
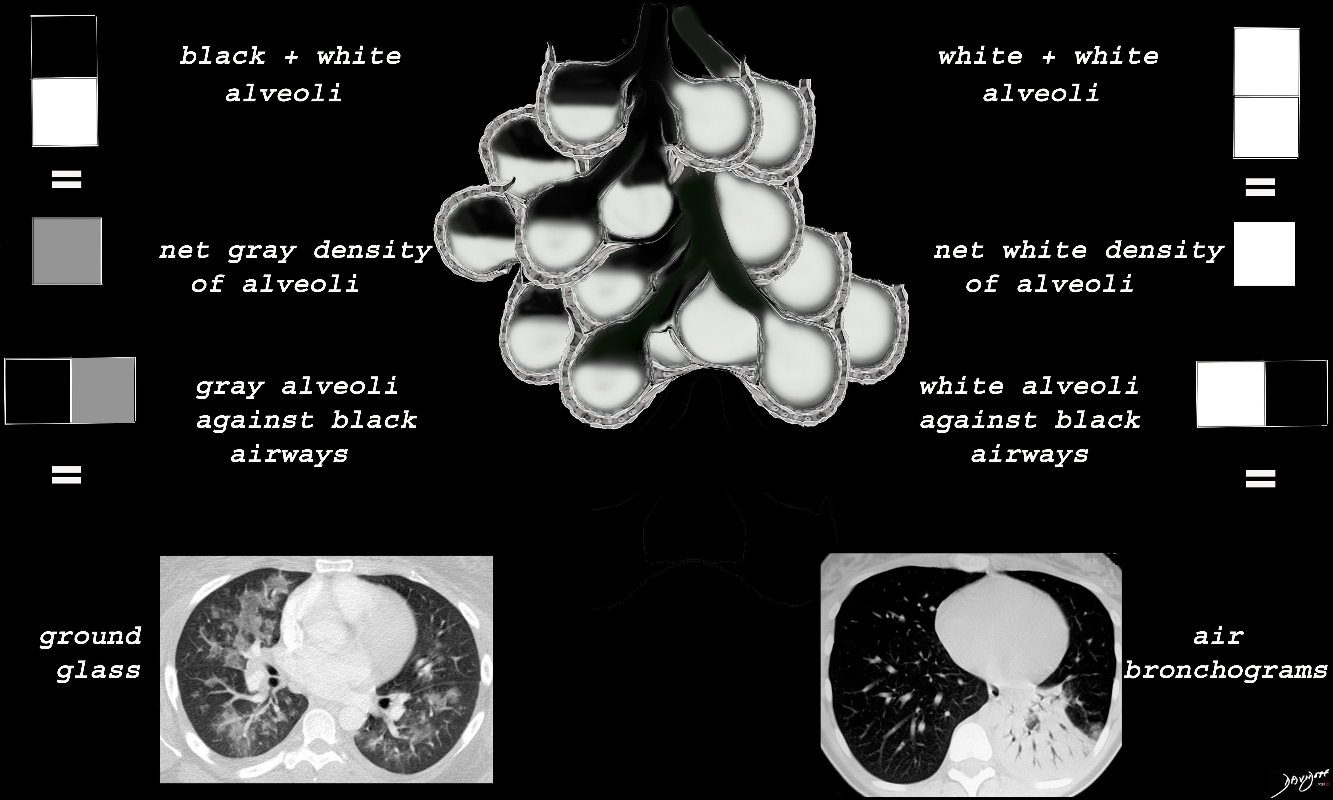
Black White and Gray Densities
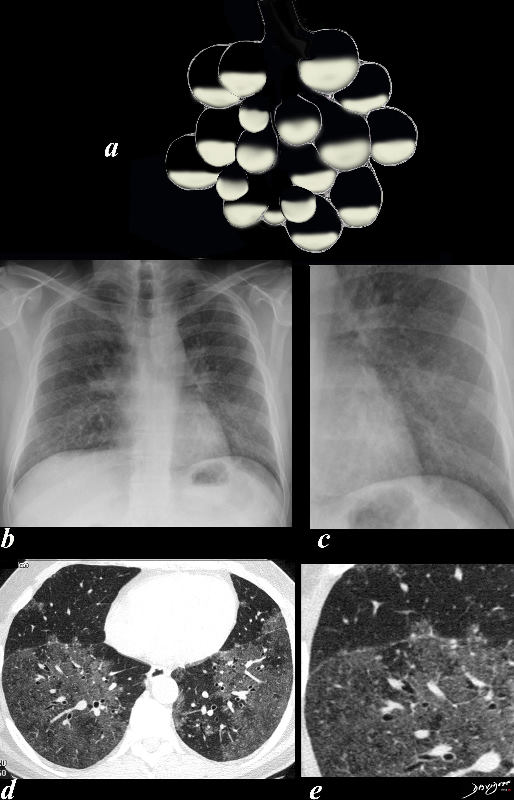
An air filled alveolus appears as black, a fluid filled alveolus appears as white and a a half filled alveolus appears as gray
Ashley Davidoff MD TheCommonvein.net lungs-00688b

When the alveoli are fully filled with fluid, tumor, or pus for example, the overall net density will be white, and when adjacent to air filled airways, air bronchograms are visible (left side of image)
When the alveoli are only partially filled, the density of the fluid added to the density of the air results in an overall gray density, and when positioned next to air filled bronchi, there is insufficient contrast to create an air bronchogram and sufficient to enable visualization of the blood vessels. This is called ground glass opacification
Ashley Davidoff
TheCommonVein.net lungs-00681
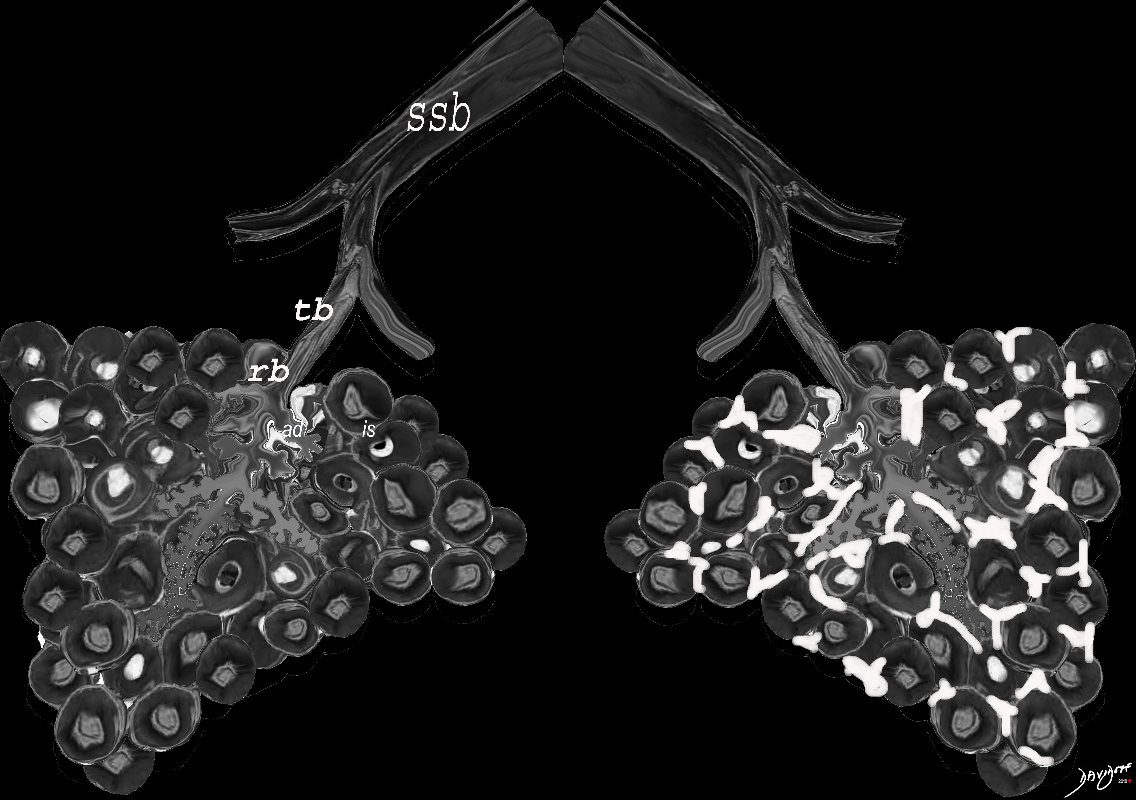
When there are extensive interstitial fibrotic changes in the interstitial compartments of the lung which include the and the interalveolar septa, and the supporting interstitium of the lung between the acini and small airways, the overall net density of the region of involvement will be gray, and when adjacent to the black air filled airways, a ground glass appearance will be apparent
Ashley Davidoff
TheCommonVein.net
ssb = subsegmental bronchiole
tb = terminal bronchiole
rb = respiratory bronchiole
as = alveolar duct
as = alvelar sac
is = anteralveolar septum
Ashley Davidoff
TheCommonVein.net lungs-00682
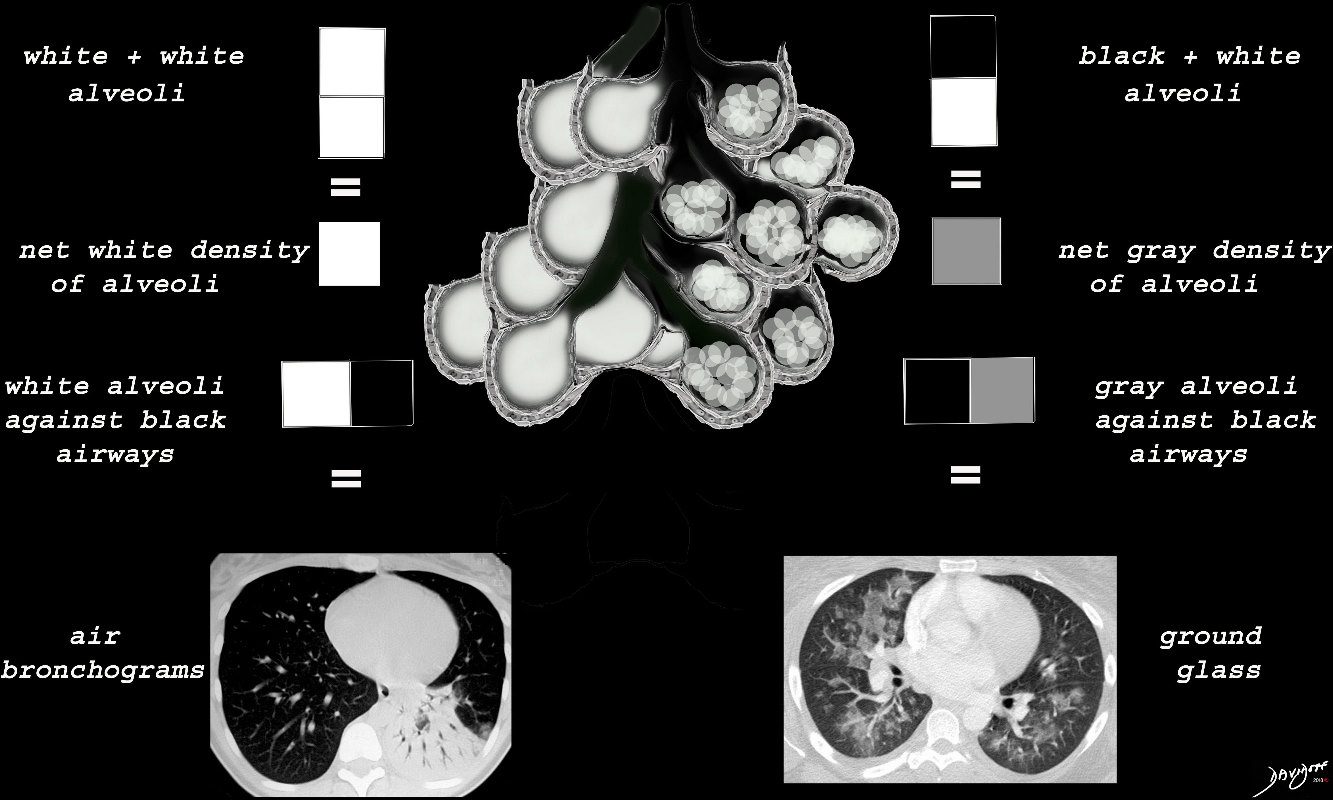
When there are extensive ceelular accumulations in the alveoli, such as adenocarcinoma with lepidic growth, Langerhans cells or other macrophages, the overall net density of the region of involvement will be gray, and when adjacent to the black air filled airways, a ground glass appearance will be apparent
Ashley Davidoff
TheCommonVein.net
ssb = subsegmental bronchiole
tb = terminal bronchiole
rb = respiratory bronchiole
as = alveolar duct
as = alvelar sac
is = anteralveolar septum
lungs-00688
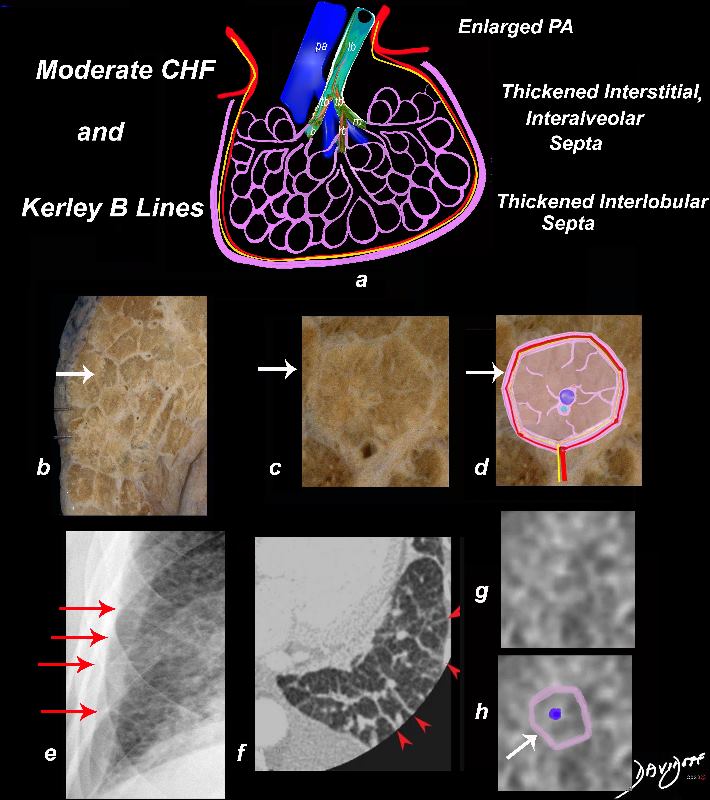
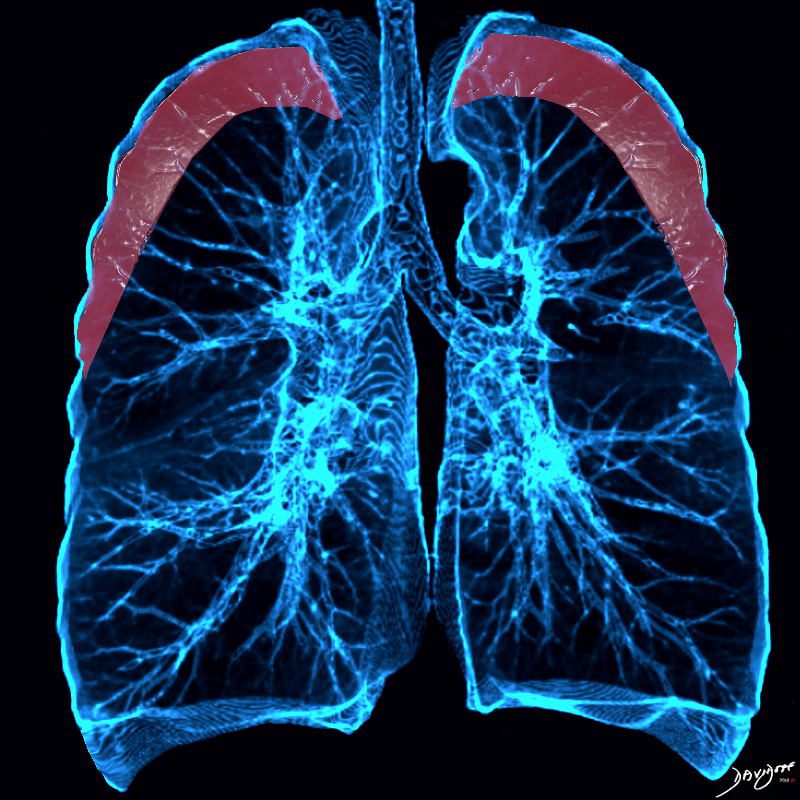
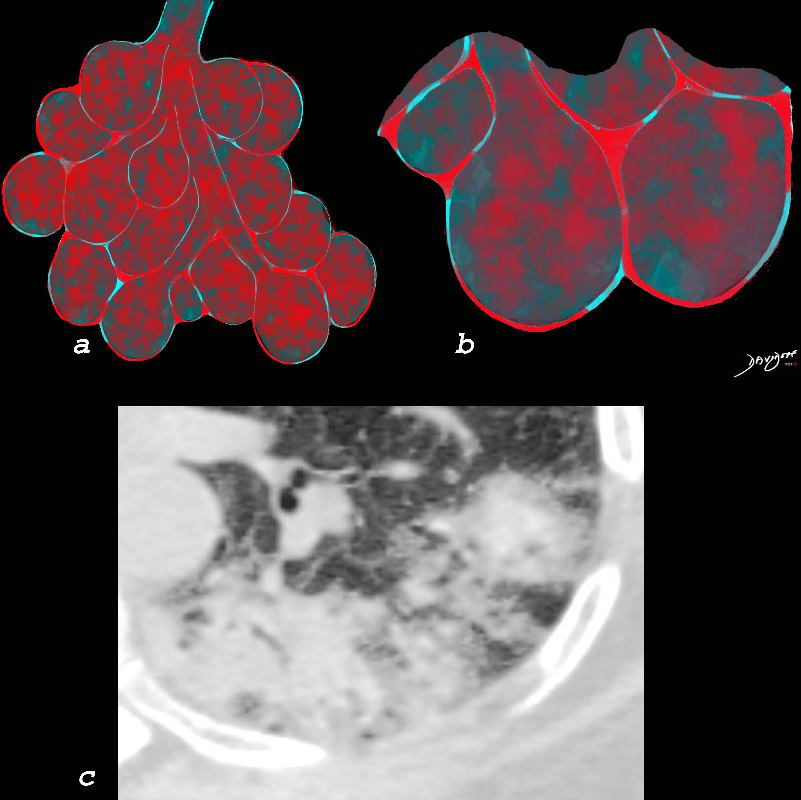
In moderate CHF, when the intravascular pressure is between 30 and 40 mmHg, it exceeds the intravascular oncotic pressure, and fluid starts to leak out of the capillaries into the interstitium. There is distension of the pulmonary arterioles, the lymphatics and thus into the interlobular septa.
The thickening of the interlobular septa (white arrows a,b,c, and d) result in the appearance of Kerley B lines on CXR (red arrows e, and red arrowheads f) . The overall increase in density caused by the fluid accumulations in the inter, and intralobular septa may result in ground glass opacity seen on the CT in images g and h.
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf01b
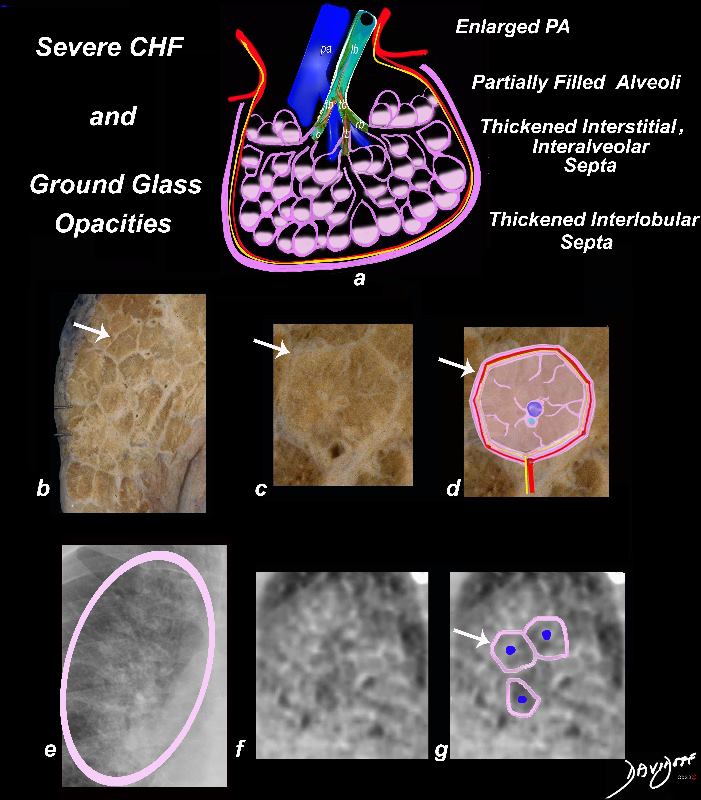
In severe heart failure the end diastolic pressure is between 30 and 40mmHg and fluid continues to leak into the interstitium but now also starts to fill the alveoli. The interalveolar septa and interlobular septa remain thickened (white arrows, b,c,d, and e) and the fluid in the alveoli result in the appearance of ground glass on CXR (circled in pink in e, and noted in the appearance on CT (f,g)) . The pulmonary arteriole remains enlarged ( blue sphere a,d,g).
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf02b
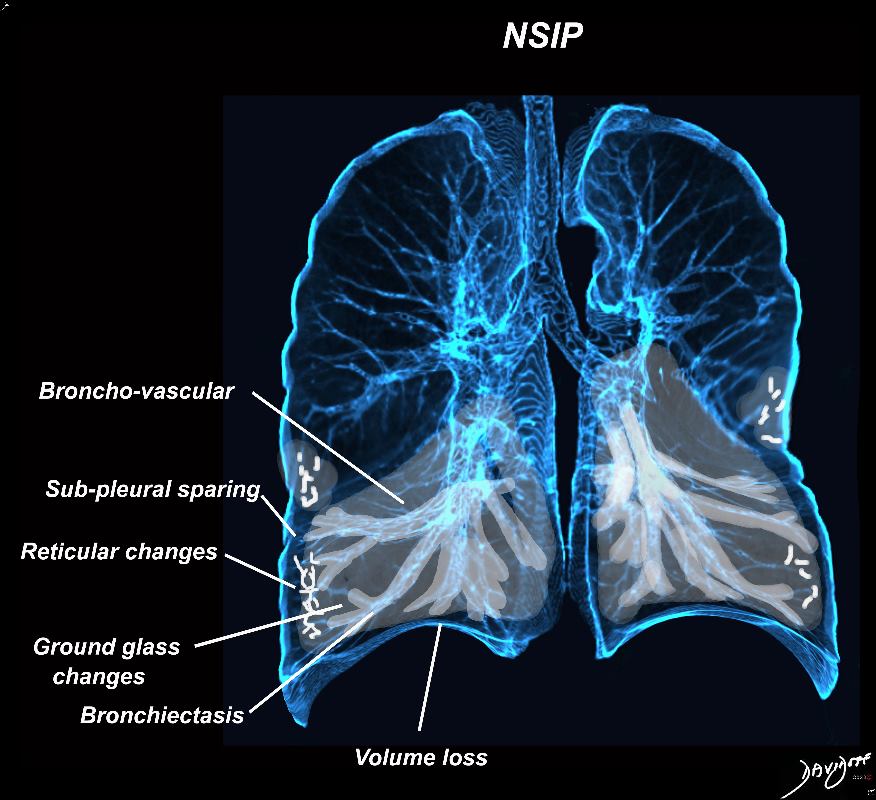
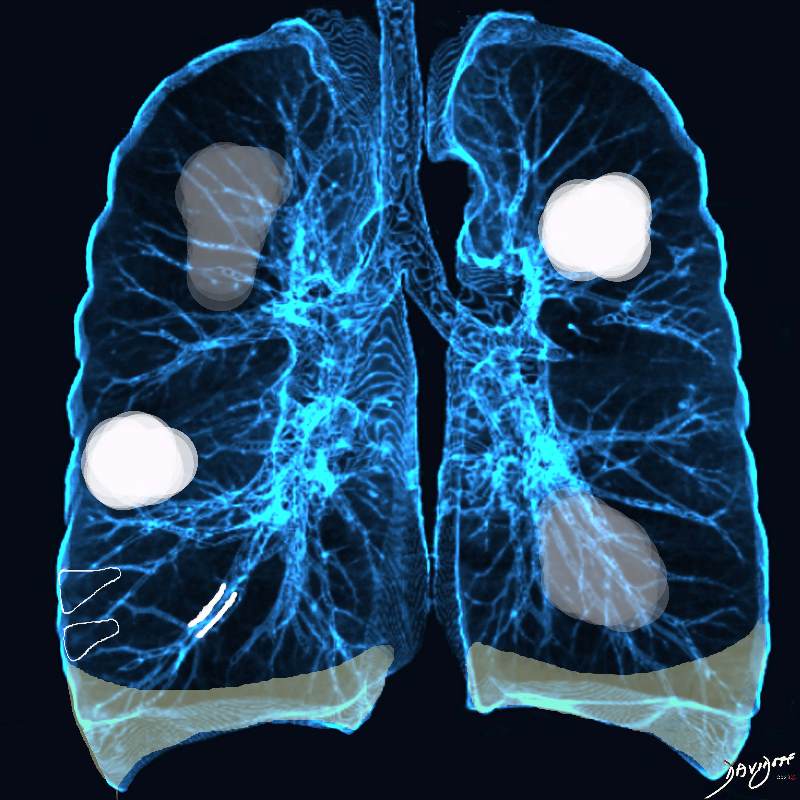
Broncho vascular distribution associated with peripheral sparing, ground glass changes, reticulations, and volume loss, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes
Ashley Davidoff MD TheCommonvein.net lungs-0771b

Broncho vascular distribution associated with peripheral sparing, ground glass changes, reticulations, and volume loss, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes
Ashley Davidoff MD TheCommonvein.net lungs-0771b
Broncho vascular and inter- alveolar interstitial fibrosis dominantly in the lower lobes but affecting the middle and upper lobes to lesser extent resulting in bronchiectasis and reticulations. The overall increase in density results in ground glass changes
Ashley Davidoff MD TheCommonvein.net lungs-0738 NSIP

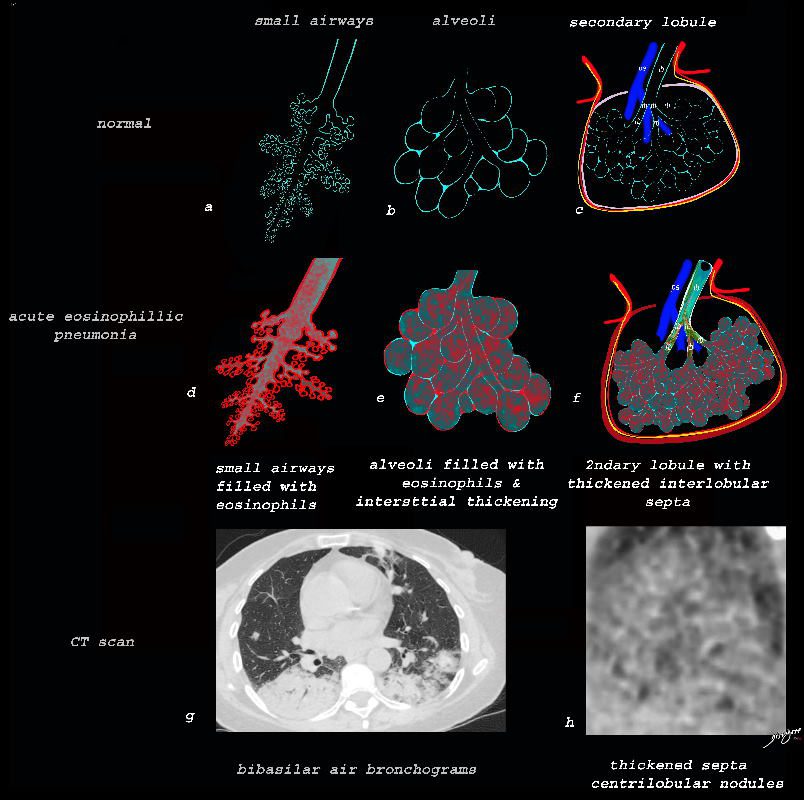
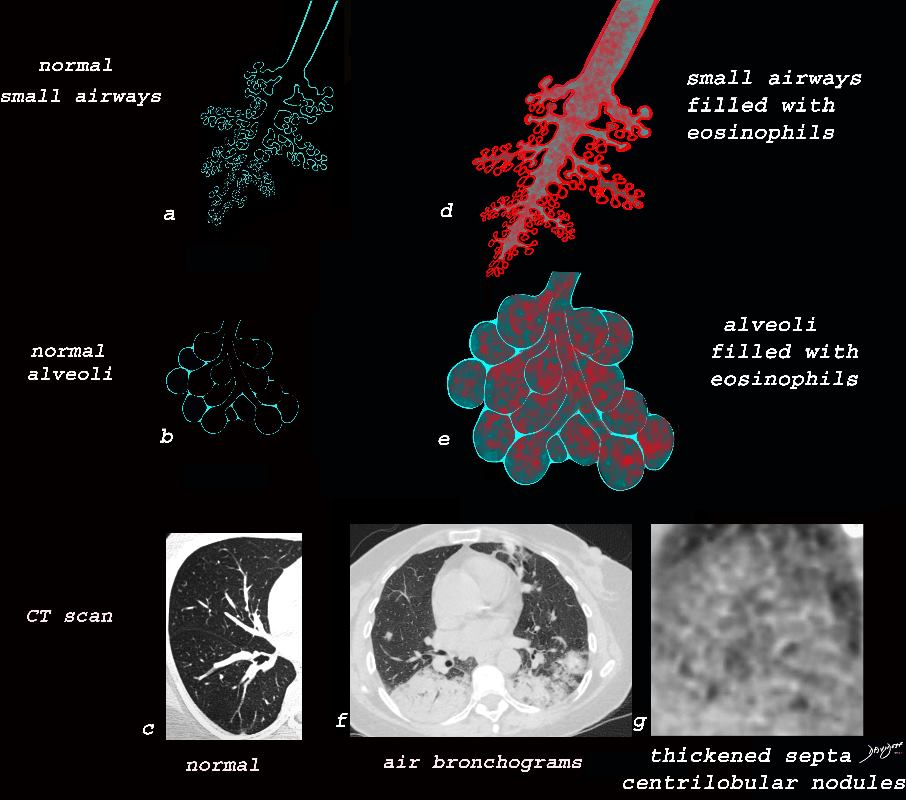
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows bilateral peripheral consolidations in the upper lobes
Ashley Davidoff MD The CommonVein.net lungs-0775e
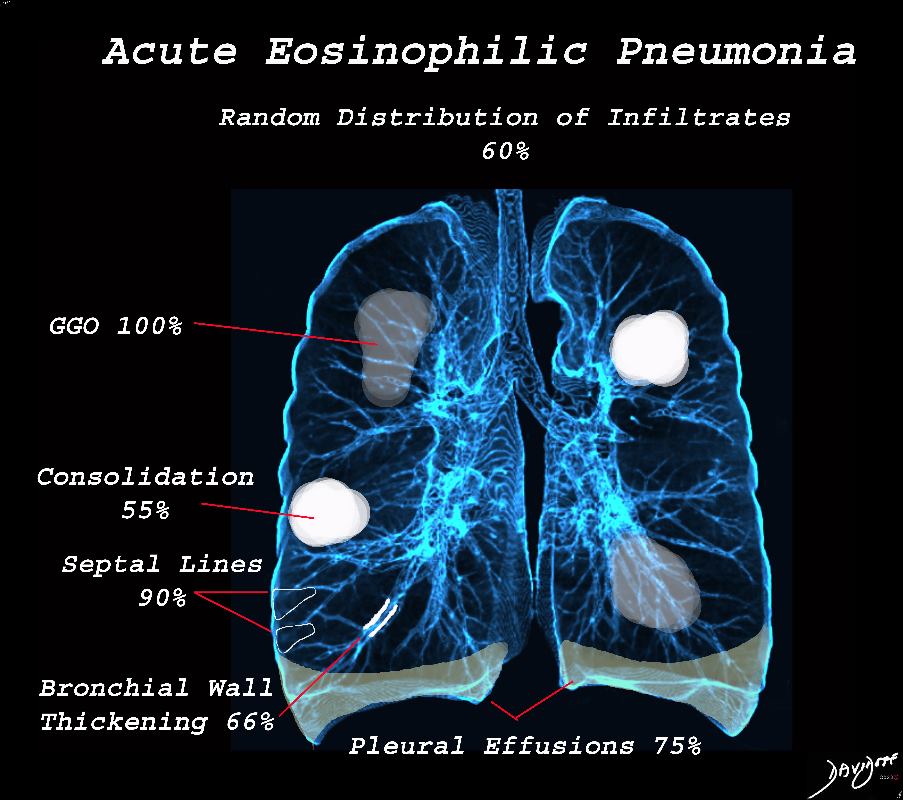
Acute Eosinophilic pneumonia is characterised by ground glass opacities (100%) and sometimes consolidation (55%) most commonly with a random distribution 60%. Septal lines (90%) and thickening of the bronchovascular bundles (66%) and bilateral pleural effusions (75%) were common.
Ashley Davidoff MD TheCommonvein.net lungs-0775-bL (Reference De Giacomi F et al)
Acute Eosinophilic pneumonia is characterised by ground glass opacities (100%) and sometimes consolidation (55%) most commonly with a random distribution 60%. Septal lines (90%) and thickening of the bronchovascular bundles (66%) and bilateral pleural effusions (75%) were common.
Ashley Davidoff MD TheCommonvein.net lungs-0775-b (Reference De Giacomi F et al)
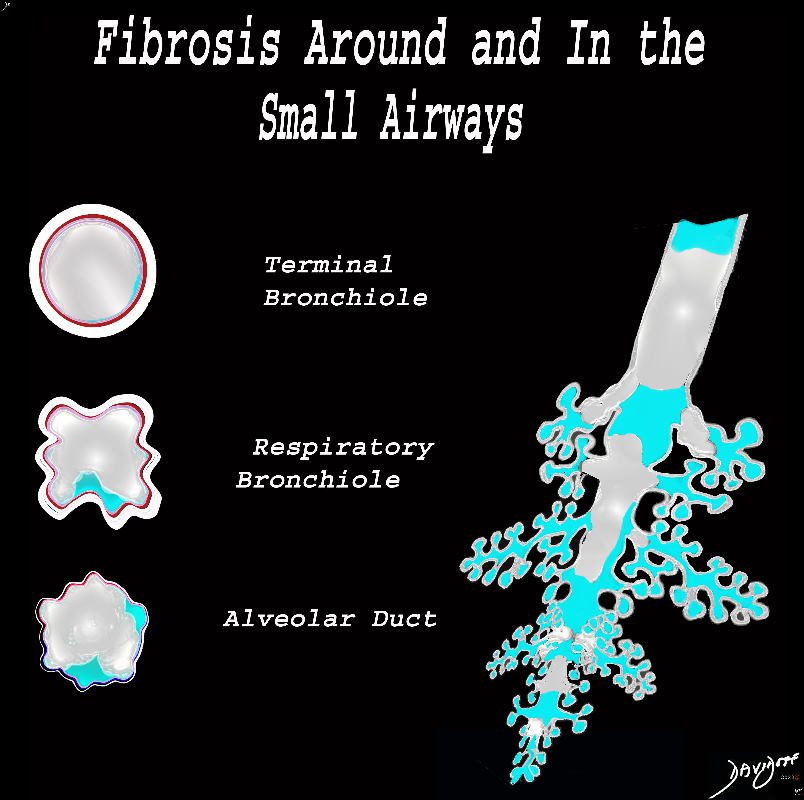
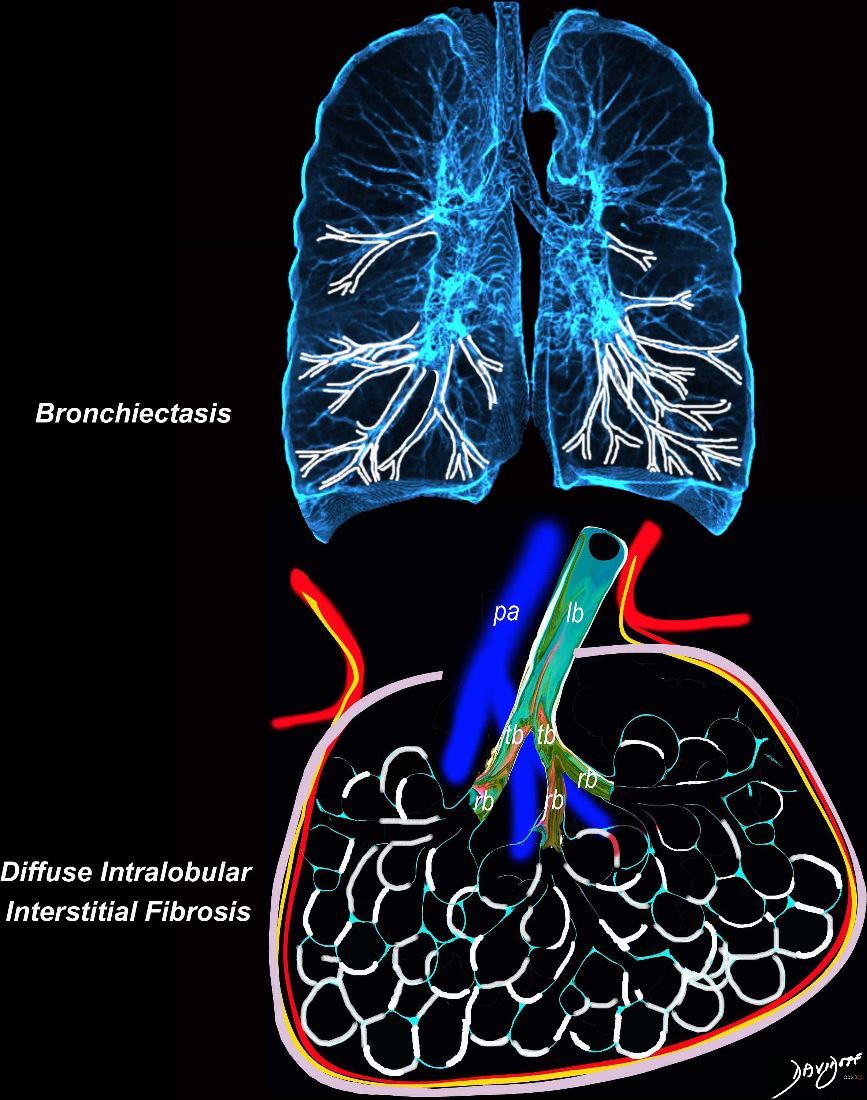
The diagram shows fibrotic changes around and within the small airways including the terminal bronchiole, respiratory bronchiole and the alveolar duct. In this instance the increase density from the fibrotic tissue would result in ground glass changes in the parenchyma and solid centrilobular nodules. Obstruction of the small airways would result in air trapping.
Ashley Davidoff MD TheCommonVein.net lungs-0778
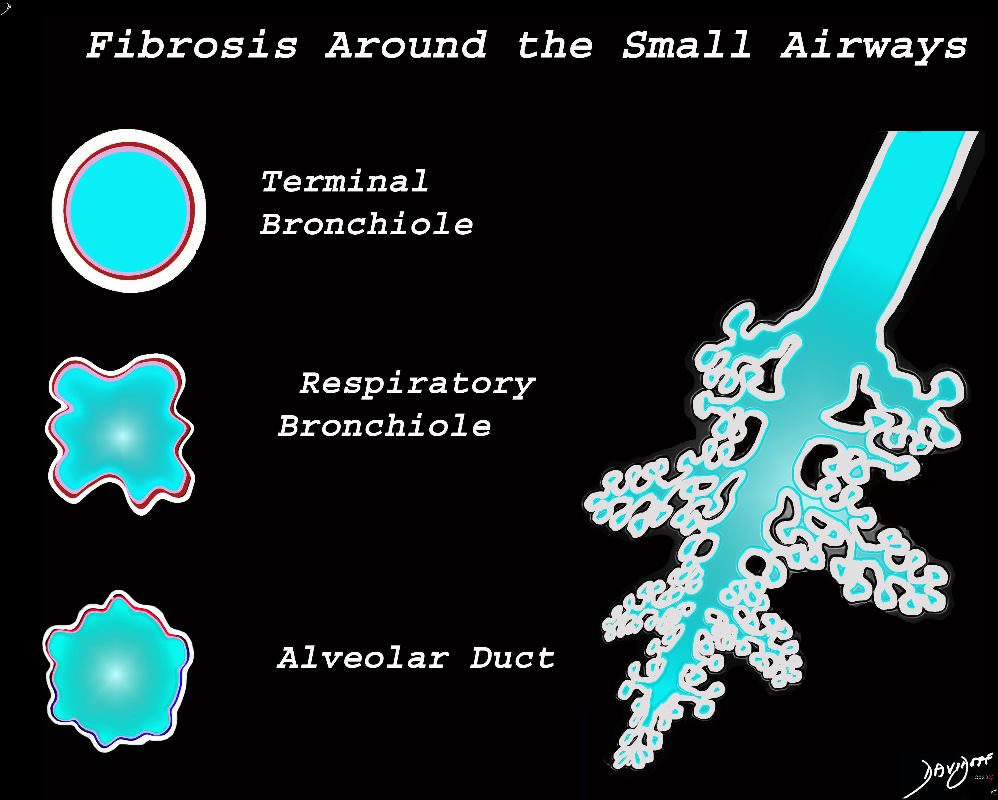
The diagram shows fibrotic changes around the small airways including the terminal bronchiole, respiratory bronchiole and the alveolar duct. In this instance the increase density from the fibrotic tissue would result in ground glass changes in the parenchyma and ground glass centrilobular nodules. Since the airways are patent there would be no air trapping.
Ashley Davidoff MD TheCommonVein.net lungs-0777
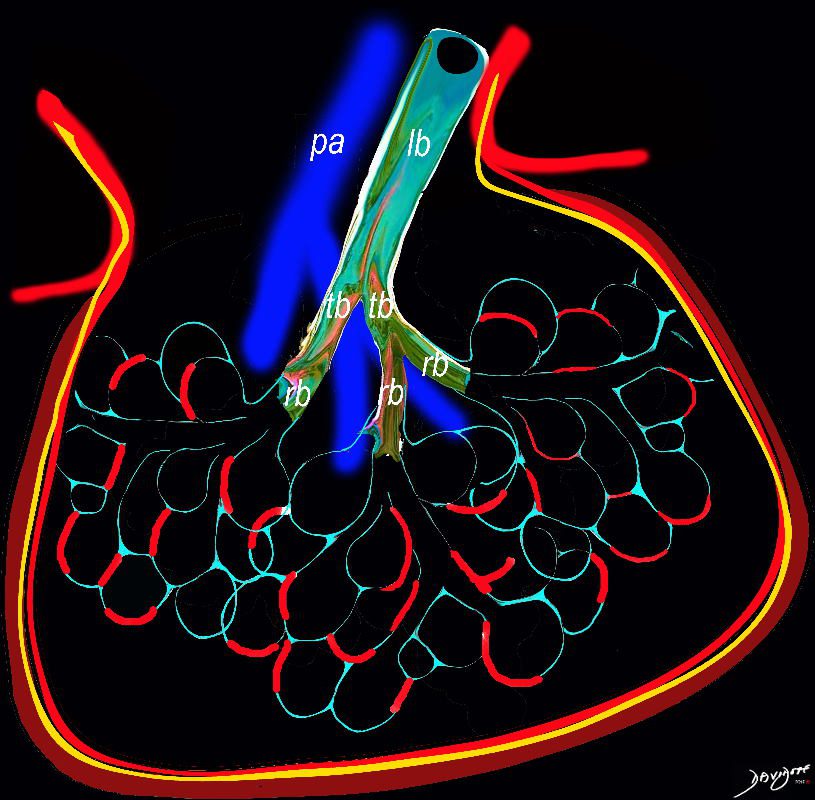
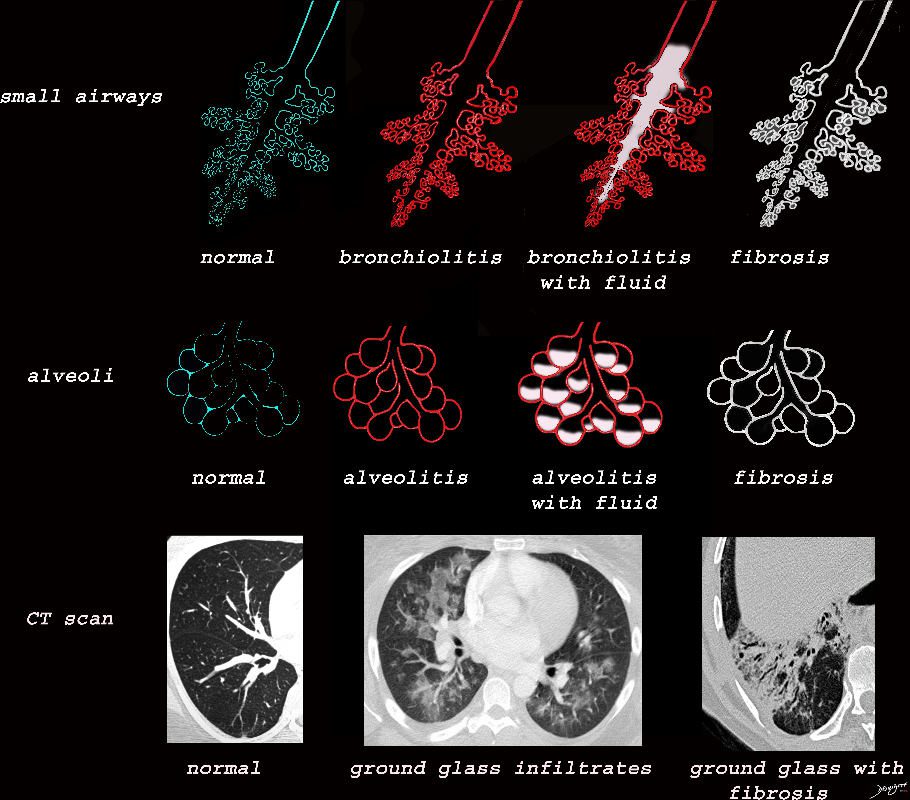
Diagram shows inflammation (red ) in the walls of the alveoli with thickening of the interlobular septa (maroon) . The increased density in the interalveolar septa and interlobular septa results in a ground glass opacity with and crazy paving appearance on CT scan
Ashley Davidoff TheCommonVein.net
lungs-0736a
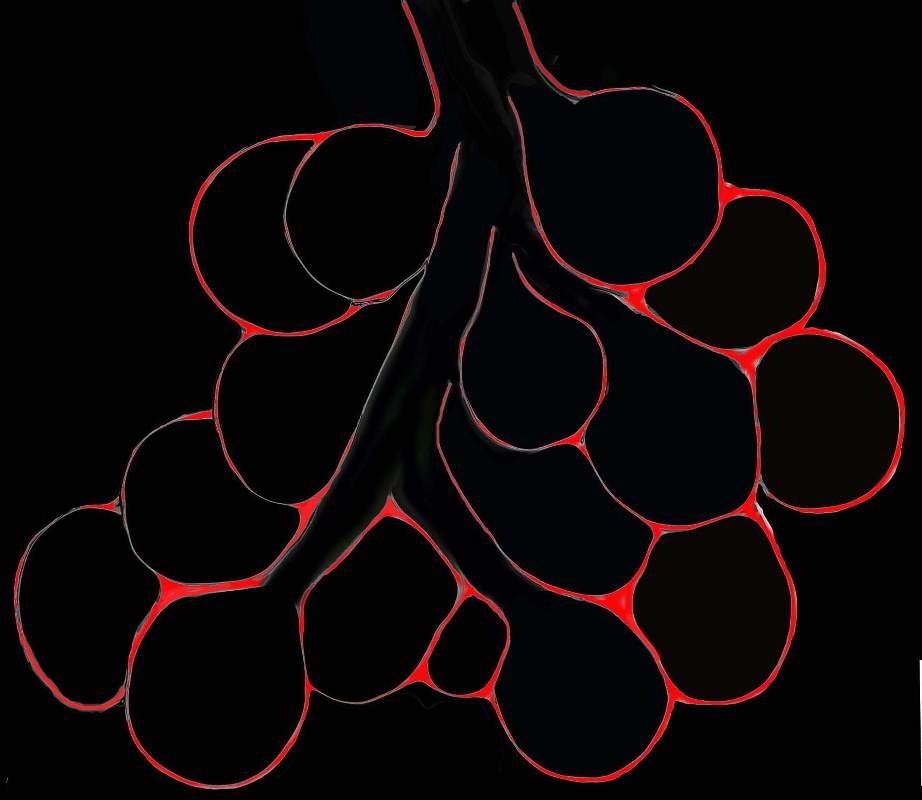
Diagram shows inflammation (red ) in the walls of the alveoli. The increased density in the interalveolar septa results in a ground glass opacity on T scan
Ashley Davidoff TheCommonVein.net
lungs-0736b
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows bilateral peripheral consolidations in the upper lobes
Ashley Davidoff MD The CommonVein.net lungs-0765
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows a peripheral consolidation in the left upper lobe
Ashley Davidoff MD The CommonVein.net lungs-0764
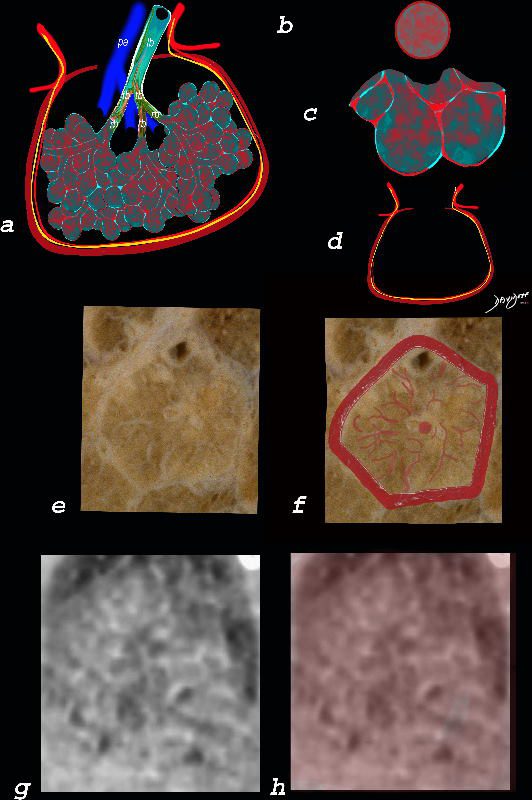
The ground glass changes are a combination of the cellular and exudative inflammatory response in the small airways, alveoli, interalveolar septa and interstitium, and thickened alveolar septum
The diagram shows the abnormal secondary lobule (a) The involved components include the small airways(b) alveoli and interalveolar interstitium (c) and the thickened interlobular septum (d) surrounding the secondary lobule due to an inflammatory process, cellular infiltrate and congestion of the venules and lymphatics in the septum. An anatomic specimen of a secondary lobule from a patient with thickened interlobular septa and interstitial thickening is shown in image e, and is overlaid in red (f) . A magnified view of an axial CT of the lungs in a patient with acute eosinophillic pneumonia shows thickened interlobular septa and centrilobular nodules (g) The inflammatory changes in the aforementioned structures result in an overall increase in density of the lung manifesting as ground glass changes (g) and overlaid in red (h)
Ashley Davidoff MD The CommonVein.net lungs-0762
Ashley Davidoff TheCommonVein.net lungs-0757b
Ashley Davidoff TheCommonVein.net lungs-0757
Ashley Davidoff MD TheCommonVein.net lungs-0733
Ashley Davidoff MD TheCommonVein.net
lungs-0708d- lo res
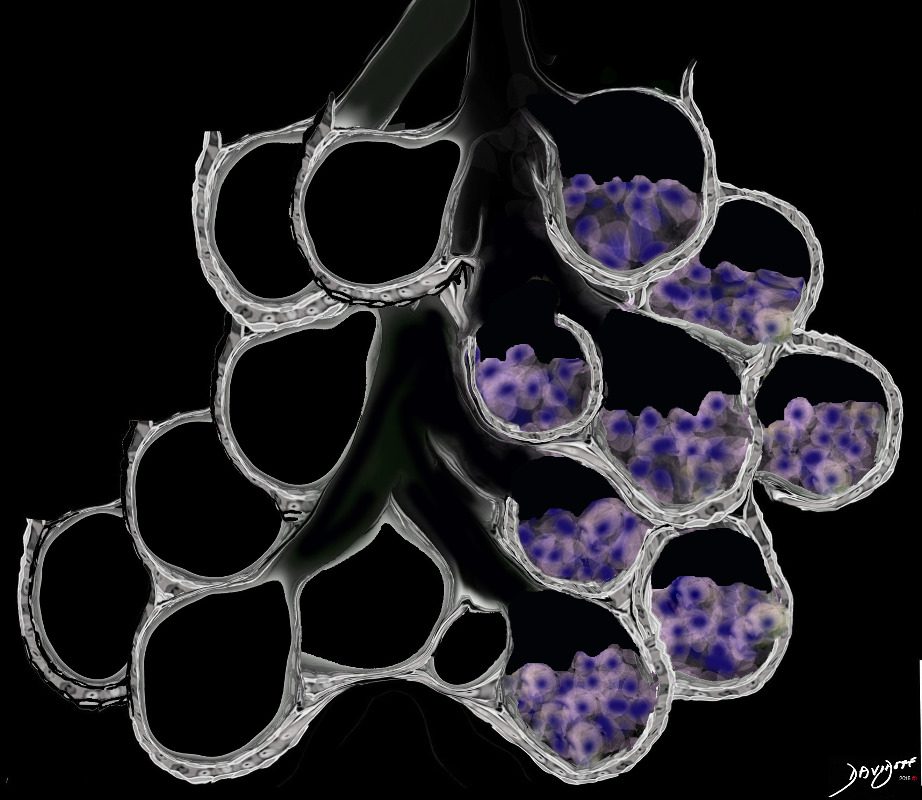
Ground glass opacification may be caused by partial filling of the alveolus with cellular material with partial replacement of air with solid material with the net density being gray rather than white if the alveolus were fully filled. The black of the airway nor the white of the vessels may blend with the gray density and hence they are not visualised in ground glass opacities. The replacement may be due to cellular infiltration including inflammatory ,benign or malignant cells without or with fluid.
Ashley Davidoff MD TheCommonVein.net lungs-0707ad
Ashley Davidoff MD TheCommonVein.net lungs-0702d- lo res
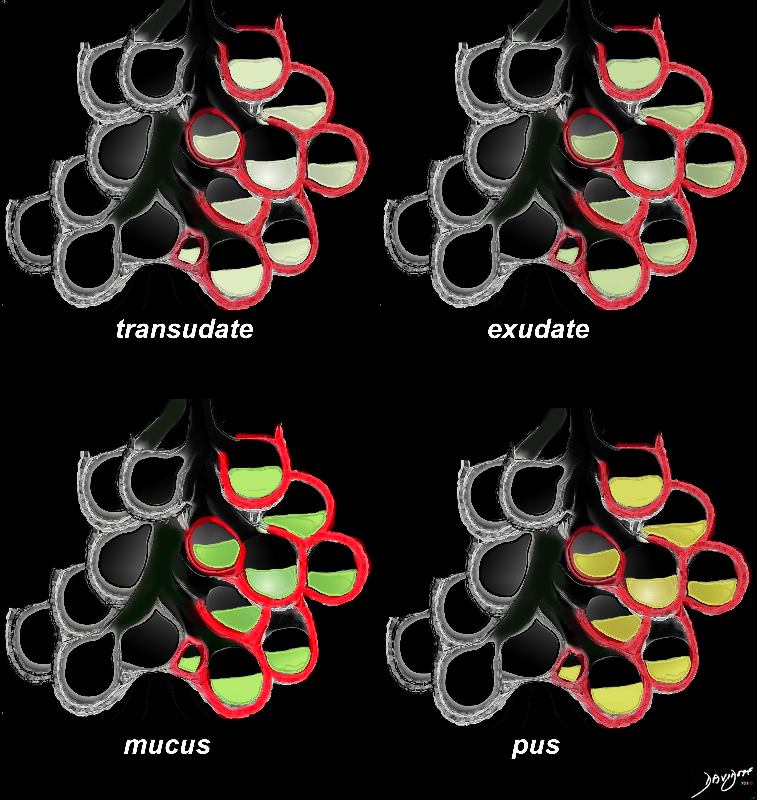
Inflammatory fluids half fill the alveolus and will therefore result in ground Glass Infiltrates
Ashley Davidoff MD TheCommonVein.net
lungs-0703d
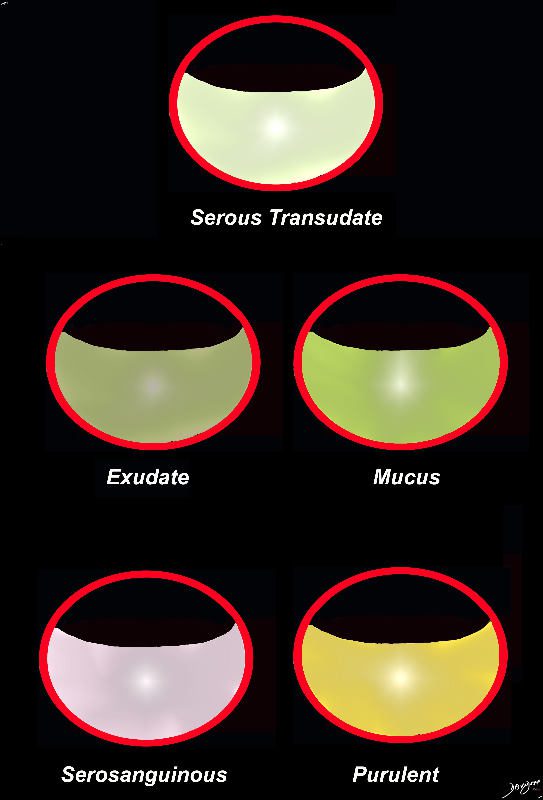
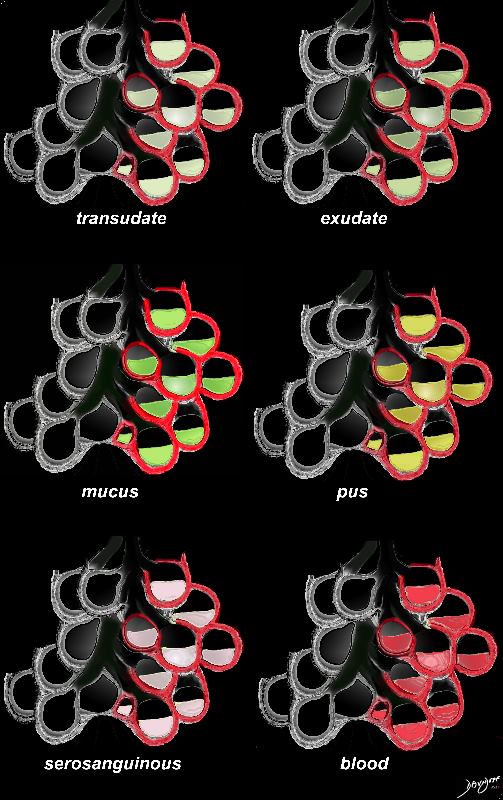
The acute inflammatory process results in fluid exudation into the alveoli which can take the form of a serous transudate, and exudate or in the form of mucus, and when severe (eg ARDS) can result in tissue and vessel destruction and could be be blood tinged. Infected fluid could be mucoid or purulent. The extent of filling the alveoli results either in a ground glass appearance when partially filled or a consolidation when filled.
Ashley DAvidoff MD TheCommonVein.net
lungs-0701d- lo res
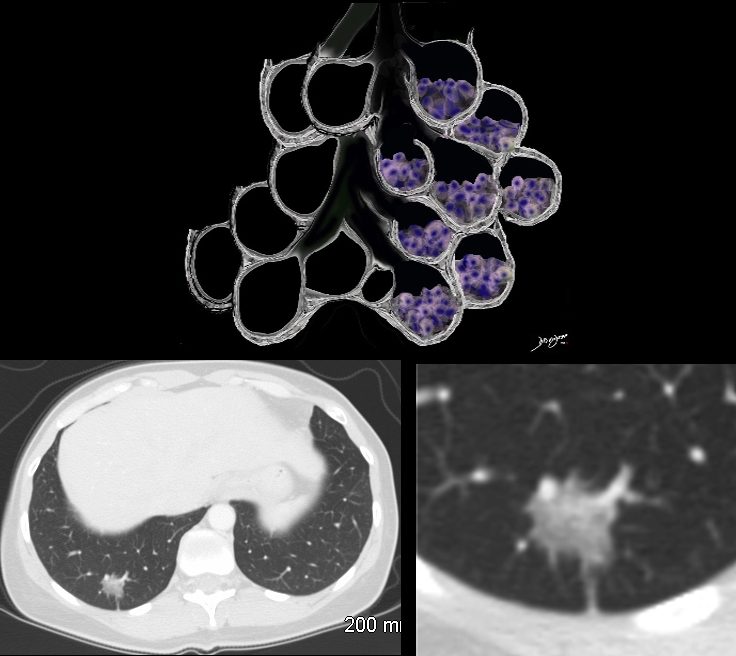
The Ground Glass Opacity (GGO) in this case is caused by partial filling of the alveolus with malignant cells Ground glass opacification may be caused by partial filling of the alveolus with cellular material resulting in partial replacement of air with solid material. The net density is gray rather than white in the situation where the alveolus is fully replaced with cells or fluid. There is blending of the black of the subtending airways and the white of the vessels with the gray density of the cellular infiltrate and hence the normal vessels are not visualized in ground glass opacities.
Ashley Davidoff MD TheCommonVein.net 134375b01
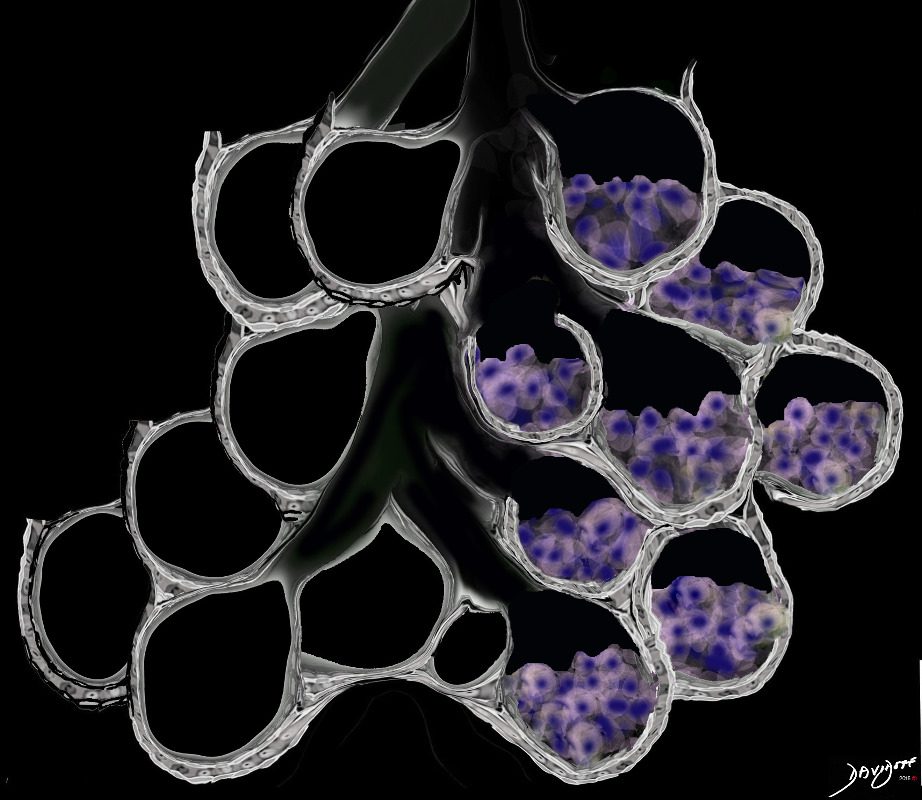
Ground Glass Opacity (GGO) Caused by Cellular Accumulation with Partial Filling of the Alveolus Ground glass opacification may be caused by partial filling of the alveolus with cellular material with partial replacement of air with solid material with the net density being gray rather than white if the alveolus were fully filled. The black of the airway nor the white of the vessels may blend with the gray density and hence they are not visualized in ground glass opacities.
Ashley Davidoff MD TheCommonVein.net lungs-0707a