
- Primary TB
- caused by inhaling mycobacterium tubercle bacilli which reach the alveoli
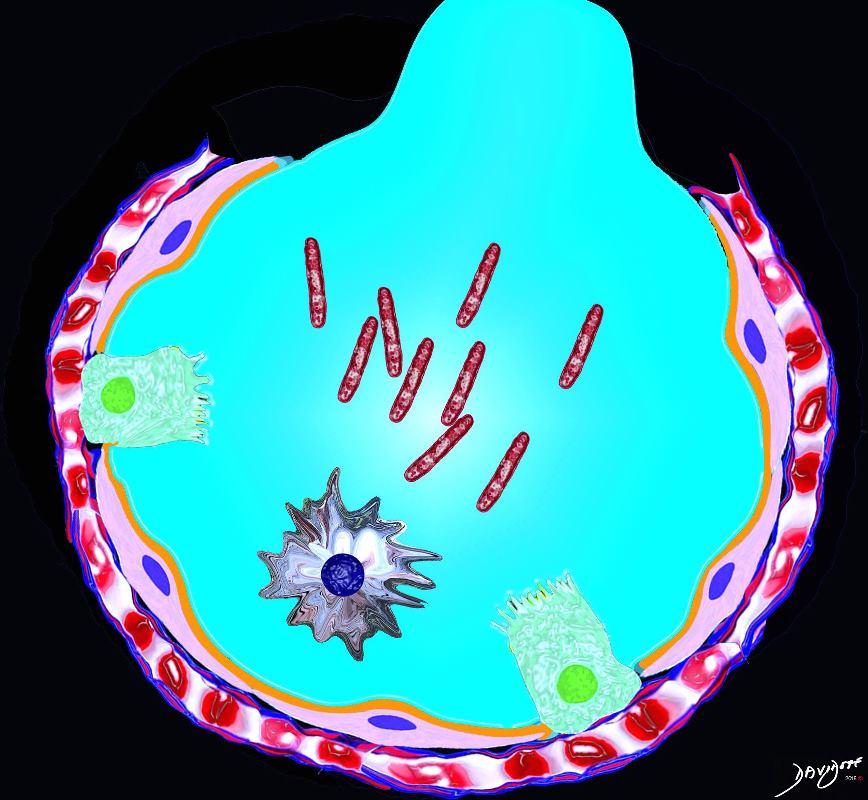
Ashley Davidoff MD TheCommonVein.net lungs-0752
-
- Primary TB may involve
- lung parenchyma,
- lymph nodes
- tracheobronchial tree, and
- pleura – TB pleuritis,
- miliary TB,
- alveolar macrophage
- ingests the bacteria
- bacteria grow inside the alveolar macrophage
- results in an inflammatory response
- immigration of
- monocytes and
- neutrophils
- drainage of bacilli via the lymphatic vessels to the
- lymph node,
- Th1 response is generated,
- resulting in the
- proliferation of
- specific effector lymphocytes
- enter the systemic circulation toward the right heart.
- reach the lung
- attracted to the infected lesions
- lymphocytes activate the
- infected macrophages, which
- kill most intracellular bacilli.
- percentage of the bacilli become dormant and survive inside the necrotic tissue
- neutrophils are attracted to the lesion, initially around the infected foamy macrophages, progressing toward a large degree of infiltration and cavitation
- specific effector lymphocytes
- resulting in
- granuloma
- as a result of macrophage proliferation
- with the bacilli multiplying in the macrophage and associated inflammatory response and
- Macrophages undergo transformation into epithelioid and
- Langehans cells which aggregate with the lymphocytes to form the classical tuberculous granuloma .
- = Ghon focus located
- near major fissures
- upper part of lower lobes
- lower part of upper lobes
- hallmark feature of TB
- near major fissures
- is a characteristic lesion is
- named after Anton Ghon, an Austrian pathologist who first described it in the early 20th century
- appears as a small, well-defined area of lung tissue
- granuloma
- occurs in both
- primary TB
- often accompanied by enlarged hilar lymph nodes
- reactivation TB
- most heal
- may become calcified,
- does not cause any symptoms and
- does not require treatment.
- can be a source of reactivation
- However, if the infection progresses and leads to active TB disease, treatment with antibiotics may be necessary to prevent complications.
- primary TB
- Primary TB may involve
-
-
- lymphadenopathy
- and if uncontrolled the active bacilli reach the draining nodes resulting in
- a Ghon Complex (or primary complex) which may undergo
- fibrosis and calcification = Ranke complex
- lymphadenopathy
-
n

Chest x-ray of Ghon’s complex of active tuberculosis
Basem Abbas Al Ubaidi
“The Radiological Diagnosis of Pulmonary Tuberculosis (TB) in Primary Care”. Journal of Family Medicine and Disease Prevention 4 (1).
- What is primary TB?
- New TB infection or
- active disease in a previously naïve host.
- Symptomatic 30%
- Low Grade – Fever – 70%Pr
- Pleuritic or Chest pain 25%
- Symptomatic 30%
- CXR and CT of primary tuberculosis demonstrates
-
- Hilar lymphadenopathy, (65%)
- Pleural effusion, (30%) and
- Infiltrates (30%) , mid to lower (cavitation uncommon)
- Perihilar
- Right Sided
- Bilateral Rare ( 2%)
-
miliary nodules
middle lobes
upper portion of lower lobes or lower portion of upper lobes
Ghon lesion, sometimes called Ghon focus,
initial tuberculous granuloma formed during primary infection and is not radiologically visible unless it calcifies – this occurs
represents a tuberculous caseating granuloma (tuberculoma) and represents the sequelae of primary pulmonary tuberculosis infection.
Ghon complex.
is a Ghon focus alongside ipsilateral mediastinal lymphadenopathy
Ranke complex
is calcified Ghon complex (Ghon lesion and ipsilateral lymph node) representing a progression of the Ghon complex
radiologically detectable
-
TCV