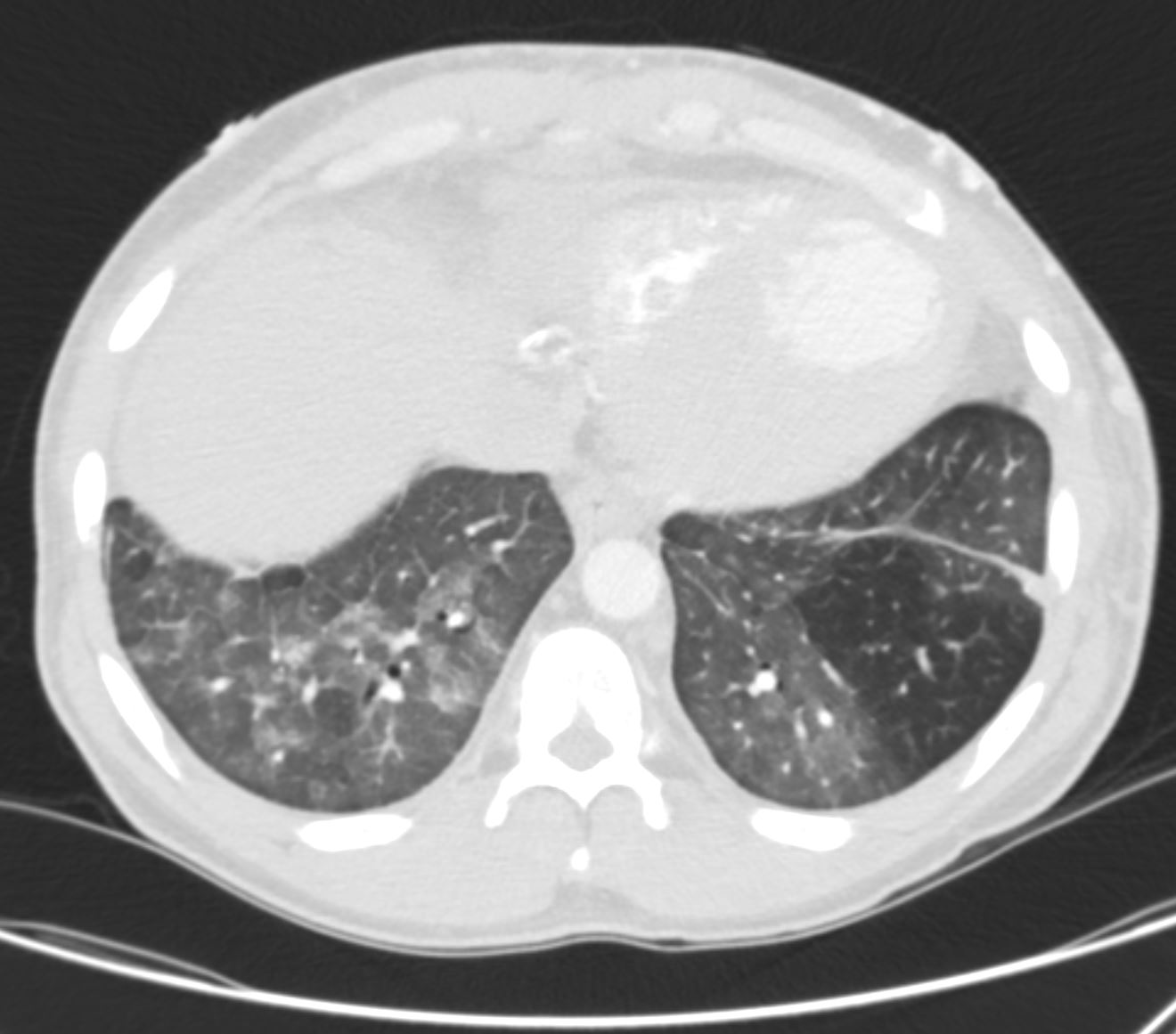
CT scan through the 4 chambers of the heart using lung windows is from a a 54 year old female with SLE. Recent CXR showed bibasilar ground glass infiltrates.
The scan shows basilar multicentric infiltrates with elements of ground glass change and small airway wall thickening (red circles in the right lower lobe middle lobe and lingula, as well as interlobular septal thickening (green circle) in the lateral basal segment of the left lower lobe. A small pericardial effusion is present (yellow arrowhead)
Ashley Davidoff MD
key words
SLE
acute pneumonitis
pericardial effusion
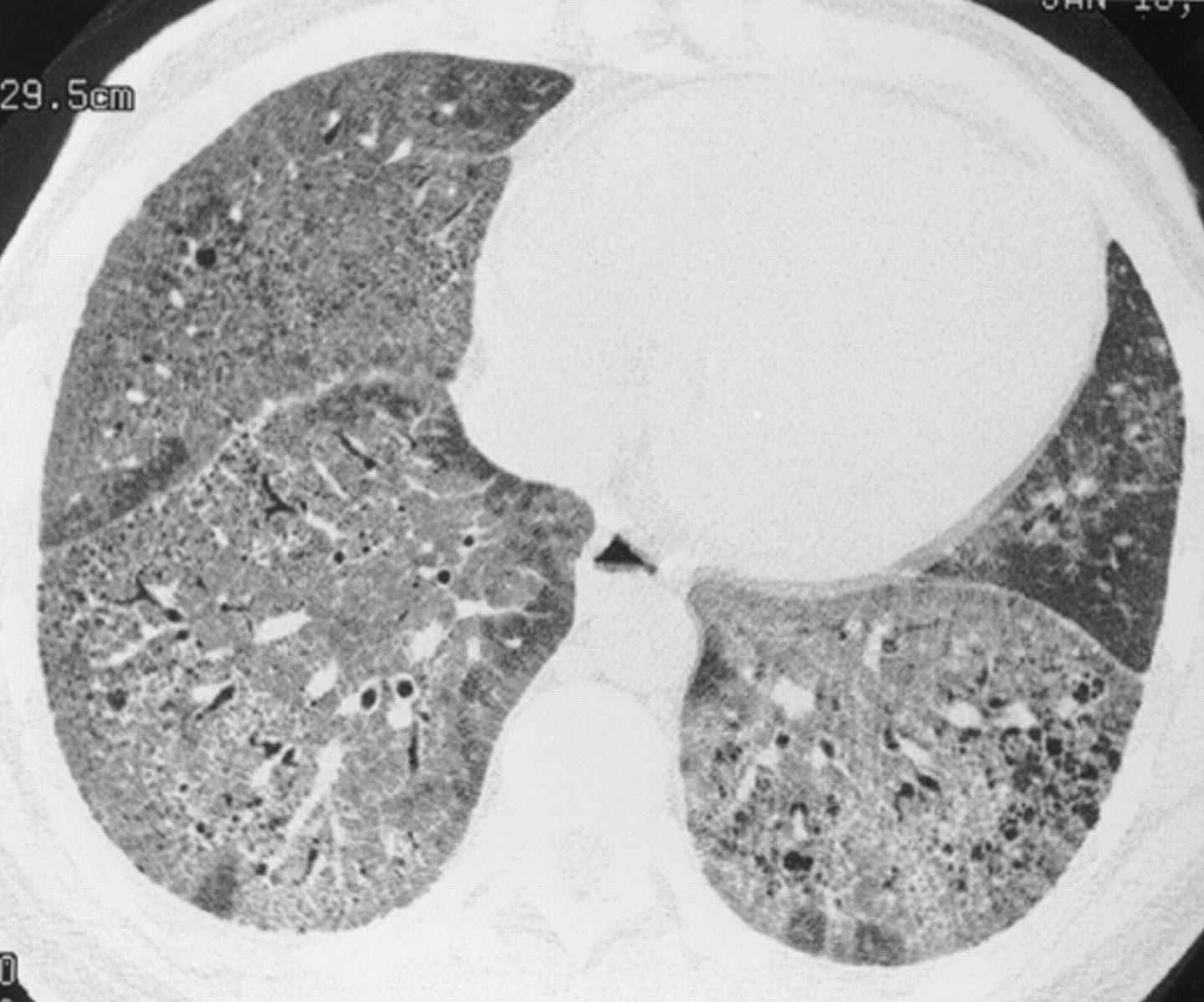
Chronic interstitial pneumonia in a 35 year old woman with SLE. HRCT scan shows extensive ground glass opacities admixed with coarse linear bands and honeycomb cysts. Open lung biopsy confirmed the diagnosis. Ground glass opacities represented a mixture of fibrosis and interstitial mononuclear cell infiltrates. Treatment with corticosteroids, azathioprine, and later cyclophosphamide failed and she subsequently underwent a single lung transplantation.
Keane et al Pleuropulmonary manifestations of systemic lupus erythematosus
BMJ Volume 55, Issue 2
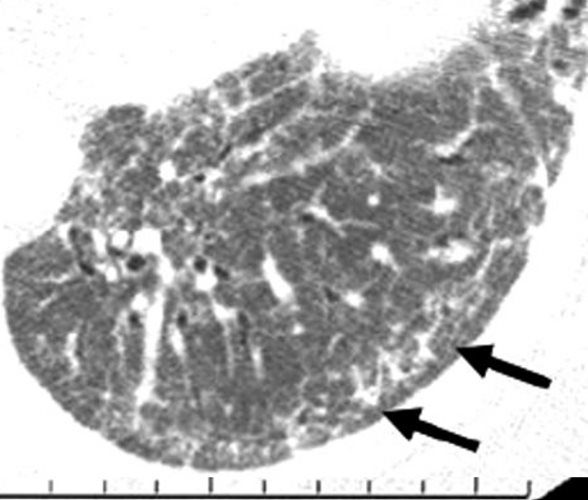
Image from a HRCT scan from a patient with SLE- related ILD. This image of the lower lobes shows predominant abnormalities of diffuse GGO and peripherally based reticular opacities. Note the subpleural sparing (arrows) that is sometimes seen in scans from patients with an NSIP pattern of lung injury.
Research gate
SLE AND PE
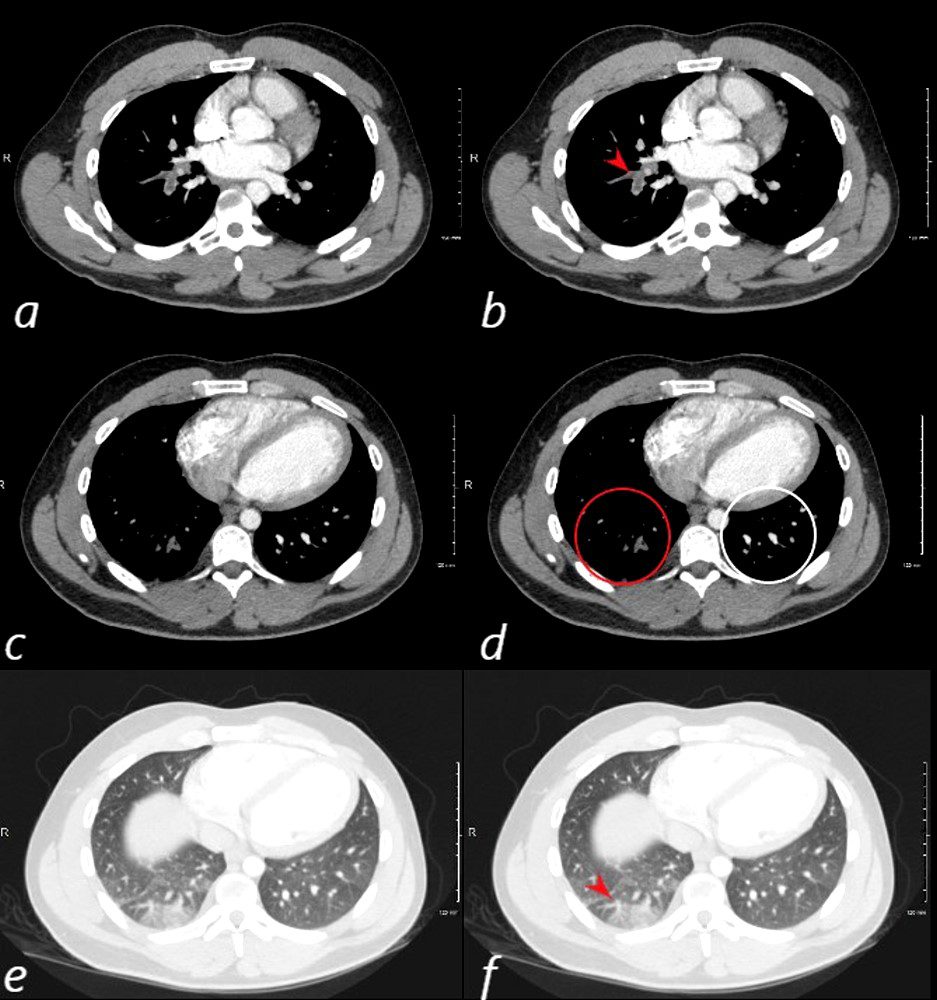
24 year old male with SLE presented with chest pain and dyspnea and initial CT showed occlusive pulmonary emboli to the right lower lobe (a,b, red arrowhead) with total occlusion of the right lobe artery extending into posterior basal segmental vessels (red ring d compared with normal vessels surrounded by white rin (d). An associated wedge shaped ground glass region is noted (e,f red arrowhead) representing either hemorrhage or early infarction
Ashley Davidoff MD
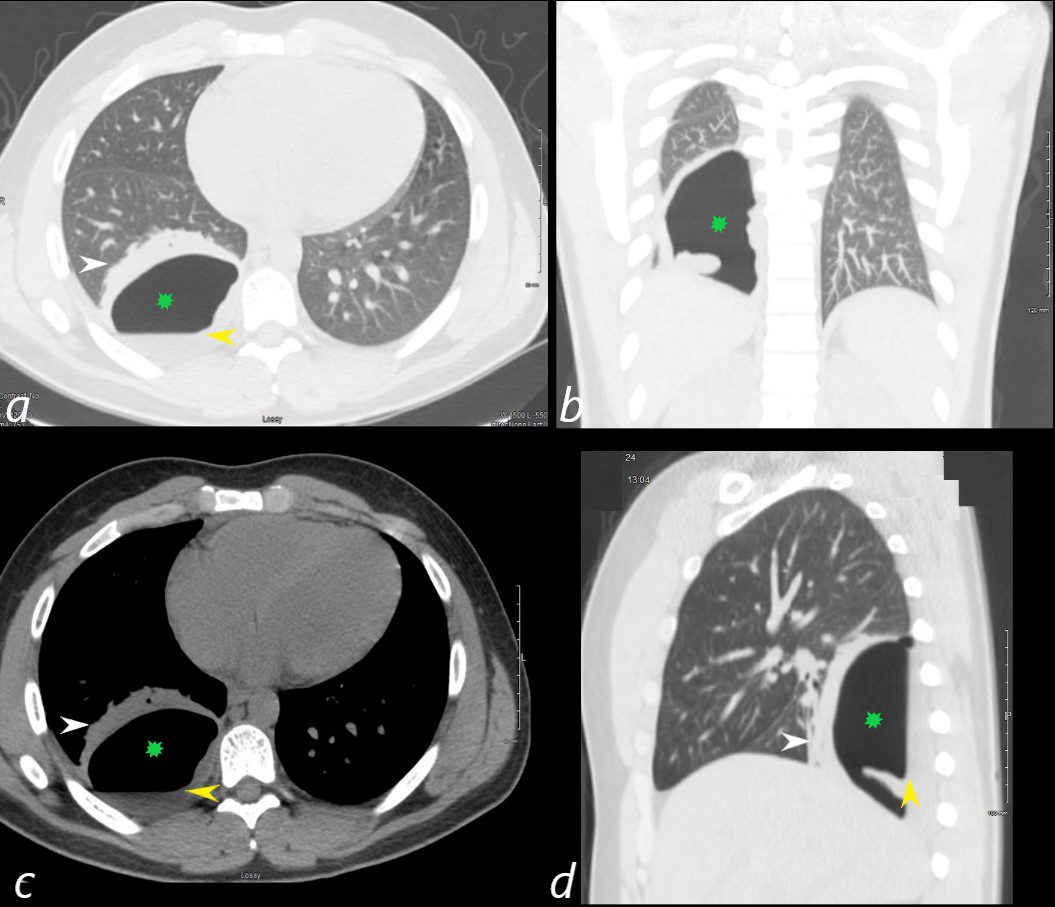
24 year old male with SLE presented with chest pain and dyspnea and initial CT showed occlusive pulmonary emboli to the right lower lobe initially associated with a wedge shaped ground glass region. 2 weeks later this evolved into a bronchopleural fistula, with a loculated pneumothorax in the right lower lobe (green star in a,b,c,d).with an air fluid level (yellow arrowhead in a,c,d) and a region of compressive atelectasis (white arrowhead a,c,d).
Ashley Davidoff MD
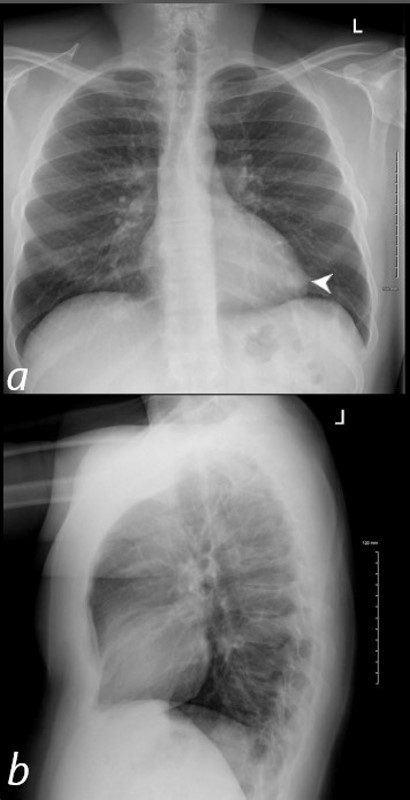
40 year old male with SLE presented with chest pain and dyspnea and initial CXR shows a vague retrocardiac density (a, white arrowhead)
A CT scan that followed showed occlusive pulmonary emboli to the left lower lobe associated with a wedge shaped infiltrate
Ashley Davidoff MD

40 year old male with SLE presented with chest pain and dyspnea and initial CXR showed a vague retrocardiac density
A CT scan that followed showed occlusive pulmonary emboli to the left lower lobe (circled in white) associated with a wedge shaped infarct (red arrowhead)
Ashley Davidoff MD
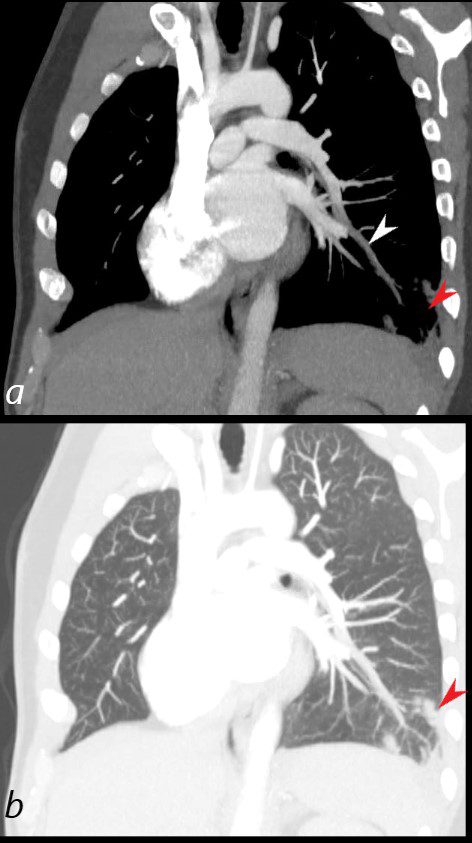
40 year old male with SLE presented with chest pain and dyspnea and initial CXR showed a vague retrocardiac density
A CT scan reconstructed in the oblique projection shows occlusive pulmonary emboli to the left lower lobe (white arrowhead,a) associated with a wedge shaped infarct (red arrowhead a,b)
Ashley Davidoff MD
key words
CT scan
SLE
PE
pulmonary embolism
pulmonary infarct

Ashley Davidoff TheCommonVein.net

Ashley Davidoff TheCommonVein.net
Ashley Davidoff TheCommonVein.net
Mosaic Attenuation in a patient with SLE thought to represent small vessel disease
Ashley Davidoff TheCommonVein.net
Ashley Davidoff TheCommonVein.net
References and Links
Lung Findings
Keane et al Pleuropulmonary manifestations of systemic lupus erythematosus
BMJ Volume 55, Issue 2