
Adenocarcinoma of Left Lung with Bilateral Lymphangitic Spread

CXR of 50-year-old female with primary adenocarcinoma of the left lung shows extensive consolidation of the left lower lung field with diffuse bilateral reticulonodular changes reminiscent of lymphangitic spread of disease bilaterally
Ashley Davidoff MD TheCommonVein.net 158Lu 131022
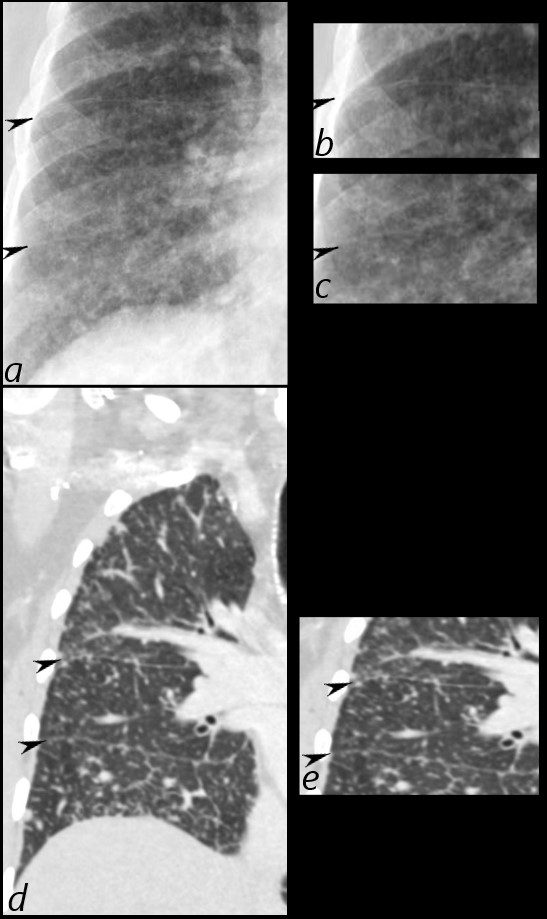
50 year old female with primary adenocarcinoma of the left lung presenting with pneumonic consolidation. And diffuse reticulonodular changes bilaterally
Images from the CXR (a, and magnified in b and c) show thickening of the fissures of the right lung (black arrowheads) with diffuse reticulonodular changes.
The coronal CT scan (d, magnified in e) confirm nodular thickening of the fissures (black arrowheads). In addition there are nodular changes with centrilobular location and along the interlobular septa, reminiscent of lymphovascular spread. These findings are consistent with the diagnosis of lymphangitis carcinomatosa
Ashley Davidoff MD TheCommonVein.net 158Lu 131022c
Halo Sign Around a Malignant Mass
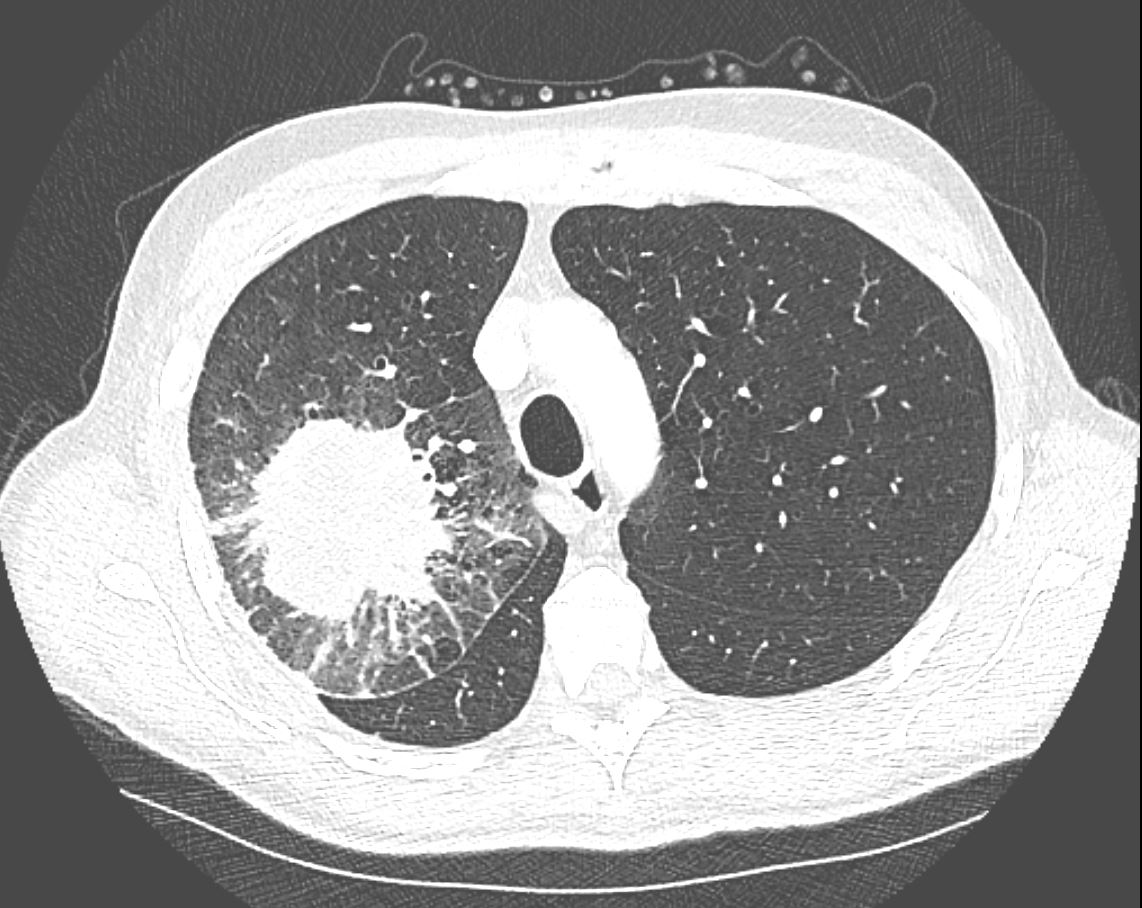
CT in the axial plane demonstrates a large, spiculated mass in the right upper lobe with surrounding halo likely reflecting hemorrhage or lymphatic edema around the mass. In addition, there is evidence of irregular interlobular septal thickening likely reflecting lymphatic invasion and indicating lymphangitis carcinomatosa. There is irregular thickening of the major fissure suggesting involvement.
Ashley Davidoff MD TheCommonVein.net 135865
69 Year Old Male with NSCLC Metastatic to Adrenal and Brain
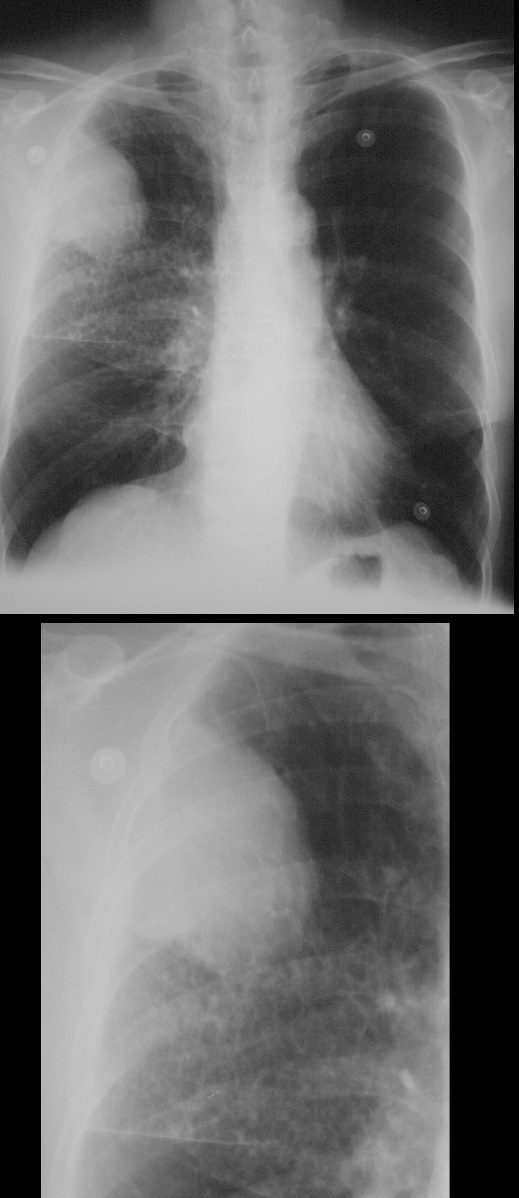
67-year-old man with prior history of bladder cancer. Frontal chest X-ray (CXR) shows a large right upper lobe lung mass. Inferior to the mass, there a polygonal pattern of the intertstitium suggesting lymphangitis carcinomatosis
Ashley Davidoff MD TheCommonVein.net 32270c01
67-year-old man with prior history of bladder cancer. CT scan in the axial plane shows a large right upper lobe lung mass. Posterior to the mass, the interlobular septa are thickened.. These findings suggest lymphangitis carcinomatosis. Peribronchial thickening of the apical segmental airway may be due either to lymphangitis or chronic bronchitis There is background evidence of centrilobular emphysema, dominant in both upper lobes giving an internal comparison of the normal vs abnormal size of the interlobular septa
Ashley Davidoff MD TheCommonVein.net 32285c
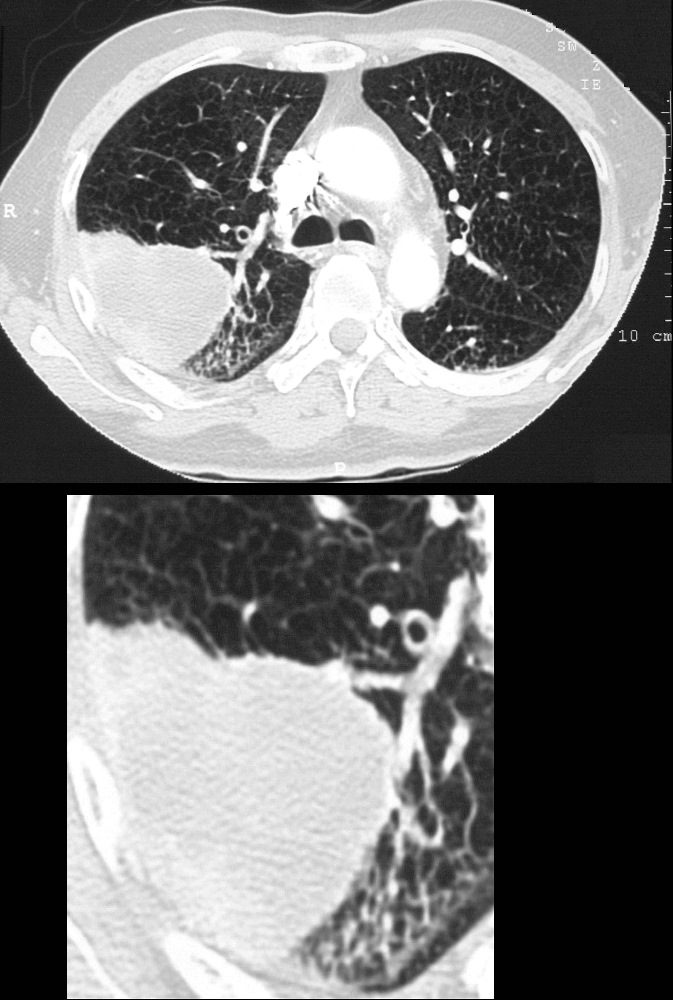
67-year-old man with prior history of bladder cancer. CT scan in the axial plane inferior to the lung mass shows extensive irregular thickening of the interlobular septa magnified in the right lower panel. These findings reflect lymphangitis carcinomatosis. There is background evidence of centrilobular emphysema, dominant in both upper lobes. A magnified view in the right lower panel offers an internal comparison of the abnormal vs the normal size and shape of the interlobular septa
Ashley Davidoff MD TheCommonVein.net 32287c
Known Head and Neck Cancer Metastases –
Abnormal Secondary Lobules –
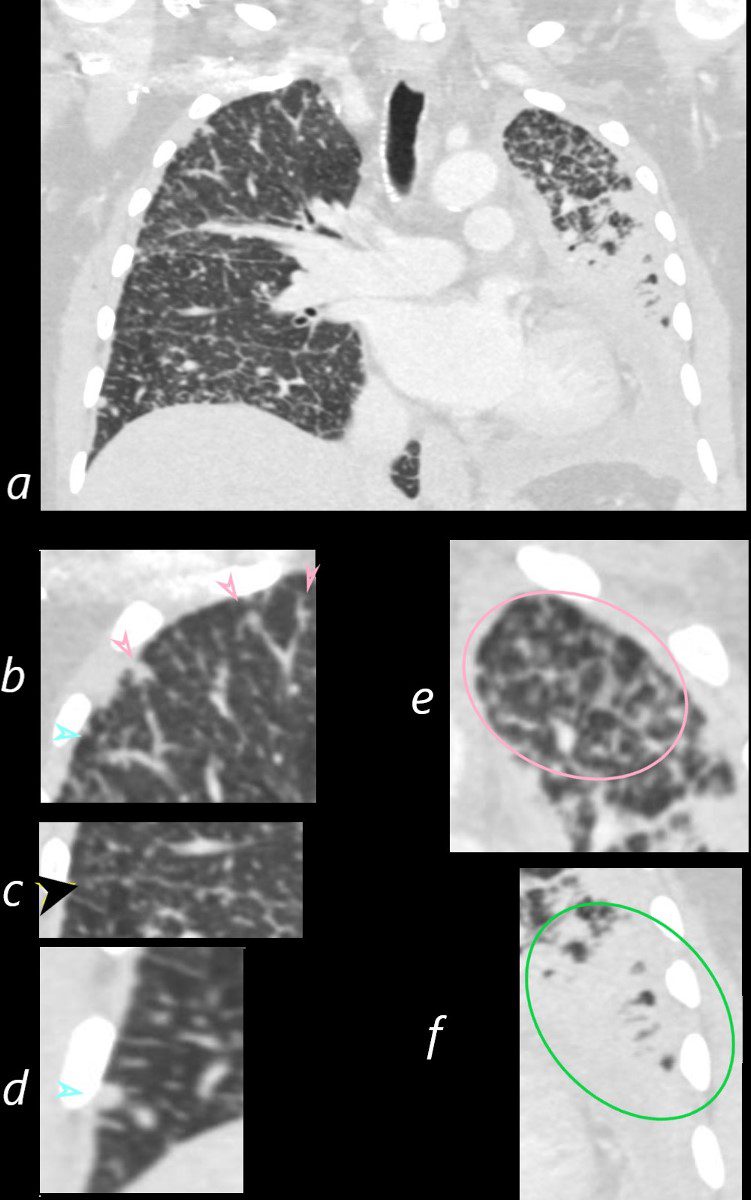
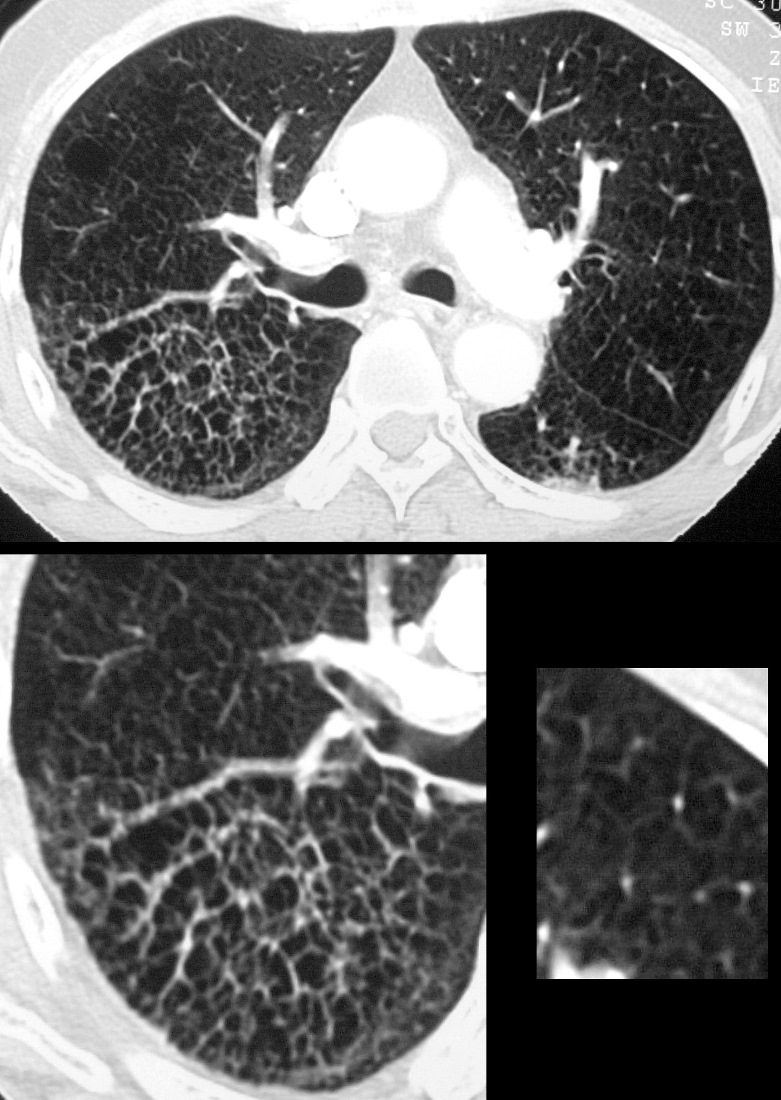
CT of the chest in the axial plane of a 53year old male with head and neck cancer. In the anterior segment of the right upper lobe are a few secondary lobules with prominent centrilobular nodules and irregularly thickened septa
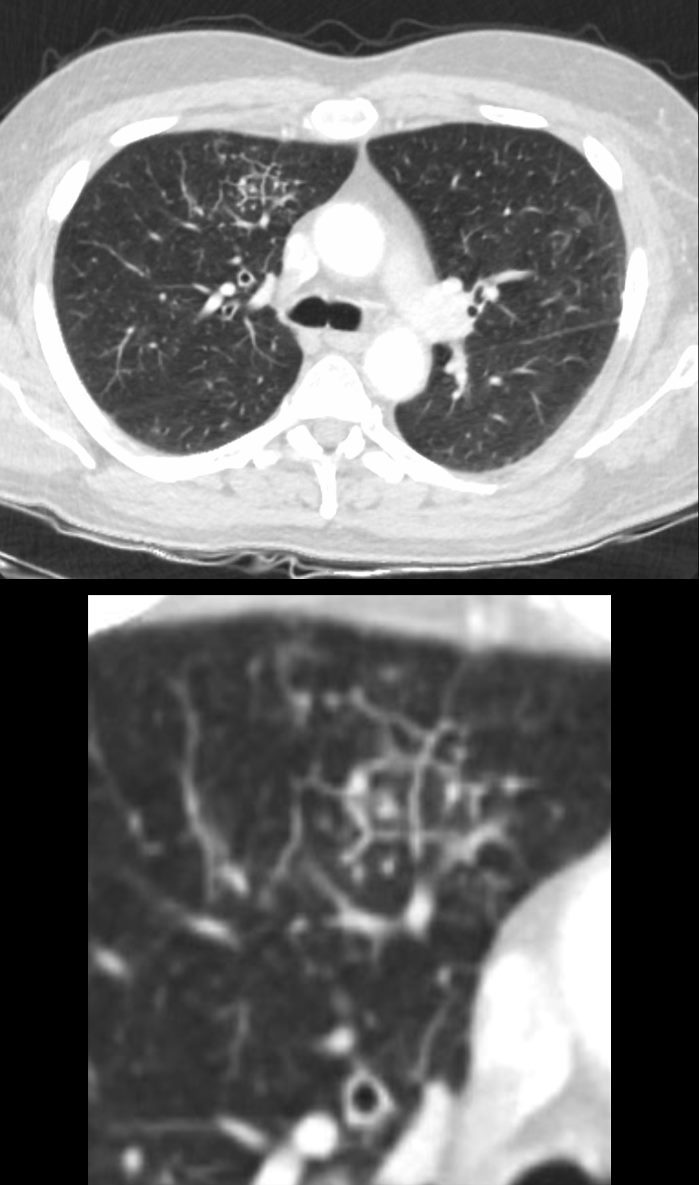
Abnormal Secondary Lobules –
CT of the chest in the axial plane of a 53year old male with head and neck cancer. In the anterior segment of the right upper lobe are a few secondary lobules with prominent centrilobular nodules and irregularly thickened septa
Ashley Davidoff MD TheCommonVein.net 013Lu 136054c
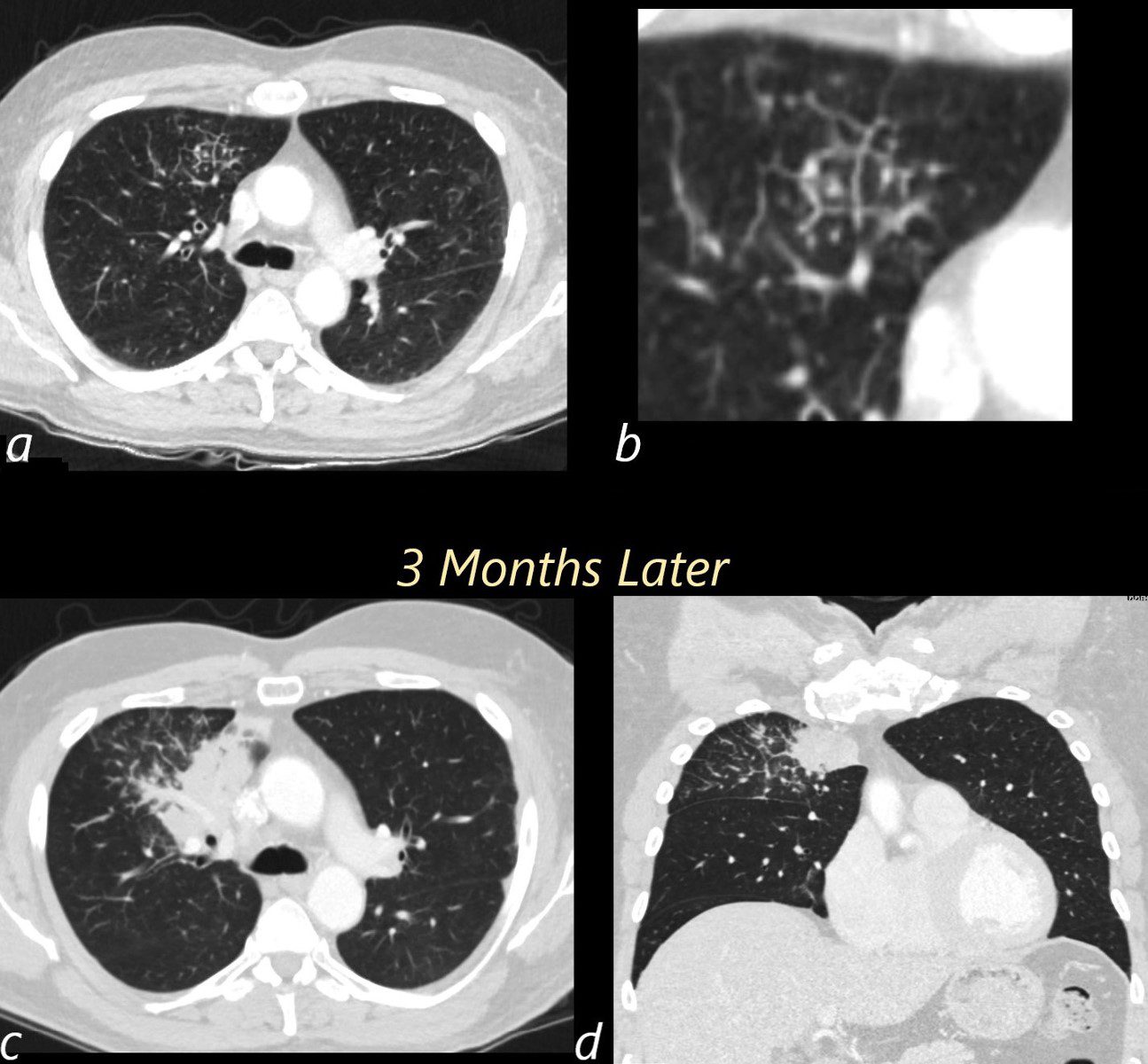
Images a and b show the initial presentation of disease characterised by right upper lobe changes in a few secondary lobules characterised by thickening of the septa and prominence of the centrilobular nodules. 3 months later (c and d) the patient presented with a cough A large right upper lobe consolidative mass and progressive involvement of more secondary lobules with thickening of interlobular septa is noted. These findings likely reflect lymphangitis carcinomatosa
Ashley Davidoff MD TheCommonVein.net 013Lu 13606cL