
Size
Small
CXR Small Pleural Effusion
Blunting of the Right Costophrenic Angle
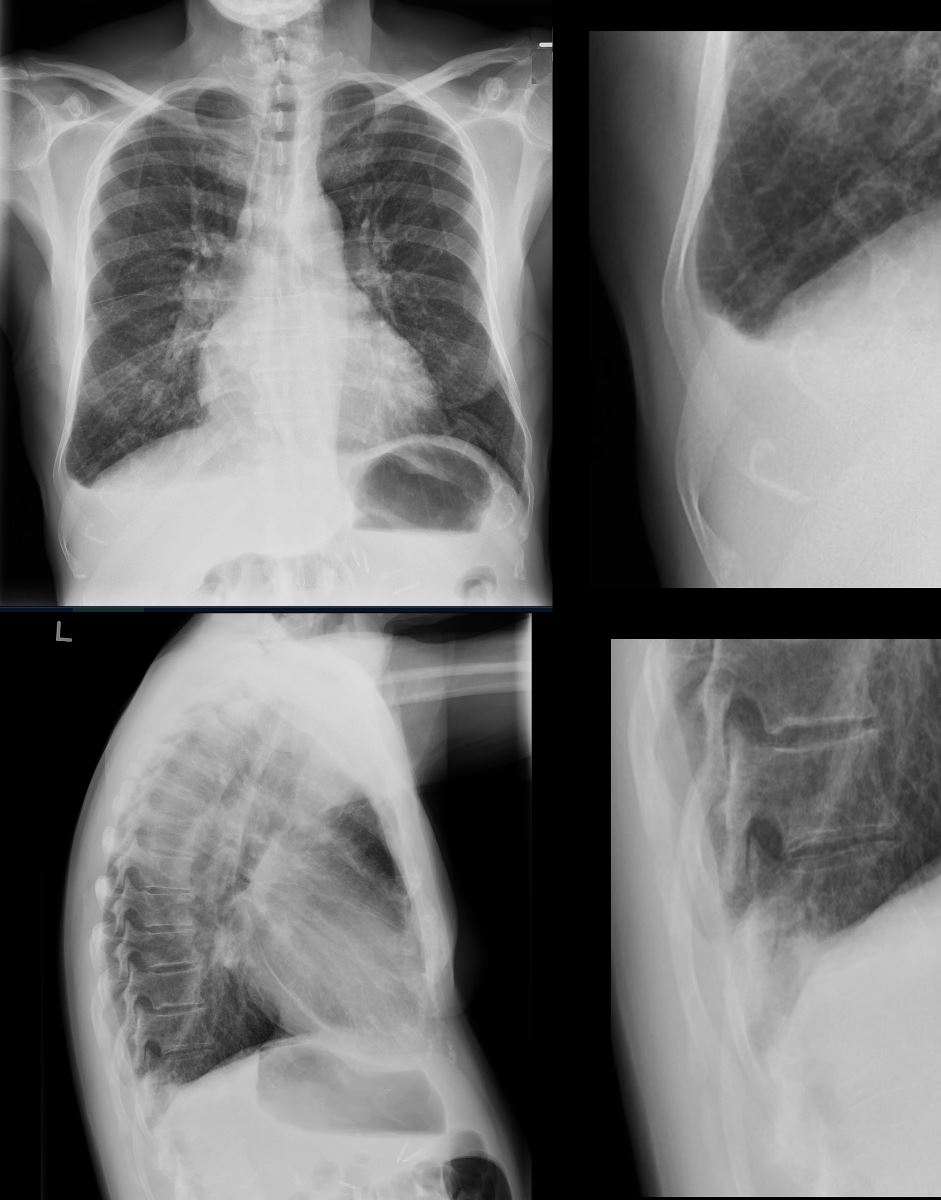
50-year-old man presents with dyspnea. PA and lateral view shows blunting of the right costophrenic angle in the P-A view (above) and confirmed on the lateral view (below)
Courtesy Ashley Davidoff MD TheCommonVein.net 136550c

85-year-old female with a history of lung cancer, presents with a dyspnea and hypotension. Reconstruction of the CT scan in the coronal plane, shows a large right pleural effusion under pressure with herniation into the left chest (white asterisk e,and f) , with mediastinal shift to the left (yellow arrowhead b, c, d). In addition, there is compression of the heart with back up of venous return due the pressure effect on the heart and vascular structures. Among the structures showing venous distension are the SVC (blue arrowhead, c) right sided upper limb veins (blue arrowhead d) and the left upper pulmonary veins (red arrowhead, d and f). The density of the systemic venous abd arterial systems is similar, but vascular structures as noted by the green arrowhead in a could represent venous collaterals.
Ashley Davidoff MD TheCommonVein.net
Shape
Simple Transudate with Crescent Shape Obeying the Laws of Gravity
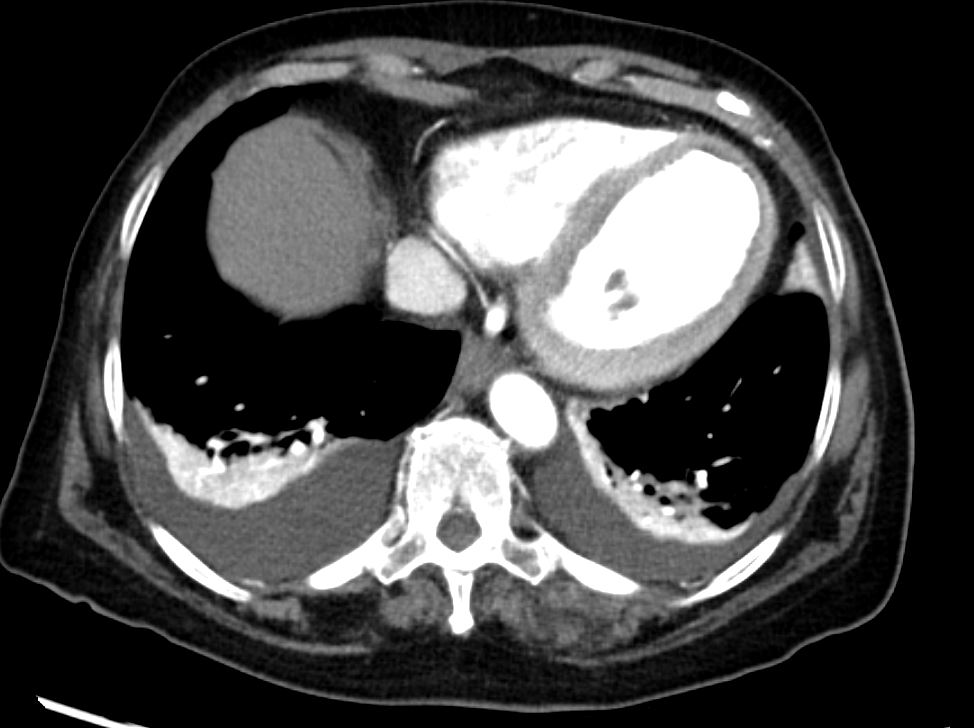
CT scan of the lung bases shows moderate sized bilateral effusions with compressive atelectasis. The atelectatic lung shows hyper-enhancement
Ashley Davidoff MD TheCommonVein.net 135685
Complex Exudative without Crescent Shape on the Right and Not Obeying the Laws of Gravity and Crescentic Shape on the Left

Position
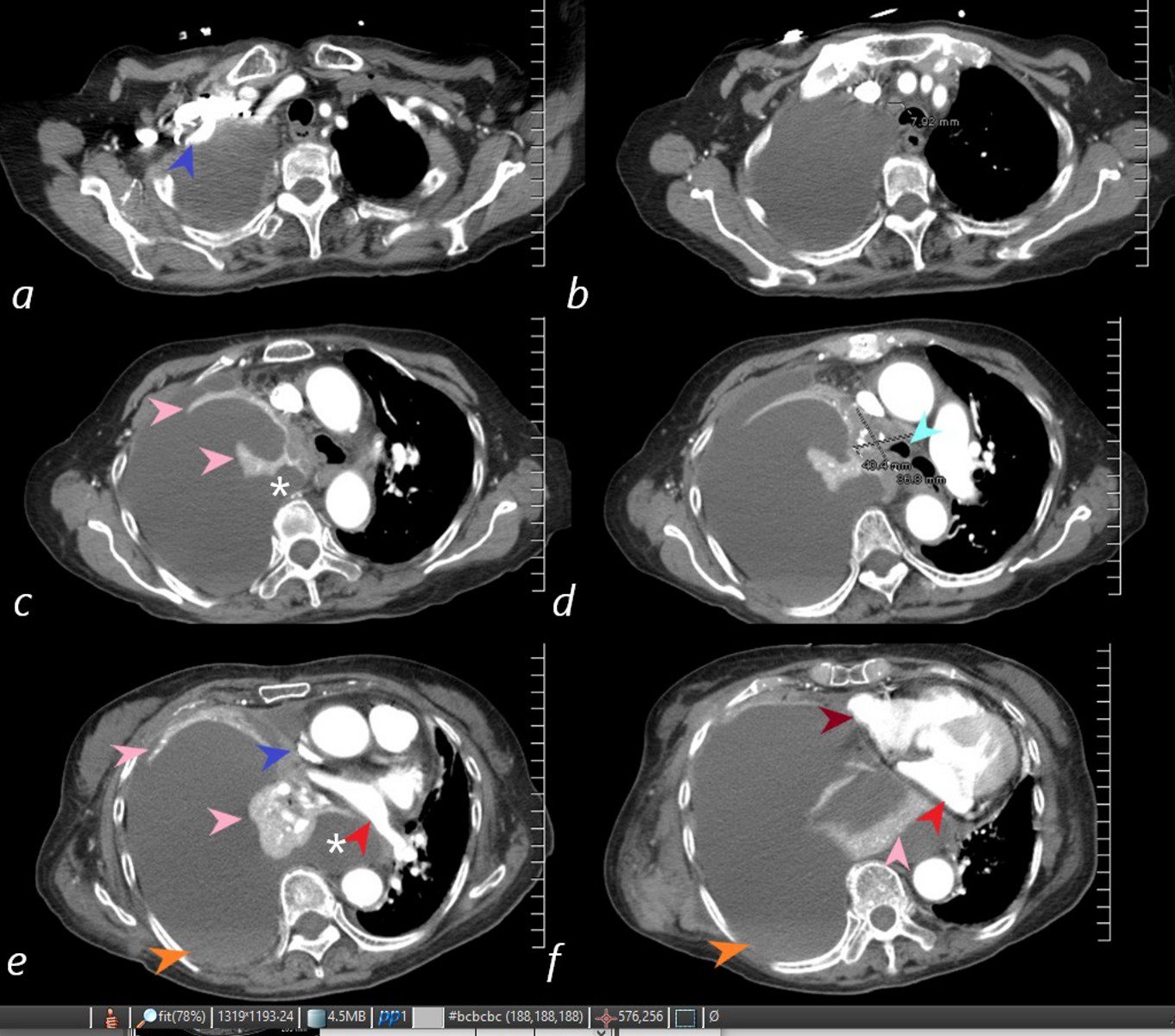
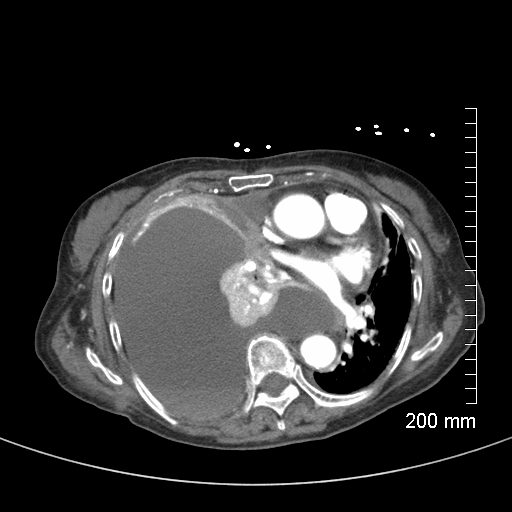
85-year-old female with a history of lung cancer, presents with a dyspnea and hypotension. CT scan shows a large right pleural effusion under pressure, suggestion of blood in the pleural cavity (orange arrowheads e, f) and mediastinal shift to the right. In addition, there is compression of the heart with back up of venous return due the pressure effect on the heart and vascular structures. Among the structures showing compressive effects are the SVC (blue arrowhead, c) with venous distension on right sided upper limb veins (blue arrowhead a). There is also pressure effect on the trachea with narrowing (light blue arrow d) The effusion in the right pleural cavity with atelectatic lung herniates into the left hemithorax, (white asterisk c, e). There is a dense sediment in the pleural fluid (orange arrowheads, e and f) suggesting blood in the pleural cavity. The left atrium is compressed (red arrowhead, e, f), and the right atrium is compressed (maroon arrow f).
Ashley Davidoff MD TheCommonVein.net
Character
High Density Effusion with Loculated Air
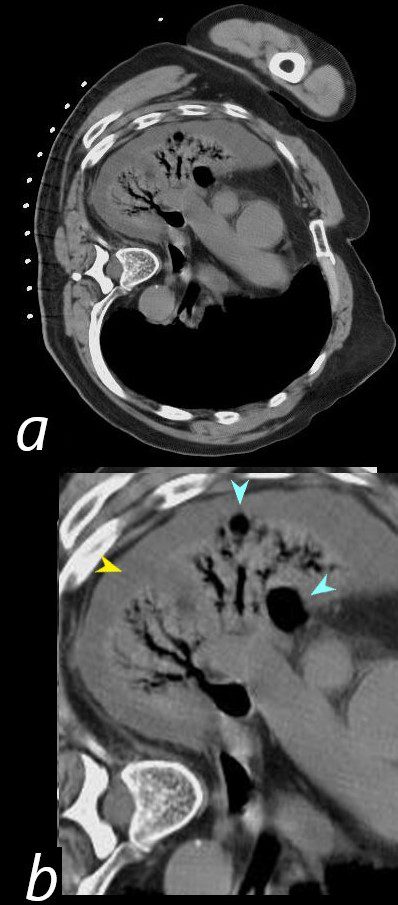
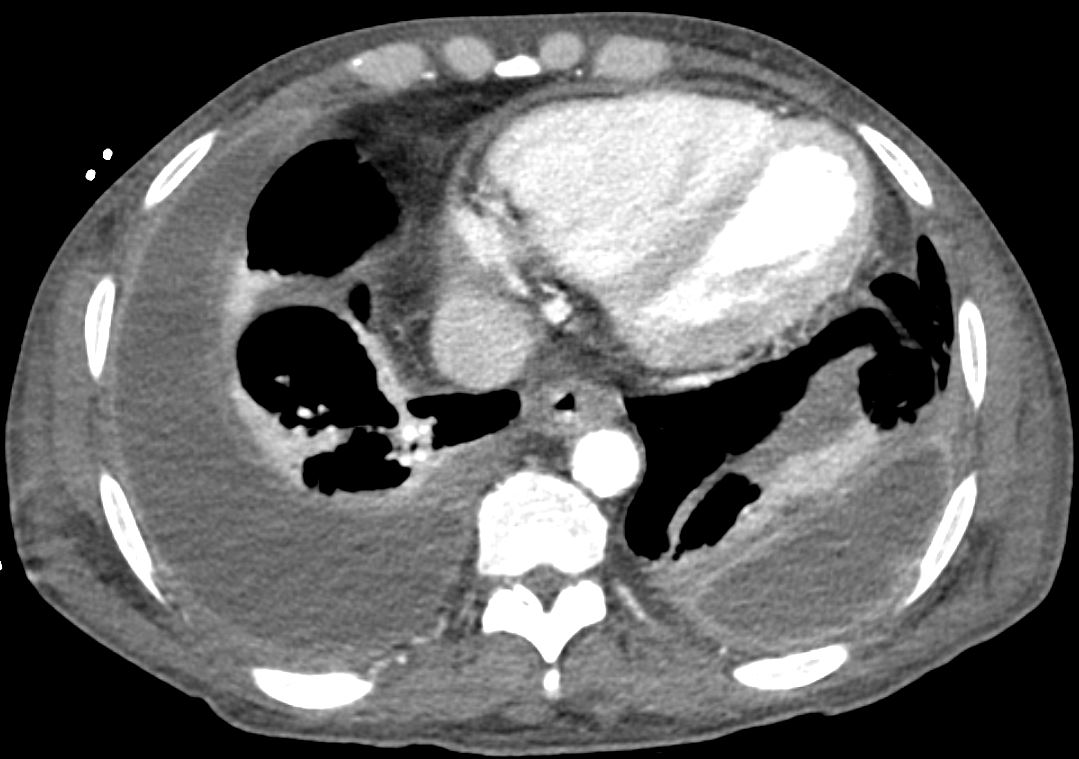
54-year-old female presents with a cough, fever and leukocytosis and multicentric lung abscesses. The patient continued to be febrile with rising white cell count. CT in the axial plane with the patient in decubitus position prior to diagnostic aspiration shows compressive atelectasis of the right upper and right lower lobes by a complex para-pneumonic effusion (b, yellow arrowhead). Air pockets within the effusion (b, teal blue arrowheads) and the relative hyperdensity of the effusion confirm its complexity. Air bronchograms are noted.
Ashley Davidoff MD TheCommonVein.net 19599cL01
Effusion with Sediment
Ashley Davidoff MD TheCommonVein.net RnD 106Lu
Infection
CT Parapneumonic Effusion – Empyema Thickened Pleura
CT scan in a 76-year-old male shows a left lower lobe consolidation (b, white arrowhead) associated with a loculated parapneumonic effusion with trapped air bubbles (b yellow arrowhead) which was culture positive and a thickened enhancing pleura
Ashley Davidoff MD TheCommonVein.net 136194cL
Parapneumonic Complex Effusion and Compressive Atelectasis
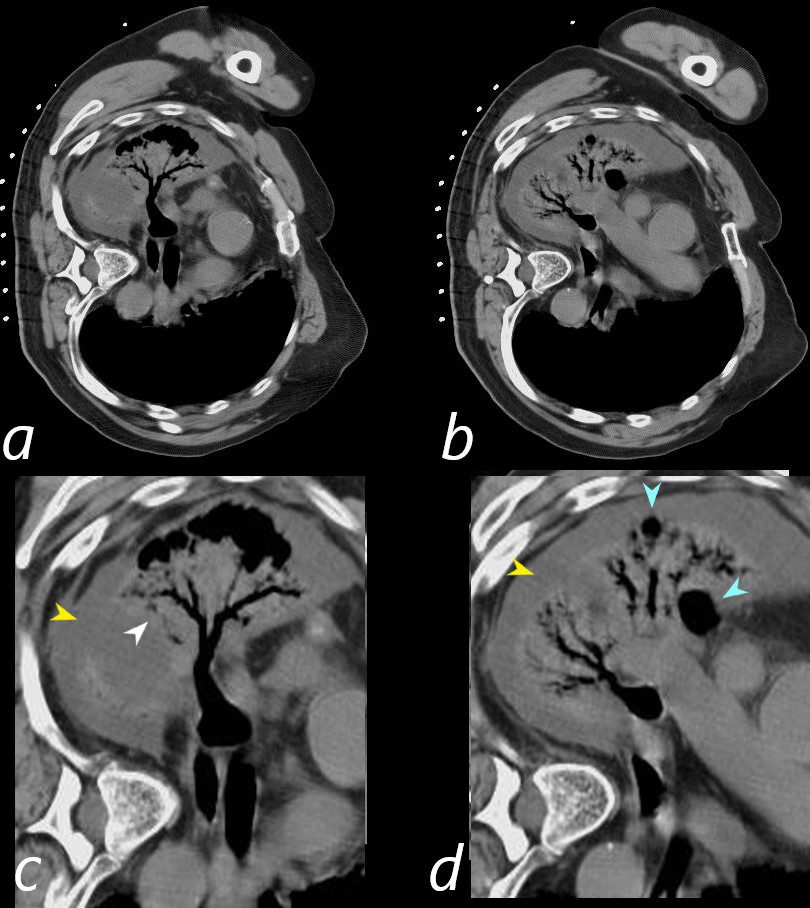
54-year-old female presents with a cough, fever and leukocytosis and multicentric lung abscesses. The patient continued to be febrile with rising white cell count. CT in the axial plane with the patient in decubitus position prior to diagnostic aspiration shows compressive atelectasis of the right upper and right lower lobes by a complex para-pneumonic effusion (c,d yellow arrowheads). Air pockets within the effusion (d, teal blue arrowheads) and the relative hyperdensity of the effusion confirm its complexity. Air bronchograms are noted.
Ashley Davidoff MD TheCommonVein.net 19599cL
Inflammation
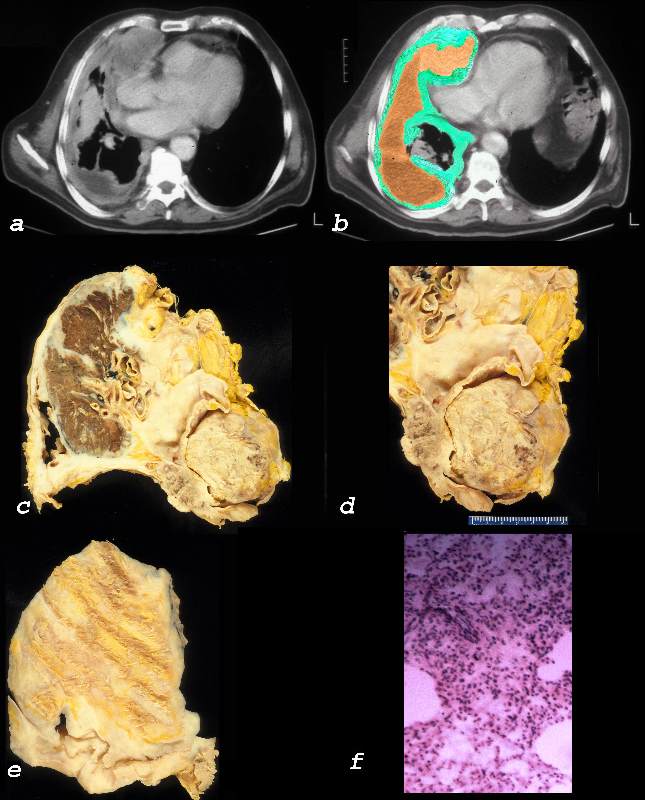
Malignancy
Axial CT scan with contrast of 71-year-old male shows bilateral complex and loculated effusions with thickened enhancing pleura. Pleural tap of the left effusion revealed evidence of lymphoma likely related to the patients underlying herpes virus infection. An entity called primary effusion lymphoma (PEL) is a rapidly progressing non-Hodgkin’s B-cell lymphoma that develops in body cavities
Ashley Davidoff MD TheCommonVein.net 135684

Ashley Davidoff MD TheCommonVein.net 32640c01L01.8
Mechanical
Atelectasis
Trauma
Metabolic
Circulatory-
CHF
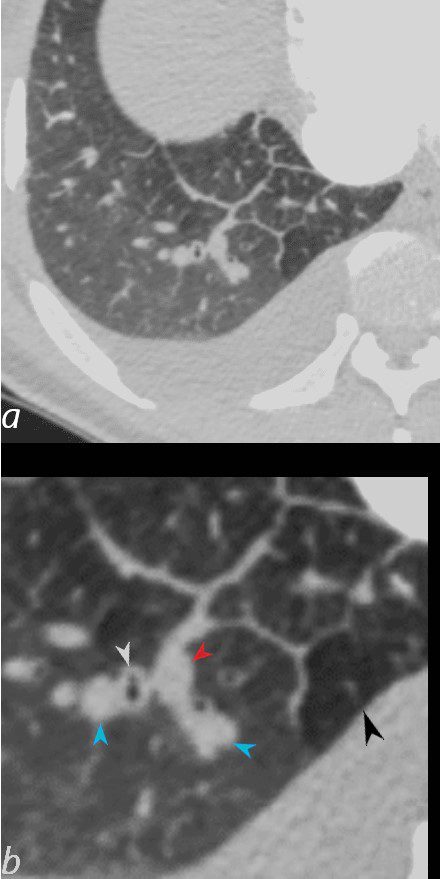
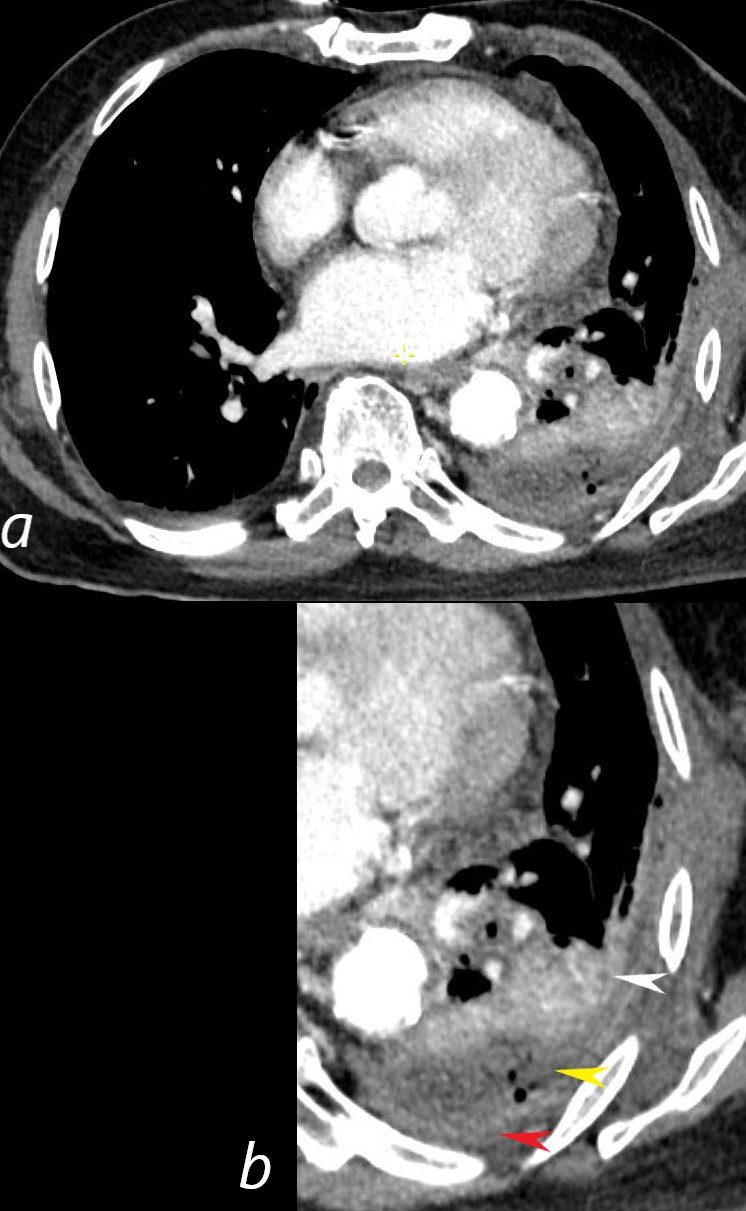
50-year-old female with diabetes, chronic renal failure and congestive heart failure. CT in the axial plane through the right posterior recess, shows thickened interlobular septa at the right base, congested arterioles (light blue arrowheads, b), alongside the bronchioles, peribronchial cuffing (white arrowheads, b), a congested pulmonary venule in the interlobular septum (red arrowhead arrowheads, b), ground glass changes and a secondary lobule demonstrating mosaic attenuation (black arrowhead arrowheads, b). The IVC is dilated and a small complex effusion is present.
Ashley Davidoff MD TheCommonvein.net 135783cL 193Lu
Early Severe CHF Bilateral Effusions Right Greater than Left
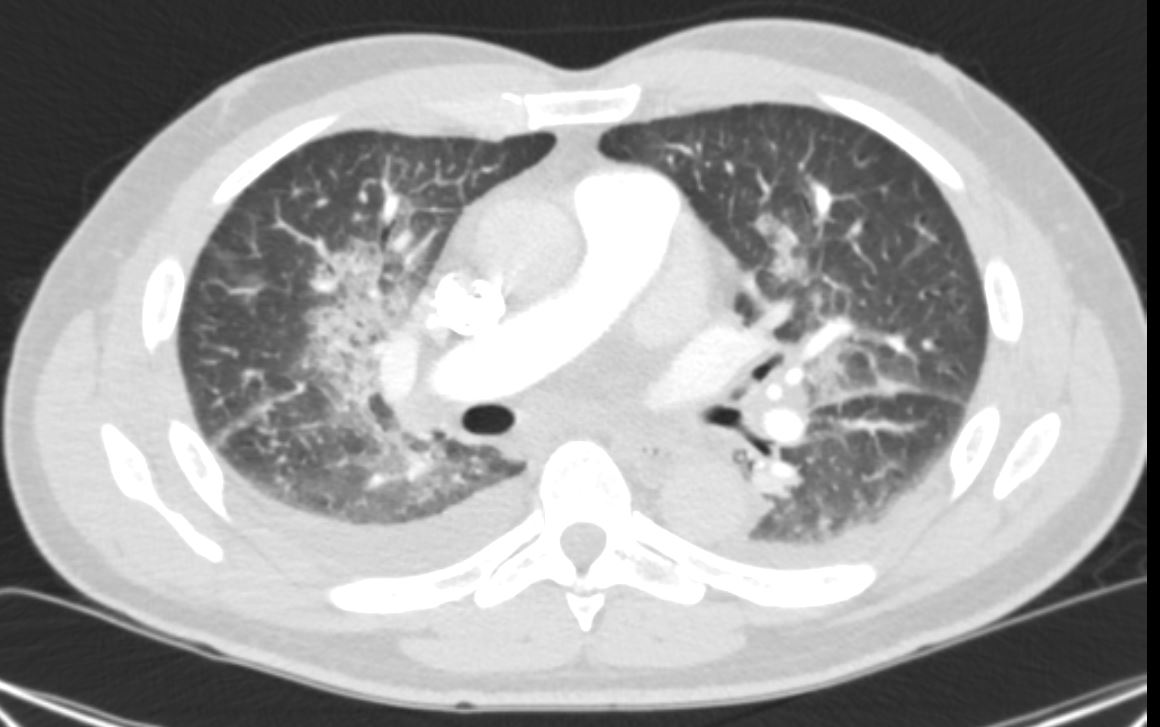
50 year-old male presents with severe dyspnea and orthopnea. CT in the axial plane shows early severe CHF, with perihilar ground glass changes and small bilateral pleural effusions – right greater than left. These findings are consistent with early severe heart failure with a projected LVEDP of greater than 30mmHg
Ashley Davidoff MD TheCommonVein.net 285Lu 135760
Hemorrhage
Immune Infiltrative Idiopathic Iatrogenic