
Introduction
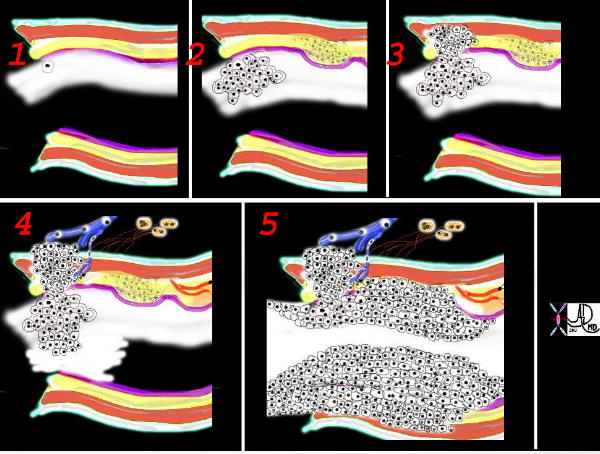
This is a collage showing the evolution of a malignant cell (1) into a nodule restricted to the epithelium (2) which with time penetrates the basement membrane and progressively extends into the submucosa and muscularis (3). Subsequent extension into local lymph nodes and blood vessels occurs (4) as well as growth into the lumen. As it grows circumferentially, narrowing and eventually obstruction of the lumen complicates the process (5) Space in tubular systems is limited and malignant growth has no respect for this space nor for boundaries. By definition malignant disease is space occupying.
Ashley Davidoff
TheCommonVein.net
32336c
Complications of Lung Cancer in General
The result of neoplastic disease is space occupying disease. Depending on the location – different structural and functional effects and hence complications will result. Local obstruction of the airways will expectedly result in localized atelectasis Involvement of the pleura will be complicated by pleural effusion and if the pericardium is involved – pericardial effusion. If these accumulate rapidly or sizably they may respectively affect the function of the lung and heart. Acute tamponade can be life threatening.
Invasion into the lymphatics can result in lymhangitis obliterans sometimes with significant respiratory compromise and marked dyspnea. Obstruction of the SVC may result in the SVC syndrome sometimes with dramatic face swelling and discoloration.
Local Effects
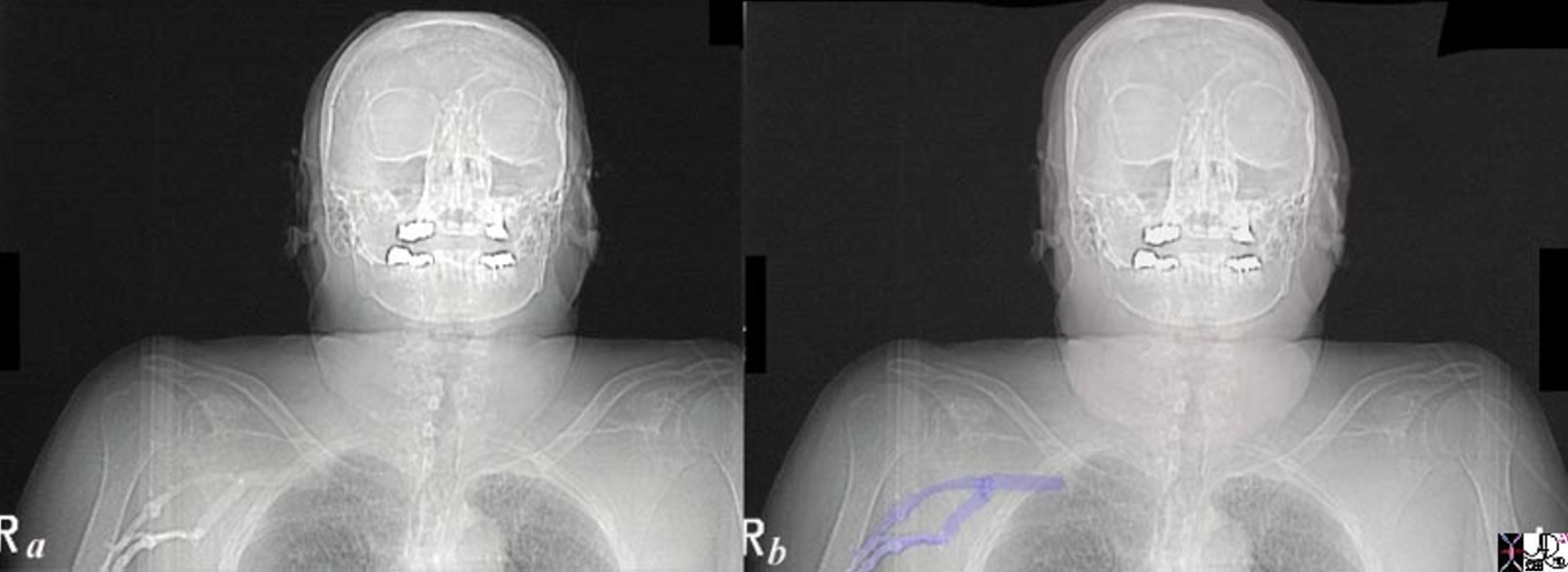
76 year old female with central lung cancer and SVC syndrome as noted by this scout film following contrast injection where contrast is trapped in the right subclavian system because of the obstruction of inflow. Note also the significant swelling of the face and neck which was new for this patient.
Courtesy Ashley Davidoff MD
TheCommonVein.net
24705c01.8s
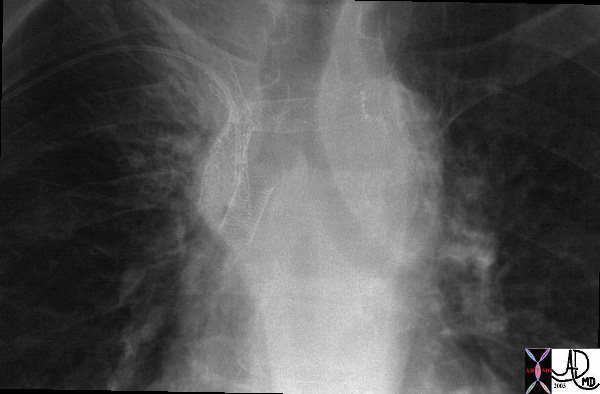
This is a case of a central squamous carcinoma causing obstruction of the right mainstem bronchus and SVC requiring stents in both. This image tells the story of how tubular transport function is compromised by reduced size, and how size can be restored by modern technology.
Courtesy Ashley Davidoff MD
TheCommonVein.net
0916030018
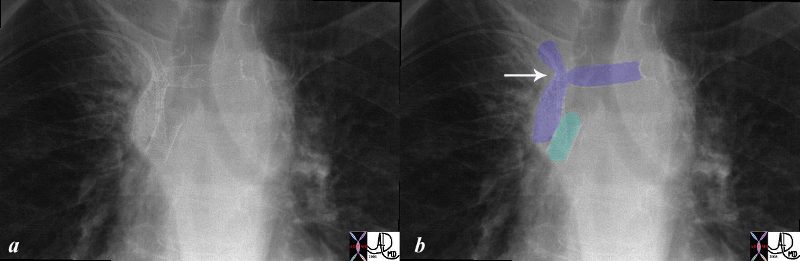
This is a case of a central squamous carcinoma causing obstruction of the right mainstem bronchus and SVC requiring stents in both. This image tells the story of how tubular transport function is compromised by reduced size, and how size can be restored by modern technology.
Courtesy Ashley Davidoff MD
TheCommonVein.net
32147c03.8s
Ashley Davidoff MD
TheCommonVein.net
32269b see 680249
keywords
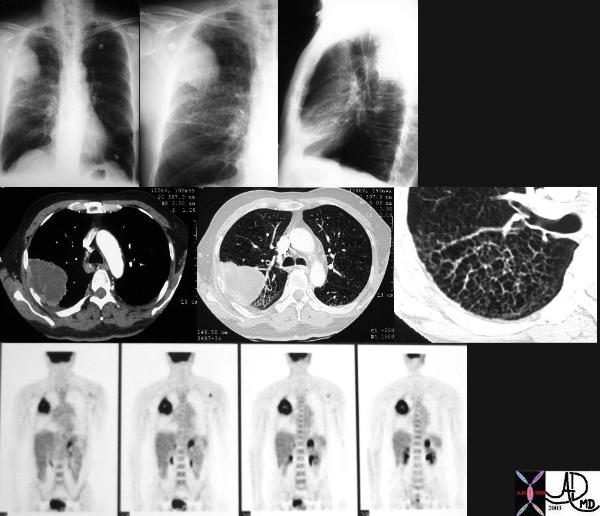
lungs pulmonary mass RUL neoplasm malignant primary lymphatics lymphangitis imaging plain film CXR CTscan PETscan

This paramidline sagittal section of the left lung (leftward of the hilum) shows a 3cms cebtral lesion in the left upper lobe, and a smaller 1cms central nodule in the middle of the left lower lobe. Ashley Davidoff MD
TheCommonVein.net
32325b.8s
keywords
lung cancer carcinoma central lesion malignant satellite nodule
TheCommonVein.net
32315c keywords
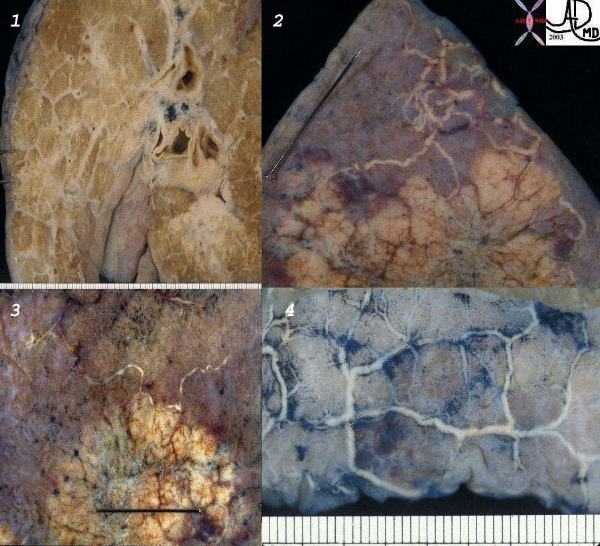
lungs pulmonary pleura secondary lobules interlobular septa thickened parenchymal nodules neoplasm lymphatics distended metastases lymphangitis obliterans gross pathology
Distant Disease
Metastatic disease to the bone can result in pathological fracture and to the spine which at the extreme can cause significant neurological compromise and a need for urgent radiation therapy.
Another dramatic clinical presentation may be as a result of brain metastases, while bilateral adrenal metastases in the extreme can cause an Addisonian crisis.
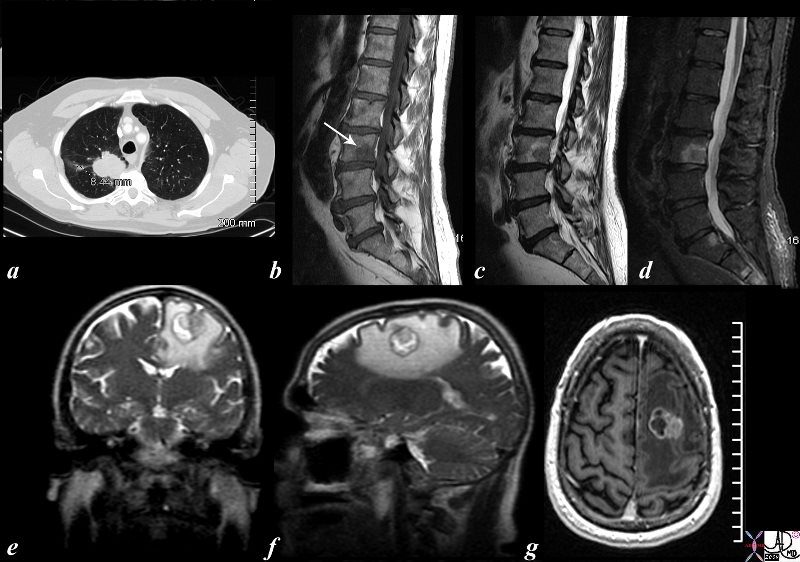
The CTscan and MRI images are from a 56 year old male who presented with back pain and a neurological deficit. The CT scan of the chest shows a right upper lobe lung mass and the MRI of the spine (b= T1, c =T2 and d= STIR) confirm the presence of a metastasis in L3) while MRI of the brain (e= T2 coronal, f = T2 sagittal and g= post gadolinium study) reveal a mass in the high left parietal lobe with surrounding edema (white around the round tumor in e and f) and showing enhancement (g). lung brain spine lumbar spine cancer metastasis metastases vasogenic edema.
Courtesy Ashley Davidoff MD
TheCommonVein.net
87681c02.8s
At autopsy extra thoracic metastatic disease (and in order of diminishing frequency,) is found most commonly in patients with small cell cancer (>95%), adenocarcinoma and large cell carcinoma,(80%) and then squamous cell (>50%).
This coronal reformat of the thoracic spine in a patient with known lung carcinoma and blastic metastasis reveals an ivory vertebra. It is characterised by diffuse involvement with blastic disease. Other focal blastic changes in the vertebra are present as is a large layering posterior pleural effusion.
Courtesy Ashley Davidoff MD
TheCommonVein.net
39006
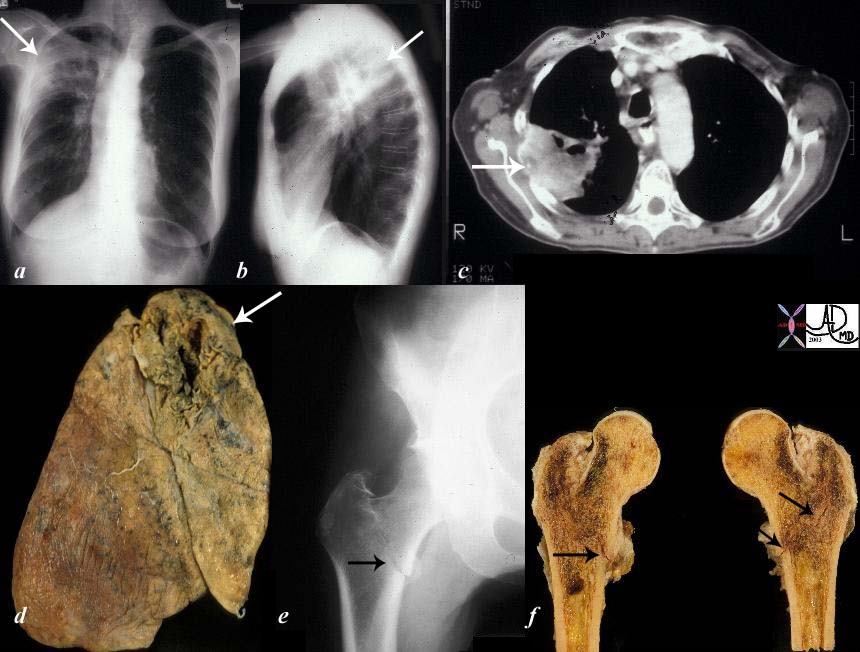
The collage of images reflect a patient with stage IV cavitating primary squamous carcinoma of the RUL (a,b,c,d – white arrows) with COPD. A metastatic lesion to the right femur was complicated by a pathological fracture. (e,f black arrows).
Courtesy Ashley Davidoff MD
TheCommonVein.net
32202c02
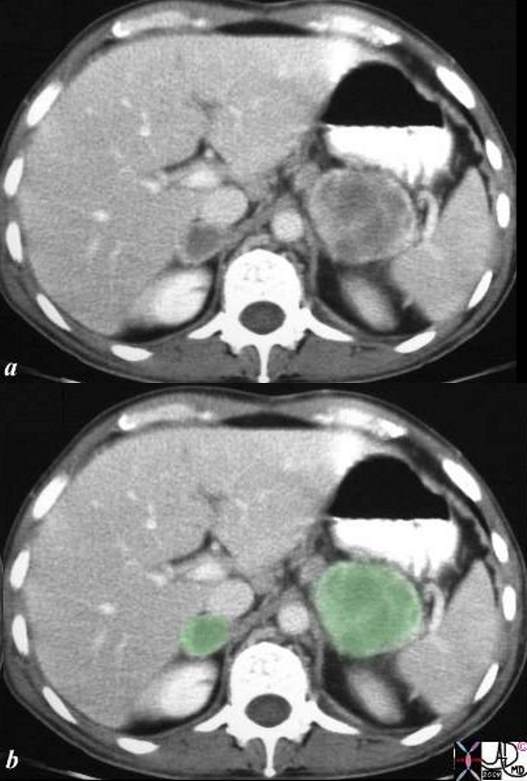
This is a CT scan of adrenal masses and diagnosis of SVC syndrome and diagnosis of lung carcinoma. Courtesy Ashley Davidoff MD. code adrenal mass masses bilateral neoplasm malignant metastasis metastases primary lung imaging radiology CTscan
Courtesy Ashley Davidoff MD
TheCommonVein.net
25767c01.8s

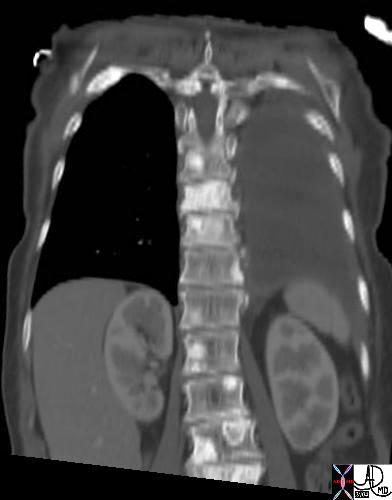
This CT scan reveals a rapidly growing mass in this patient with known squamous cell carcinoma of the lung. A PET scan had shown this to be the only site of disease and therefore it was removed and confirmed to be squamous cell carcinoma. code lung cancer metastasis malignant kidney mass CTscan
Courtesy Ashley Davidoff MD.
TheCommonVein.net
31442.8s
Some of the complications of local extension have been alluded to above and others occur as a result of local lymphatic extension (lymphangitis obliterans), or to distant metastases the most devastating usually being brain metastasis.
At autopsy extra thoracic metastatic disease is found most commonly in patients with small cell cancer (>95%), then adenocarcinoma and large cell carcinoma,(80%) and then
squamous cell (>50%). The adrenals, brain, liver and bone are the common sites of metastatic disease.
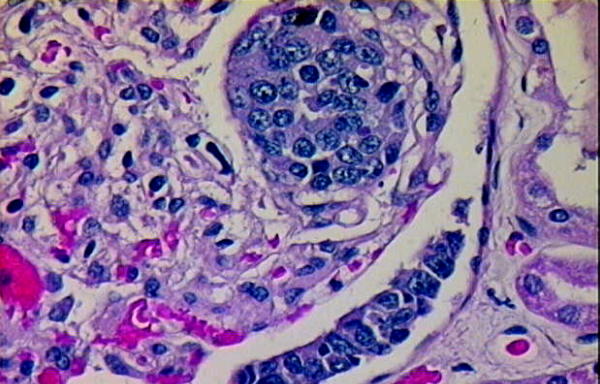
Lung Carcinoma metastatic to Renal Glomerulus.
Courtesy tumorboard.com
54410
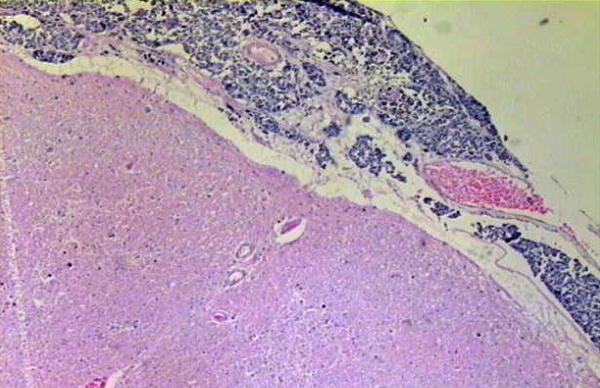
Lung Carcinoma Metastatic to Meninges of Brain.
Courtesy tumorboard.com
54412
Paraneoplastic diseases
Paraneoplastic syndromes occur as a result of lung carcinoma but may be the presenting finding. Endocrine syndromes occur in about 10% of patients with lung carcinoma. Ectopic PTH produced by squamous cell carcinoma may produce hypercalcemia and hypophosphatemia. Small Cell carcinoma (oat cell carcinoma) may produce ectopic ADH or possibly atrial natriuretic factor resulting in hyponatremia with the syndrome of inappropriate secretion of antidiuretic hormone. SCLC may also produce ACTH resulting in electrolyte disturbances, particularly hypokalemia. Lung carcinoma can be associated with a number of paraneoplastic syndromes which elaborate hormone-like factors resulting in often clinically significant metabolic derangement.
The hormones that are commonly produced include ADH (anti diuretic hormone) and ACTH (adrenocorticotrophic hormone antidiuretic hormone), parathormone, calcitonin, gonadotropins and serotonin.
ACTH and ADH ectopic production occur predominantly with the small cell carcinomas. Carcinoid syndrome can also be associated with the small cell carcinoma, but if present is more likely to be associated with a carcinoid tumor of the bronchus. Squamous cell tumors more commonly are responsible for hypercalcemia
Autoimmune antibodies can be elicited by lung carcinoma producing a number of neuro muscular aberrancies.
Clubbing occurs in 30% of cases (usually non-small cell carcinomas) and hypertrophic pulmonary osteoarthropathy in about 5% of cases (usually adenocarcinomas)
Small cell carcinoma (oat cell cancer) is associated with neurologic-myopathic syndromes seen in about 1% of patients. All types are uncommonly associated with autoimmune induced peripheral neuropathy, cerebellar and or cortical degeneration, and polymyositis
Hypercoagulable states and other and other hematological disorders occur in about 5%, while dermatomyositis and acanthosis nigricans, and nephropathies occur in about 1% of patients.
Lymphatic Obstruction

TheCommonVein.net
32317
keywords
lungs pulmonary pleura secondary lobules interlobular septa thickened parenchymal nodules neoplasm lymphatics distended metastases lymphangitis obliterans gross pathology crab cancer shape d
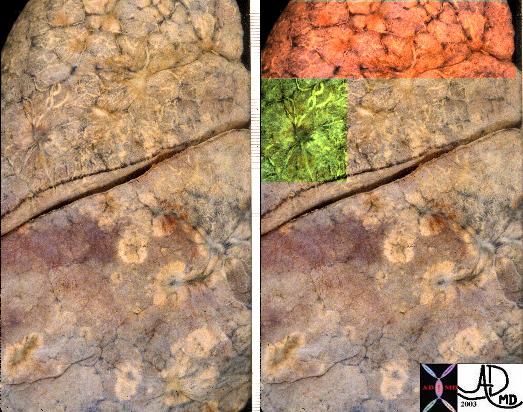
TheCommonVein.net
32313c keywords
lungs pulmonary secondary lobules interlobular septa thickened parenchymal nodules neoplasm lymphatics distended metastases lymphangitis obliterans gross pathology
TheCommonVein.net
32315c keywords
lungs pulmonary pleura secondary lobules interlobular septa thickened parenchymal nodules neoplasm lymphatics distended metastases lymphangitis obliterans gross pathology

Courtesy tumorboard.com
54411 Keywords
lung pulmonary lymphatics neoplasm malignant malignancy primary lung adenocarcinoma histopathology
Ashley Davidoff MD
TheCommonVein.net
32269b see 680249
keywords
lungs pulmonary mass RUL neoplasm malignant primary lymphatics lymphangitis imaging plain film CXR CTscan PETscan
Links and References