
Etymology
- Derived from the Old English word “bleb,” meaning a small bubble or blister. In pulmonary terminology, it refers to a small subpleural air-filled space.
AKA
- Subpleural air cyst
What is it?
- A lung bleb is a small, air-filled, subpleural space within the visceral pleura. It is typically less than 1 cm in size and results from localized alveolar rupture or air trapping in the lung periphery.
Caused by:
- Rupture of alveoli due to:
- Smoking-related lung damage
- Chronic obstructive pulmonary disease (COPD)
- Mechanical ventilation with high pressures
- Congenital conditions leading to localized air trapping
- Idiopathic factors in young, otherwise healthy individuals
Resulting in:
- Subpleural air collections
- Weakening of the pleura
- Potential predisposition to spontaneous pneumothorax
Structural Changes:
- Localized air trapping in the visceral pleura
- Thinning or rupture of adjacent alveolar walls
Pathophysiology:
- Lung blebs form when localized alveolar walls rupture, allowing air to dissect into the subpleural space. Repeated alveolar stretching or damage, often from smoking or underlying lung conditions, increases the likelihood of bleb formation. Blebs can compromise pleural integrity, leading to air escape into the pleural cavity and causing pneumothorax.
Pathology:
- Subpleural cystic spaces surrounded by thin fibrous walls
- Associated alveolar damage, particularly in smokers or patients with emphysema
Diagnosis
Clinical:
- Often asymptomatic when small
- May present with sudden onset of pleuritic chest pain and dyspnea if associated with pneumothorax
- Risk factors include smoking and a history of recurrent pneumothorax
Radiology:
- CXR:
- Small, air-filled lucencies near the lung apex, often subtle
- Associated pneumothorax if rupture occurs
- CT:
- Thin-walled, subpleural air-filled spaces, typically ≤ 1 cm
- Predominantly located in the upper lobes or apices
Labs:
- Not routinely used for diagnosing blebs but may help rule out underlying lung conditions in recurrent cases
Management:
- Asymptomatic blebs typically require no treatment
- Surgical intervention (e.g., bullectomy) may be indicated for recurrent pneumothorax
- Smoking cessation is critical to reduce the risk of recurrence
Radiology
CXR
Findings:
- Subtle lucencies at the lung apices
- Potential evidence of pneumothorax (e.g., pleural line separation from the chest wall)
Associated Findings:
- Hyperinflation or signs of underlying emphysema in smokers
- Mediastinal shift if pneumothorax is tension-type
CT
Parts:
- Subpleural areas of the lung, particularly the apices
Size:
- Typically less than 1 cm in diameter
Shape:
- Thin-walled, spherical, or irregularly shaped air-filled spaces
Position:
- Located just beneath the visceral pleura, often in the upper lobes
Character:
- Thin-walled cystic spaces with no significant surrounding soft tissue abnormality
Time:
- Chronic but may present acutely if rupture occurs
Associated Findings:
- Evidence of emphysema or bullae in smokers
- Pneumothorax if rupture leads to pleural air accumulation
Other relevant Imaging Modalities
MRI/PET CT/NM/US/Angio:
- MRI: Rarely used but may help in identifying associated soft tissue changes
- Ultrasound: Useful for detecting pneumothorax but not for identifying blebs
Pulmonary Function Tests (PFTs):
- May show mild airflow limitation if associated with underlying COPD or emphysema
Recommendations:
- CT of the Chest for definitive identification of blebs
- Smoking cessation to prevent recurrence or progression
- Surgical consultation for patients with recurrent pneumothorax
Key Points and Pearls:
- Lung blebs are small, subpleural air-filled spaces often associated with smoking or emphysema.
- They are typically asymptomatic but can predispose individuals to spontaneous pneumothorax.
- High-resolution CT is the gold standard for diagnosis, especially in recurrent cases.
- Smoking cessation and surgical intervention are key management strategies for prevention and treatment of complications.

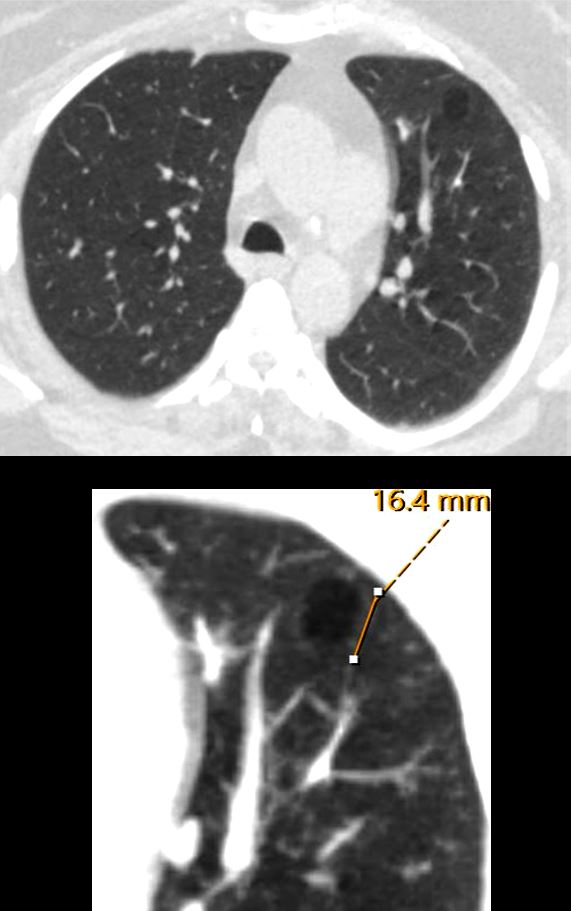
CT scan in the axial plain in a 59 Year old female with emphysema, shows a 1.6cms bleb in the anterior segment of the left upper lobe
Ashley Davidoff MD TheCommonVein.net 136619cL

CT scan in the axial and coronal plains in a 50 year old female shows a 1.cms bleb in the apex of the left upper lobe
Ashley Davidoff MD TheCommonVein.net 137860
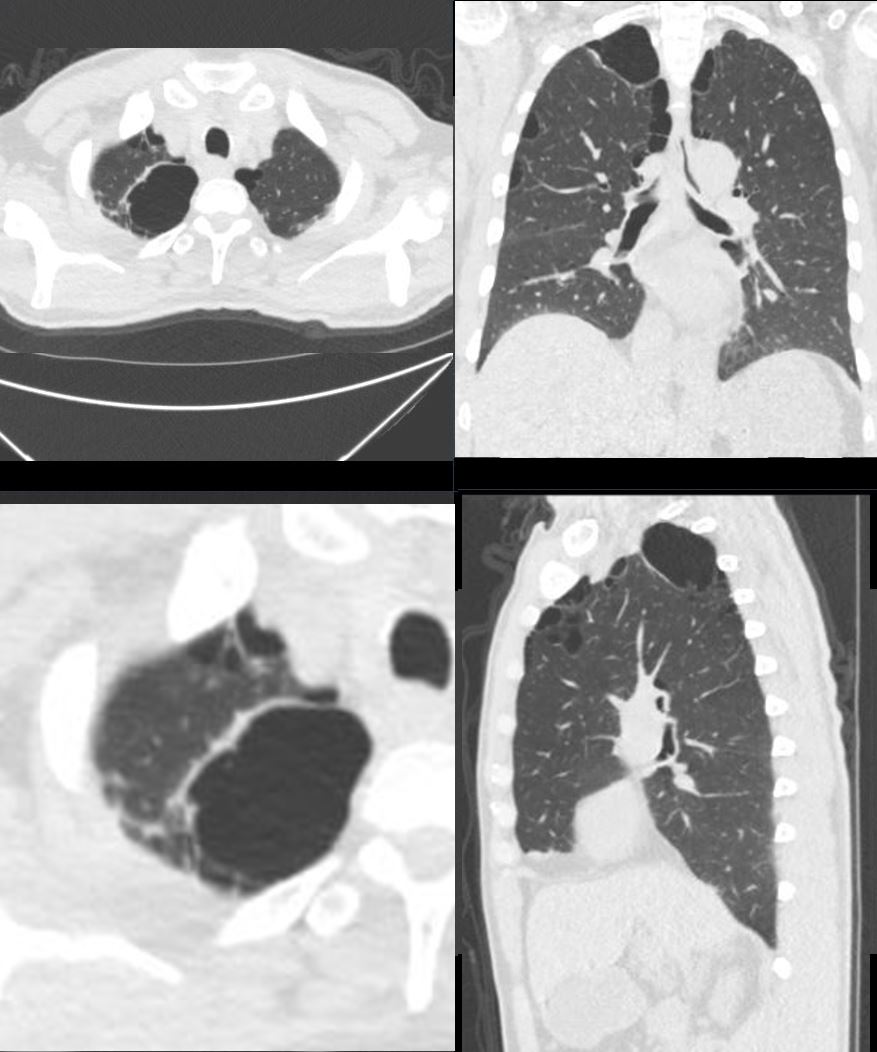
CT scan in the axial and coronal plains in a 55 year old male shows a combination of blebs bulla and paraseptal emphysema most prominent in the apex of the right upper lobe
Ashley Davidoff MD TheCommonVein.net 136929
Links and References
Fleischner Society
Anatomy.—A bleb is a small gas-containing space within the visceral pleura or in the subpleural lung, not larger than 1 cm in diameter (,25).
CT scans.—A bleb appears as a thin-walled cystic air space contiguous with the pleura. Because the arbitrary (size) distinction between a bleb and bulla is of little clinical importance, the use of this term by radiologists is discouraged.