
Infection Inflammation Malignancy Mechanical/Atelectasis Trauma Metabolic
Circulatory- Hemorrhage
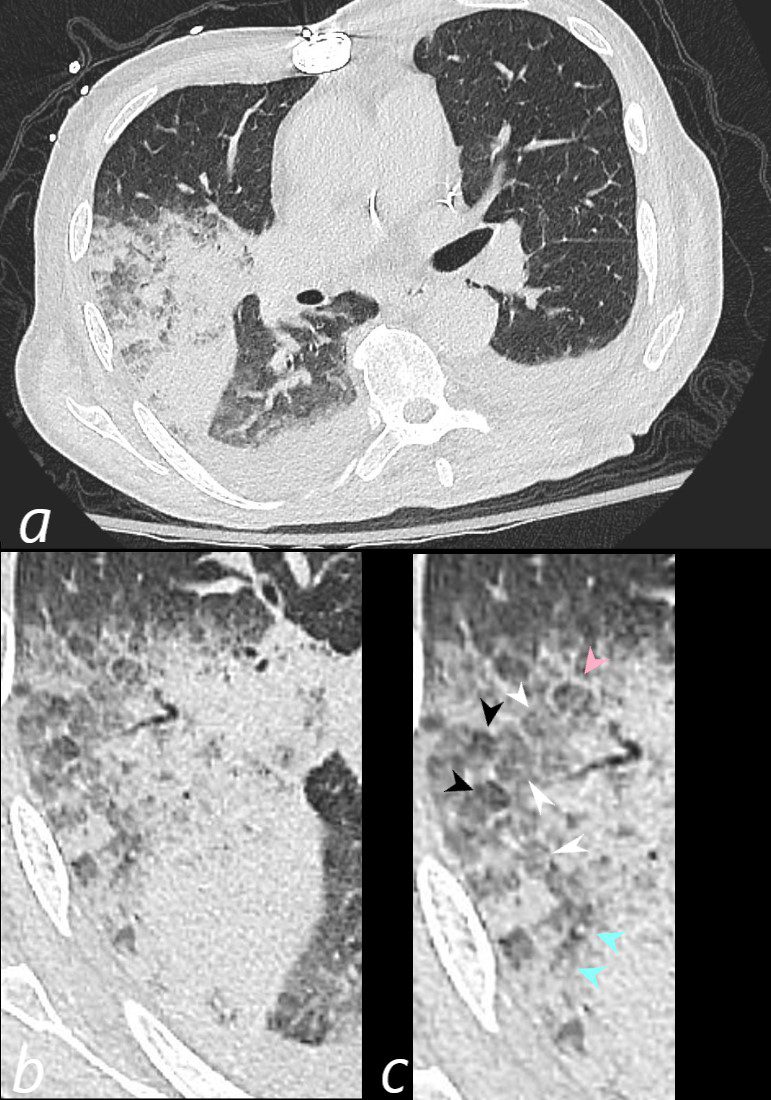
75-year-old man on blood thinners s/p aortic valve replacement presents with hemoptysis s/p trauma. He was afebrile and without an elevated white count
Axial CT at the level below the carina shows medial displacement of the major fissure by a dense right upper lobe consolidation. The mass effect on the major fissure likely results from a hematoma. Anterior to the consolidation there is a combination of ground glass opacity with thickened interlobular septa, and minor region of subsegmental consolidation with air bronchograms, likely resulting from hemorrhage.
The lower panels magnify the regions of the heterogeneity of the secondary lobule with most showing ground glass changes, some normal or with mosaic attenuation (black arrowheads, c), some showing thickened smooth interlobular septa (pink arrowhead, c) and others revealing centrilobular nodules (teal arrowheads, c).
There are bilateral effusions
Ashley Davidoff MD TheCommonVein.net 165Lu 135851cL
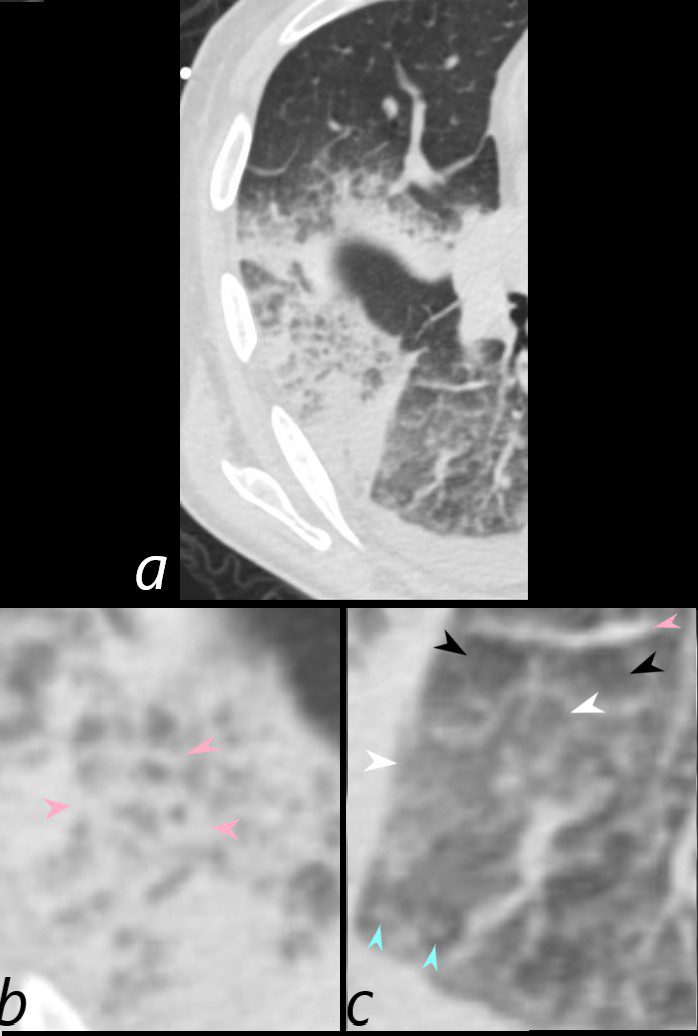
75-year-old man on blood thinners s/p aortic valve replacement, s/p trauma, presents with hemoptysis. He was afebrile and without an elevated white count
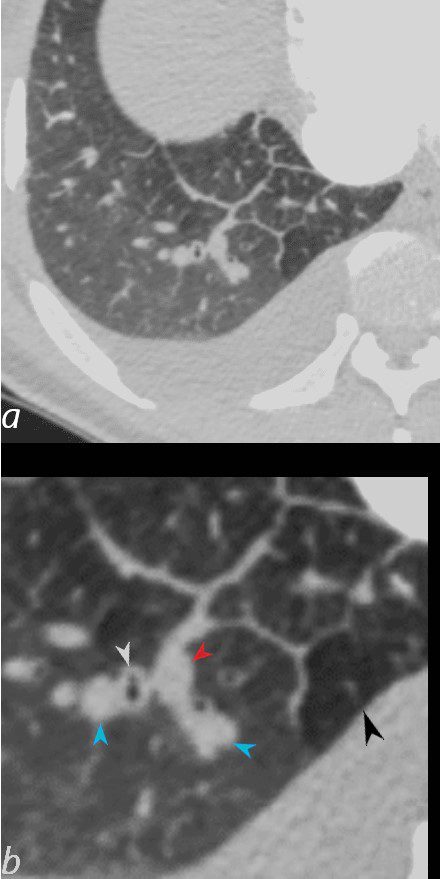
Axial CT at the level below the carina at the inferior aspect of the hematoma shows heterogenous changes of the secondary lobules. The changes in the post segment of the right upper lobe (b) show significantly thickened interlobular septa (pink arrowheads) and relatively small secondary lobules caused by the compression of the hematoma. The changes in the apical segment of the lower lobe (c) show a combination of secondary lobules with ground glass changes (white arrowheads) some normal or with mosaic attenuation (black arrowheads), some showing mildly thickened smooth interlobular septa (pink arrowheads), and others revealing centrilobular nodules (teal arrowheads).
There is a right sided effusion
Ashley Davidoff MD TheCommonVein.net 165Lu 135853cL
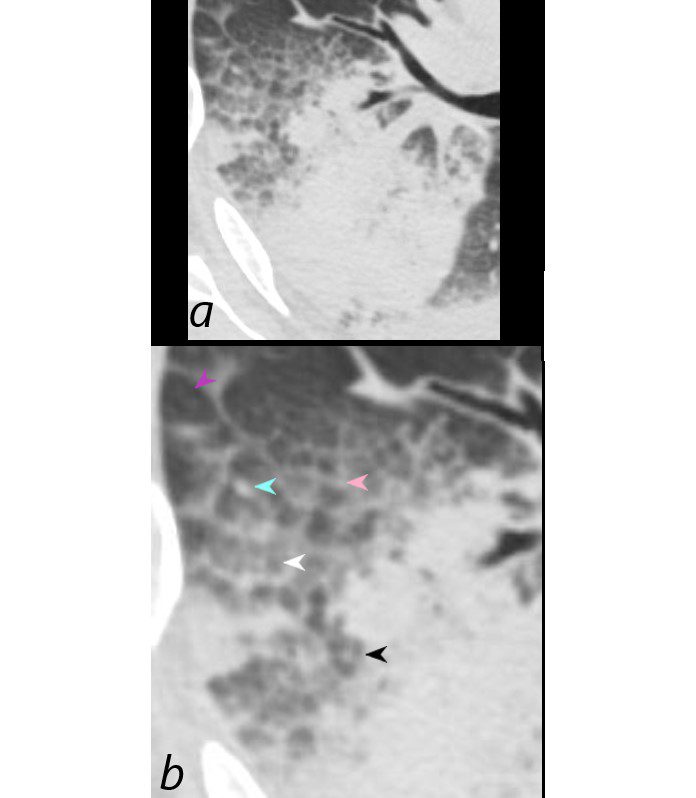
75-year-old man on blood thinners s/p aortic valve replacement, s/p trauma, presents with hemoptysis. He was afebrile and without an elevated white count
Axial CT at the level below the carina shows heterogenous changes of the secondary lobules. The changes in the post segment of the right upper lobe (a, and magnified in b) show thickened interlobular septa (pink arrowhead) and mostly relatively small secondary lobules caused by the compression of the hematoma, but also by virtue of their more centrally located position. Compare their size to the larger more peripherally located secondary lobule (purple arrowhead). There is also a combination of secondary lobules with ground glass changes (white arrowhead) some normal or with mosaic attenuation (black arrowheads), some showing mildly thickened smooth interlobular septa (pink arrowhead), and others revealing centrilobular nodules (teal arrowhead).
Ashley Davidoff MD TheCommonVein.net 165Lu 135854cL
Immune Infiltrative Idiopathic Iatrogenic Idiopathic
Infection
Active TB Transbronchial Spread with
Extensive Tree in Bud Changes
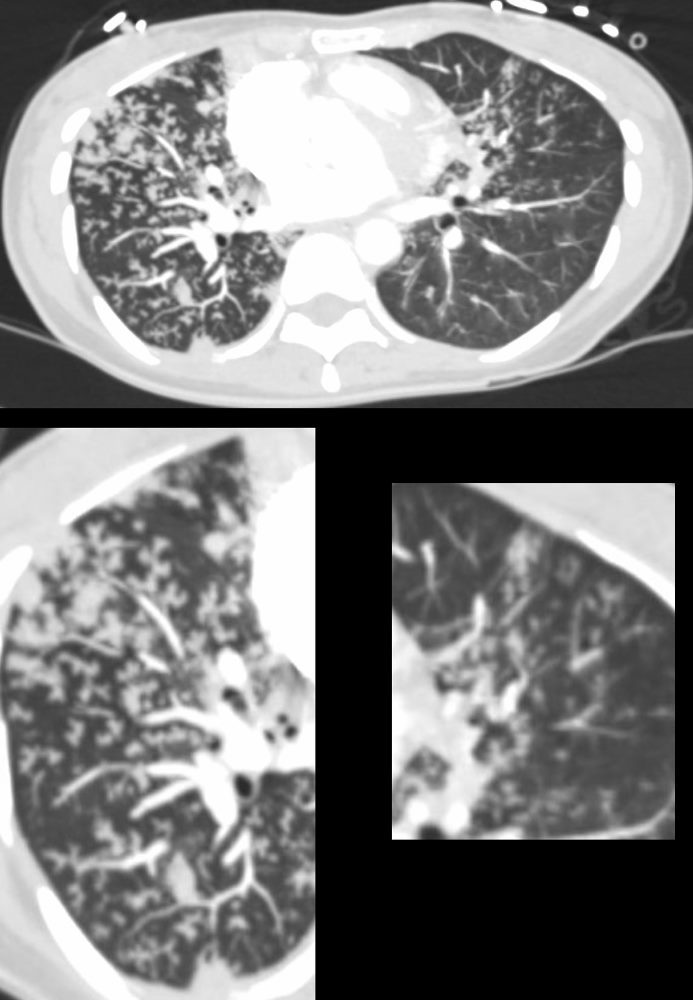
39-year-old immigrant Vietnamese male presents night sweats fever and cough. CT in the axial plane through the mid chest shows innumerable micronodules resulting from transbronchial spread with resultant tree in bud pattern scattered through the right lung (magnified in the right lower image). There are minimal similar changes in the lingula (magnified left lower image)..
Ashley Davidoff MD TheCommonvein.net 135789c 006Lu
Subsegmental and Small Airway Disease Right Upper Lobe
Active TB
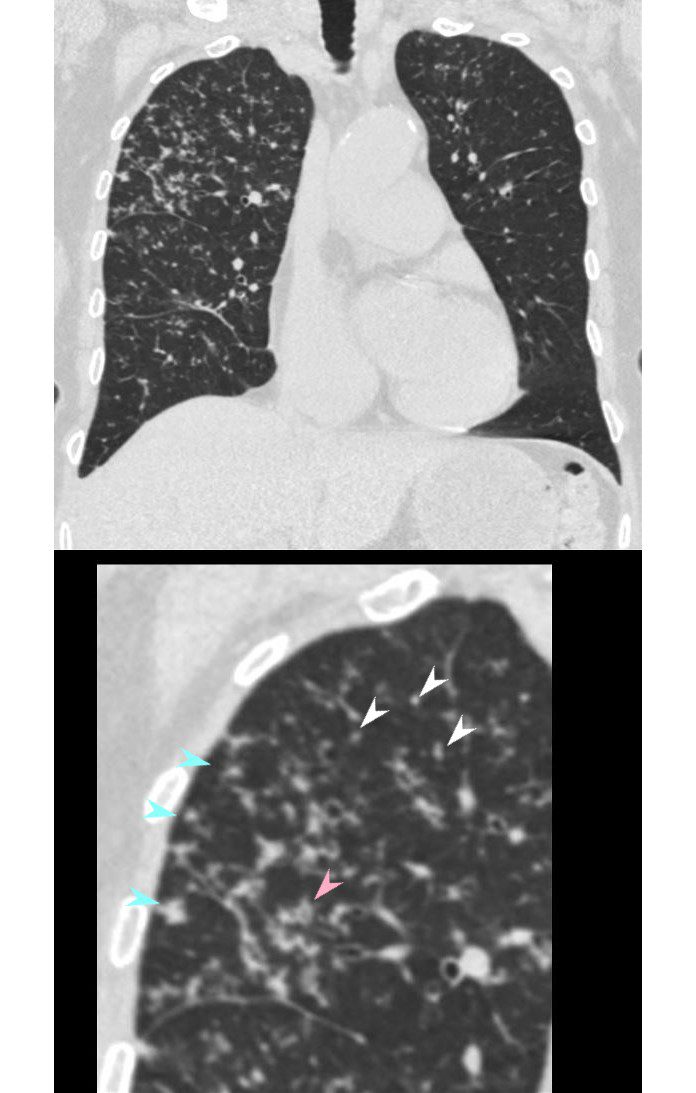
68 year old female presented with malaise night sweats weight loss QuantiFeron gold positive, with a past history of treated TB in her native country as a child. CT shows subsegmental and small airway disease dominant in the right upper lobe characterized by airway thickening (pink arrowhead),ground glass micronodules (white arrowheads) and centrilobular nodules (teal blue arrowheads). There are lesser changes in the right lower lobe, and left upper lobe. Bronchoscopy isolated Mycobacterium complex. She was treated with good result
Ashley Davidoff MD TheCommonVein.net 135822cL 192Lu
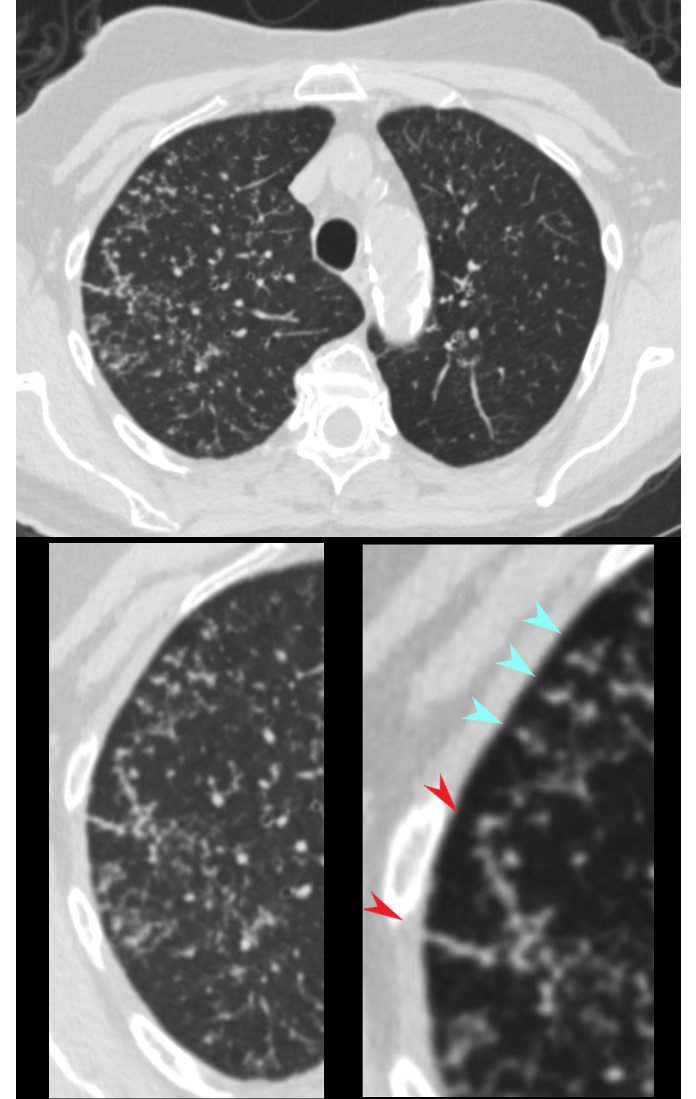
CT in the axial plane shows extensive small airway disease dominant in the right upper lobe characterized by innumerable, ground glass micronodules, centrilobular nodules (teal blue arrowheads) and nodular thickening of the interlobular septa likely reflecting lymphatic involvement (red arrowheads)
Ashley Davidoff MD TheCommonVein.net 135825cL 192Lu
Mycobacterium avium complex (MAC)
Micronodules Centrilobular Nodules, Thickened Nodular Interlobular Septa –
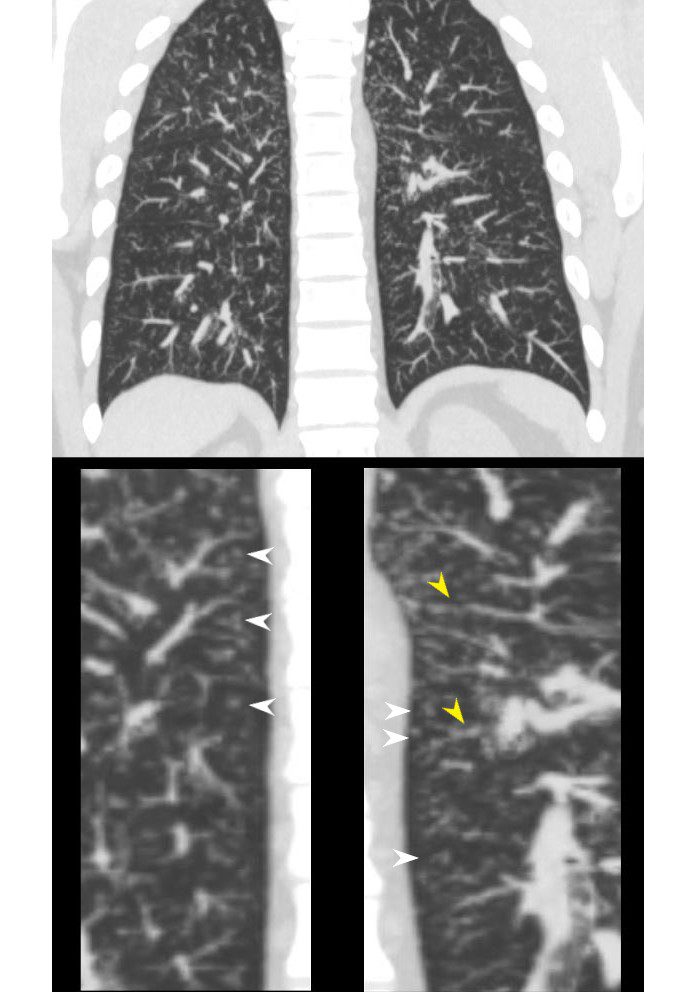
29-year-old male presents with night sweats
CT in the coronal plane in the posterior aspect of the chest shows innumerable ground glass micronodules most scattered throughout both lung fields. The inserts in the lower panel, highlight the centrilobular nodules (white arrowheads) and thickened nodular changes in the interlobular septa and along the venules, likely due to lymphatic involvement. Wedge biopsy and culture revealed a diagnosis of MAC (mycobacterium avium complex)
Ashley Davidoff MD TheCommonvein.net 135817cL 247Lu
48-year-old male with history of TB
Latent TB with
Calcified Septal Granulomas and
Calcified Centrilobular Nodule

48-year-old male with history of TB
Axial CT through the mid chest shows calcified granulomas along an interlobular septum of a secondary lobule. There is also a centrilobular calcified granuloma These calcifications are likely centered around the lymphatics of the bronchovascular bundle and in the interlobular septum
Ashley Davidoff MD TheCommonvein.net 132604c
Miliary Histoplasmosis Centrilobular and Peri-lymphatic
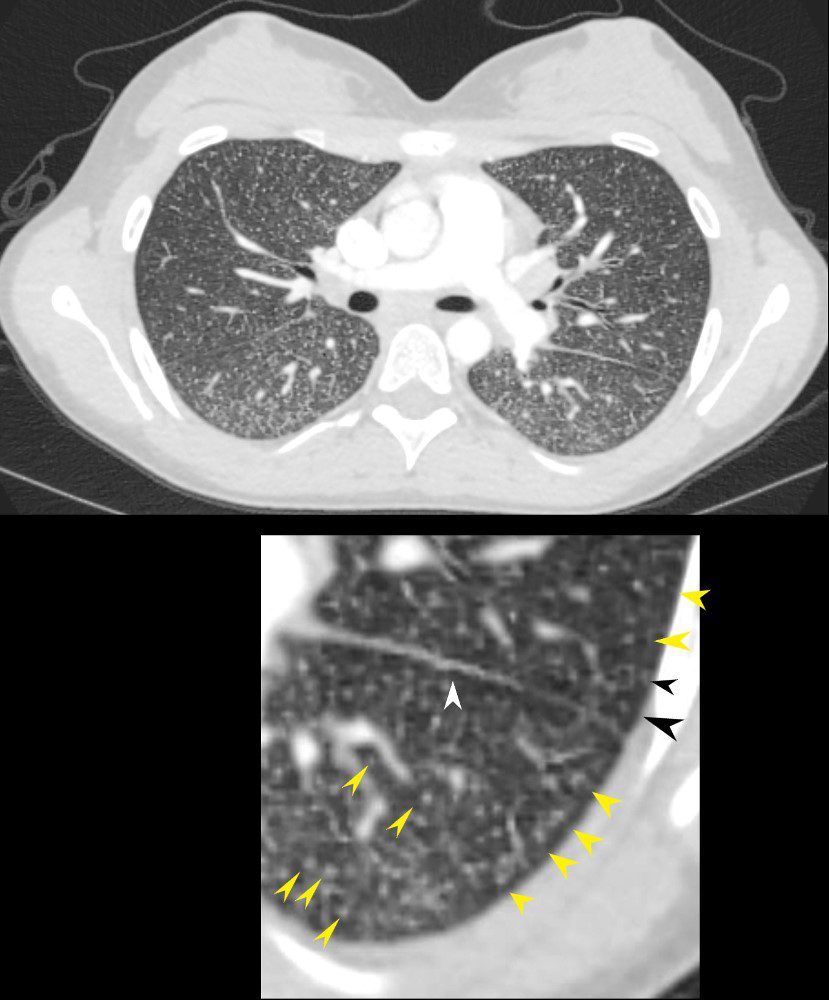
22-year-old female presents with flu like symptoms
CT of the chest at the level of the main pulmonary artery shows extensive diffuse miliary disease. Some of the nodules are centrilobular (yellow arrowheads). Some of the secondary lobules suggest mosaic attenuation (black arrowhead). The nodular and irregular appearance on the fissure (white arrowhead) indicates peri-lymphatic distribution.
Ashley Davidoff MD TheCommonvein.net 131708cL
Allergic Bronchopulmonary Aspergillosis ABPA
60 year old male with history of asthma, allergic bronchopulmonary aspergillosis (ABPA)
CT scan shows left upper lobe bronchiectasis and soft tissue/fluid impaction in the anterior segmental and subsegmental airways associated with tree in bud appearance (yellow arrowhead) and centrilobular nodules (red arrowhead) reminiscent of associated small airway disease
Ashley Davidoff TheCommonVein.net
CHF and Enlarged Pulmonary Arteriole
50-year-old female with diabetes, chronic renal failure and congestive heart failure. CT in the axial plane through the right posterior recess, shows thickened interlobular septa at the right base, congested arterioles (light blue arrowheads, b), alongside the bronchioles, peri-bronchial cuffing (white arrowheads, b), a congested pulmonary venule in the interlobular septum (red arrowhead arrowheads, b), ground glass changes and a secondary lobule demonstrating mosaic attenuation (black arrowhead arrowheads, b). The IVC is dilated and a small complex effusion is present.
Ashley Davidoff MD TheCommonvein.net 135783cL 193Lu
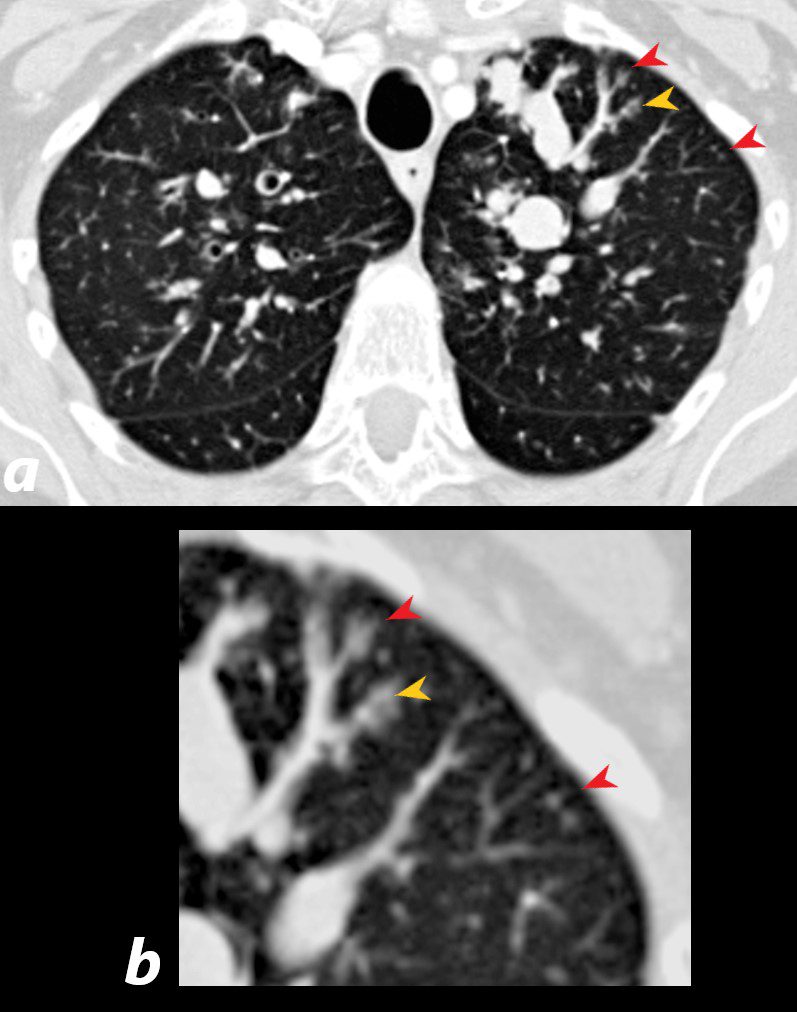
UIP Centrilobular Nodules
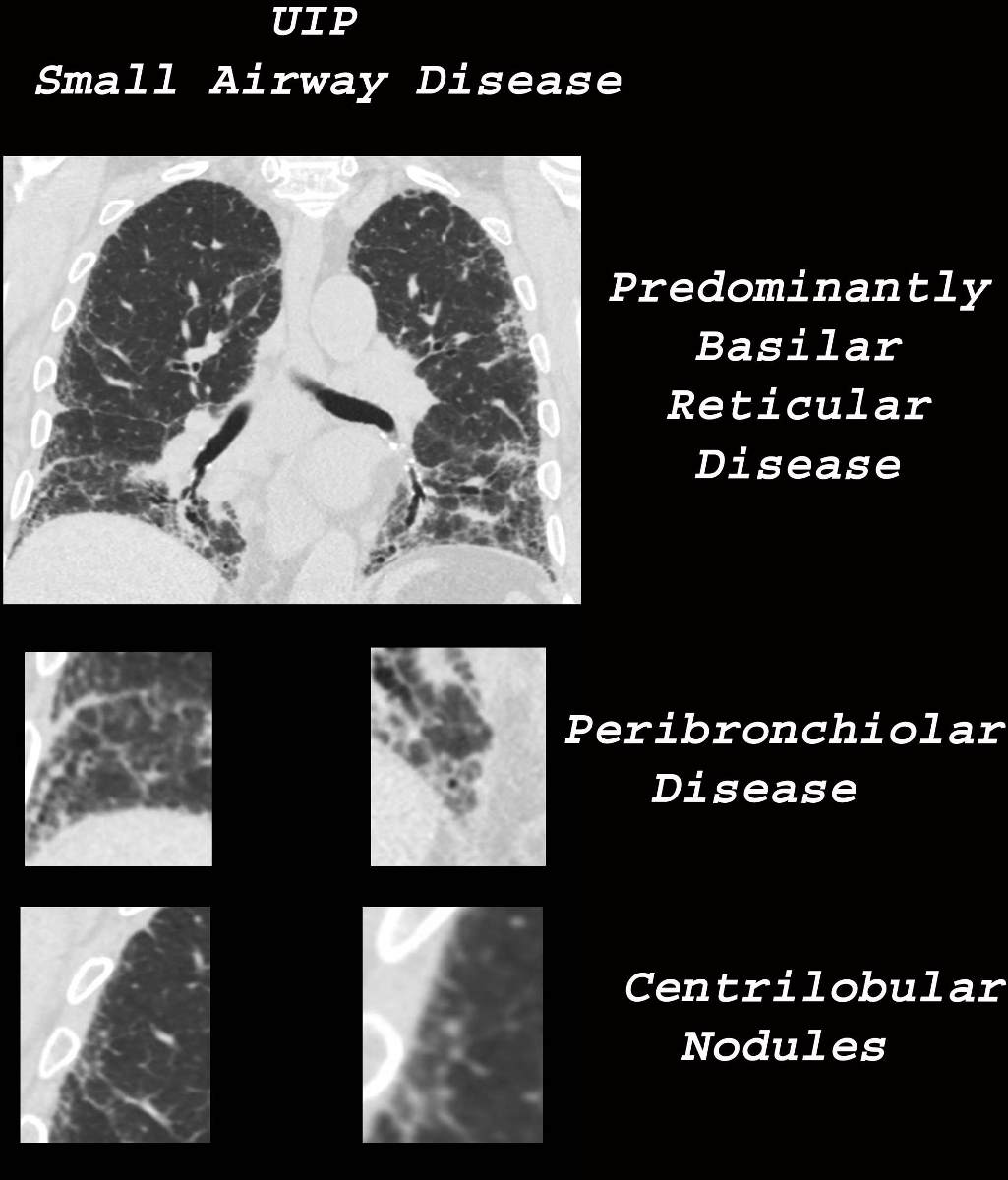
Ashley Davidoff MD TheCommonVein.net uip-002c-CT
- Bronchiole
-
- Endobronchial TB
- Non TB Mycobacteria and other Granulomatous Infections
- Infectious Bronchiolitis
- Cystic Fibrosis
- Bronchiolar Inflammation
- HP
- Asthma
- ABPA
- Langerhans Cell Histiocytosis
- OP and COP
- Smokers Bronchiolitis
- Asbestosis
- Follicular Bronchiolitis
- Angiocentric Disease
- CHF
- Pulmonary Hypertension
- Vasculitis
- Talcosis
- Hemorrhage
- Hemosiderosis
- Metastatic Calcification
- Lymphatic Disease
- Sarcoidosis
- Silicosis
- Coal Workers Pneumoconiosis
- Lymphangitic Disease
- LIP
-
Links and References
- TCV