
Left Lung Parts: Basic Anatomy
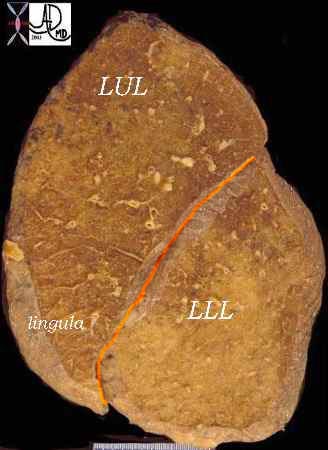
The left and right lungs are very different. We have already noted that the mainstem bronchi are different, with the left mainstem bronchus being long and thin, while the right mainstem bronchus is short and fat. The left lung has only two lobes. There is a left upper lobe (LUL) and a left lower lobe (LLL). The left lung does not have a middle lobe. Instead, the middle lobe equivalent is the lingula, which is in fact part of the LUL and not a separate lobe.
The two lobes of the left lung are separated by the major or oblique fissure, which is the only fissure on the left side. The left lung is smaller than the right and has 8 segments compared to the 10 segments on the right.
The upper lobe of the left lung has superior and lingula divisions. Both of these divisions have two segments each. The segments of the superior division are the apical-posterior and the anterior segments. The lingula is divided into superior and inferior segments. As noted there is no fissure between the upper segments of the LUL and the lingula – they are both part of the LUL. The division of the lower lobe closely resembles that of the right except that there is consolidation of two of the left lower lobe segments. Thus while the RLL has 5 segments the LLL has only four. Again, as is characteristic, the left lung consolidates its component parts.
The superior segment of the LLL forms the top of the pyramid of the LLL. Inferiorly and at the base of this pyramid, the anterior and medial segments combine to form the anteromedial basal segment, followed by the lateral basal, and posterior basal segments.

This is a drawing is of a left lung in coronal section. Note there are only two lobes separated by the major fissure
Courtesy Ashley Davidoff MD The CommonVein.net 32686b05L01
Left Lung Parts: Applied
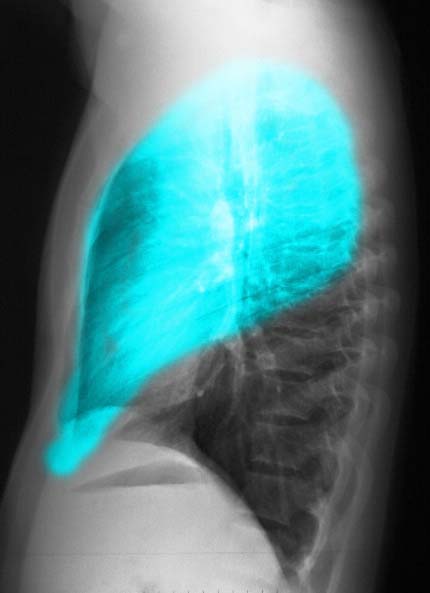
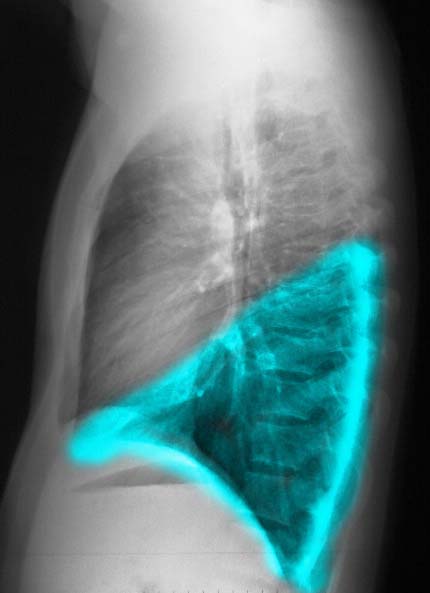
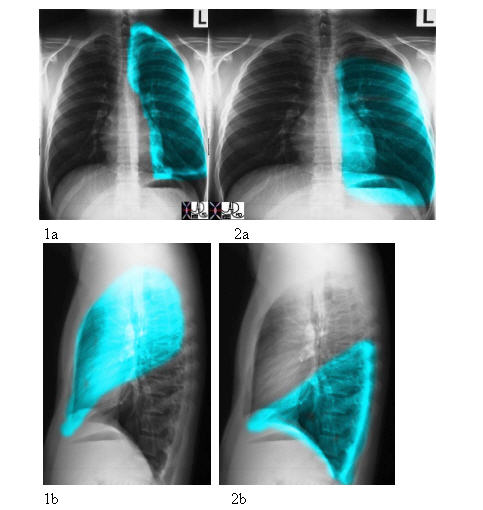
The overall volume of the left lung is smaller than the right, but the distribution of volume between LUL and LLL is more equalized and balanced. Again in the P-A projection the two lobes overlap each other. A nodule in the upper lung field or lower lung field as seen on the P-A projection can be located either in the upper or lower lobe. The lateral examination is essential to accurately locate the disease. The LUL is anterior and above the fissure (see Fig 1b), while the LLL is posterior and below the fissure (see Fig 2b).
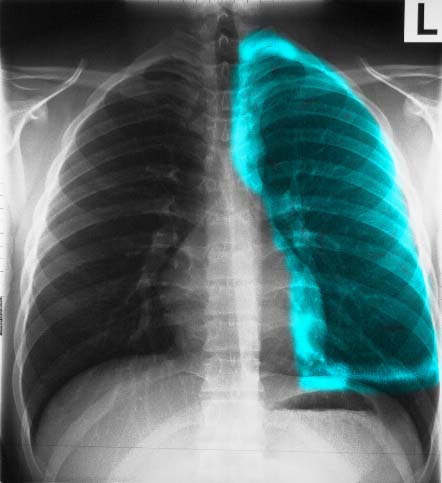
The A-P examination of the chest shows the LUL, with the teal overlay representing the upper lobe and lingula.. Note how the lingula hugs the left heart border. Ashley Davidoff MD TheCommonVein.net 30397b05
Ashley Davidoff MD

The A-P examination of the chest shows the LLL, with the teal overlay. Note the similarity in size and shape of the LUL and LLL . Ashley Davidoff MD TheCommonVein.net
Ashley Davidoff MD TheCommonVein.net 30398b06
Ashley Davidoff MD TheCommonVein.net
Courtesy of: Ashley Davidoff, M.D.
Courtesy Ashley Davidoff MD The CommonVein.net 30399
Ashley Davidoff MD TheCommonVein.net
Ashley Davidoff MD TheCommonVein.net 32228b03

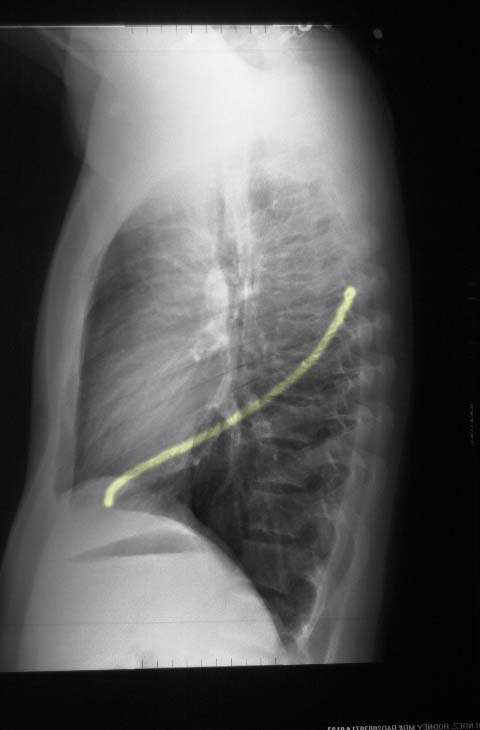
This coronal reformats through the tracheobronchial tree show the major fissures bilaterally. They are usually quite difficult to see and unless you know where to look you may miss them altogether. Usually there is a hint of hypovascularity along the fissure resulting in a relative lucency as can be appreciated in this examination. The fissures have been overlaid in orange in the next image. As the coronal cut proceeds posteriorly the lower lobe becomes more prominent and the upper lobes less so. If you review the lateral chest x-ray and project the cuts you would get a better sense of this concept of the dominance of the RLL and its posterior location .
Ashley Davidoff MD. TheCommonVein.net 32682b
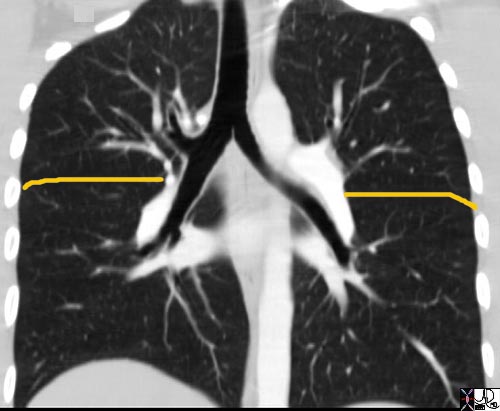
This coronal reformats through the tracheobronchial tree show the major fissures bilaterally. They are usually quite difficult to see and unless you know where to look you may miss them altogether. Usually there is a hint of hypovascularity along the fissure resulting in a relative lucency as can be appreciated in this examination. The fissures have been overlaid in orange. As the coronal cut proceeds posteriorly the lower lobe becomes more prominent and the upper lobes less so. If you review the lateral chest x-ray and project the cuts you would get a better sense of this concept of the dominance of the RLL and its posterior location .
Ashley Davidoff MD. TheCommonVein.net 32682b01.jpg
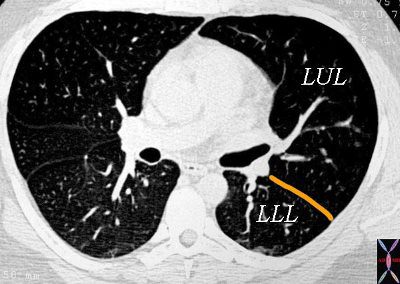
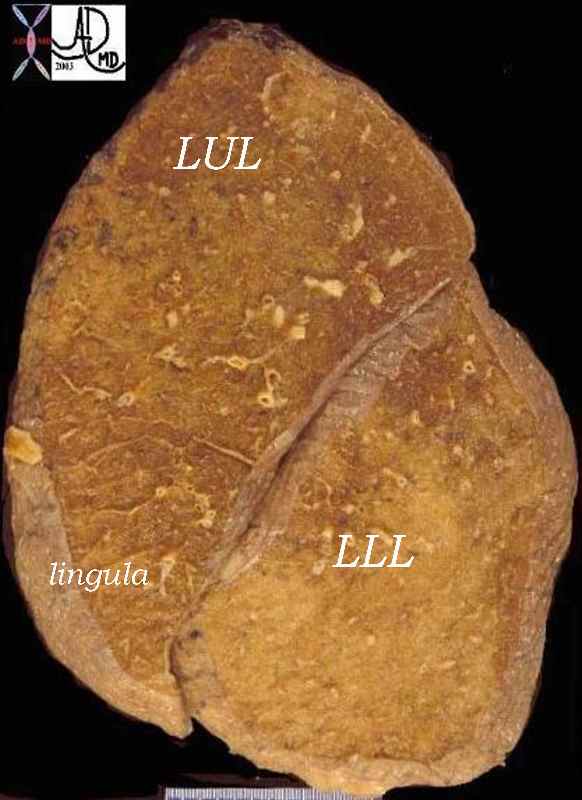
This axial CT shows the major fissure (orange) of the left lobe on the CT scan separating the LUL from the LLL The anatomic specimen in the following image is in the sagittal plane. On the right side the posteriorly placed oblique (major) fissure and the anteriorly placed transverse fissure (minor) can be seen.
Courtesy Ashley Davidoff MD The CommonVein.net 32160b0
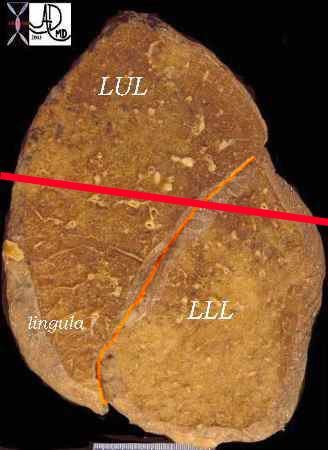
The anatomic specimen is in the sagittal plane with the posterior aspect to the left. The red line reflects the axial plane of the CT above.
Courtesy Ashley Davidoff MD The CommonVein.net 32228b04
When we read plain films of the chest we use the position and relations of the lungs to the heart and the fissures to locate disease processes, including infiltrates, nodules, and regions of atelectasis. We use two principles to locate disease. The first is the described relations of structures to each other, and the second is the concept of “silhouetting.” The important facts that pertain are that the RML abuts the right heart border, the lingula the left heart border, and the lower lobes on both sides abut the diaphragm. The principle of “silhouetting” is commonly used to define the nature and location of a soft tissue process in the lung. We have described the fact that we are able to see and distinguish two different structures because their densities are different. Thus we are able to see the heart border or the diaphragm, for example, because they abut air- filled lung tissue which has a completely different density to their soft tissue nature. If, however, the ai- filled lung is replaced by pus or exudates (pneumonia) or become airless (atelectasis), then the abutting structures both have soft tissue density and cannot be distinguished from one another. If there is a process that silhouettes the right heart border in the P-A projection then we know that this process is in the RML. Similarly, if the left heart border cannot be distinguished from the disease process, we know that it is in the lingula.
It is important to identify accurately the location of disease, particularly nodules and masses which may have to be surgically removed, since the surgeon has to know which part of the lung has to be removed.