
CHF

50 year old female with diabetes, chronic renal failure with congestive heart failure. CT in the coronal plane shows diffuse ground glass changes, Kerley B lines at the right base,
Ashley Davidoff MD TheCommonvein.net 50-003-CT

Ashley Davidoff MD TheCommonvein.net 50-004-CT

Ashley Davidoff MD TheCommonvein.net 50-010-CT

Ashley Davidoff MD TheCommonvein.net 50-007-CT
Amyloidosis
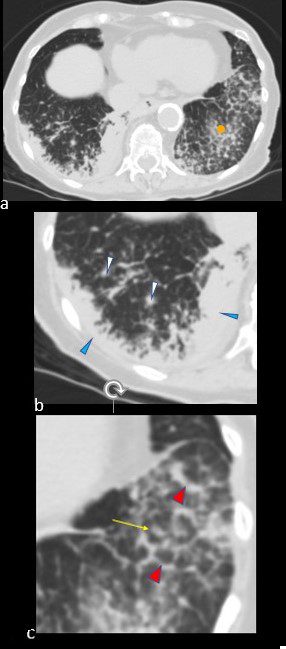
CT scan in the axial projection at the base of the lungs show many features of amyloidosis including lung nodules (white arrowheads) and infiltrates (b), and diffuse deposition within the alveolar septa (red arrowheads, c) and centrilobular nodules(yellow arrow c)
Ashley Davidoff MD Boston Medical Center
TheCommonVein.net septal-amyloidosis-001b
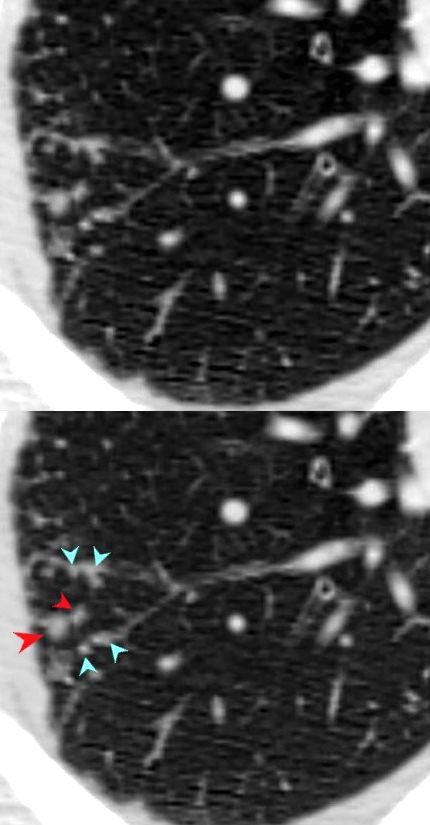
Nodular Thickening Along the Vein – Miliary TB

68 year old female presented with malaise night sweats weight loss Quantiferon gold positive, with a past history of treated TB in her native country as a child. Axial CT images through the upper lobe shows a miliary pattern of disease affecting interlobular septa, centrilobular and tree in bud nodular patterns. Bronchoscopy isolated Mycobacterium complex. She was treated with good result
Ashley Davidoff MD TheCommonVein.net mycobacterium-complex-TB-68-001

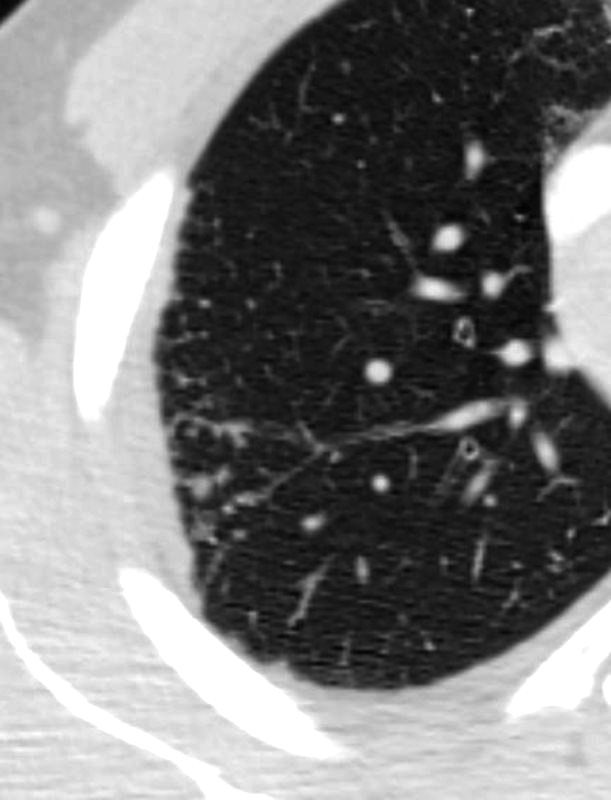
68 year old female presented with malaise night sweats weight loss QuantiFeron gold positive, with a past history of treated TB in her native country as a child. Axial CT images through the upper lobe shows a miliary pattern of disease affecting interlobular septa, centrilobular and tree in bud nodular patterns. Bronchoscopy isolated Mycobacterium complex. She was treated with good result
Ashley Davidoff MD TheCommonVein.net mycobacterium-complex-TB-68-008
Sarcoidosis
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
48-year-old previously well presented with dyspnea and initial CXR showed an infiltrate at the right base, and clinically resolved. He presented a year later with right chest pain and low grade ever and the CXR showed patchy opacities in the LUL and in the RLL
A subsequent CT showed LUL nodular opacities and subpleural rim of consolidation in the LUL and more prominently at both lung bases, associated with significant mediastinal adenopathy. Lymphovascular nodularity was noted in the bronchovascular bundles as well as in the interlobular septa, consistent with sarcoidosis
CXR and CT 4 years later showed almost complete resolution of the parenchymal findings and the CT findings except for minimal reticulation and scarring in the subpleural regions
Ashley Davidoff MD
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
48-year-old previously well presented with dyspnea and initial CXR showed an infiltrate at the right base, and clinically resolved. He presented a year later with right chest pain and low grade ever and the CXR showed patchy opacities in the LUL and in the RLL
A subsequent CT showed LUL nodular opacities and subpleural rim of consolidation in the LUL and more prominently at both lung bases, associated with significant mediastinal adenopathy. Lymphovascular nodularity was noted in the bronchovascular bundles as well as in the interlobular septa, consistent with sarcoidosis
CXR and CT 4 years later showed almost complete resolution of the parenchymal findings and the CT findings except for minimal reticulation and scarring in the subpleural regions
Ashley Davidoff MD