
Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
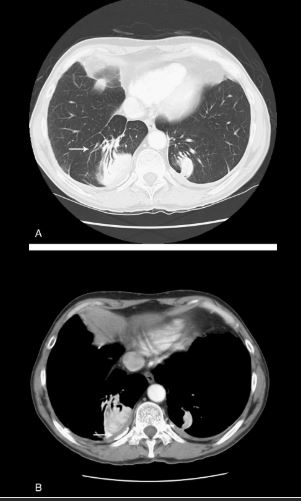
Identified as a curvilinear opacity arising from a rounded, subpleural opacity on CT (Fig. 4A, arrow), the “comet tail” denotes the distorted curving of pulmonary vessels and bronchi toward a region of round atelectasis.14–17 The atelectatic lung typically abuts an area of pleural effusion or thickening, and there are associated signs of volume loss. Round atelectasis is an unusual form of atelectasis most commonly associated with asbestos-related pleural disease (Fig. 4B, arrow), but also seen with other chronic forms of pleural disease, such as tuberculosis, histoplasmosis, pulmonary infarcts, or congestive heart failure.14–17 It is also known as atelectatic pseudotumor, folded lung, or Blesovsky syndrome, after the physician who initially postulated an association with asbestos exposure.18 Most often found in the posterior aspect of the lower lobes, it may demonstrate significant contrast enhancement and contain air bronchograms.14–17 Histopathology demonstrates fibrous thickening of the visceral pleura with extensive pleural folding and invagination.19 The exact cause is still debated. One theory suggests that a pleural effusion is the inciting event causing passive atelectasis and pleural invagination.20 Fibrous adhesions will eventually develop between the visceral and parietal pleural surfaces, so that when the effusion clears, the entrapped lung folds in on itself. An alternate theory suggests that a focal inflammatory pleural fibrotic response secondary to irritants such as asbestos, is solely responsible for causing invagination of the pleura and regional atelectasis of the subjacent lung.14,19,21