
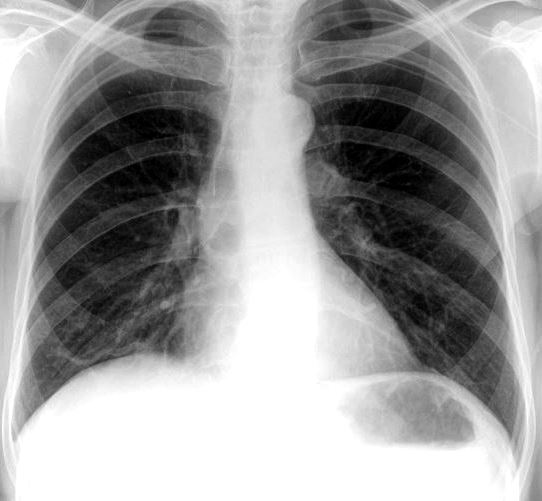
ET Tube
- Normal – 3- 5cms above the carina (head neutral position)
- around T5-T7
-

Normal Position of the the ET tube in relation to the Carina Normal Position of the the ET tube in relation to the Carina


The position of the ETT is dependent on the position of the head. If the neck is flexed, the tip of the tube descends in the trachea.
If included in the film, the mandible can be used for assessment of whether the neck is in a neutral position. In a neutral position, the lower border of the mandible should be projected over C5/C6. When flexed, the mandible projects around T1 and in extension, over C3/C4.
The carina is usually projected over T5-T7 (it descends with increasing age).
The desired position of an ETT is 5 ± 2 cm above the carina, but markedly varies with neck position and rotation and hence, the inclusion of the mandible is a helpful indicator:
- flexed: 3 cm (± 2 cm) above carina
- neutral: 5 cm (± 2 cm) above carina
- extended: 7 cm (± 2 cm) above carina
Venous Lines

Venous Line
Courtesy Radiopedia
Tunneled Dialysis Catheter

Courtey Radiopedia

Courtey Radiopedia
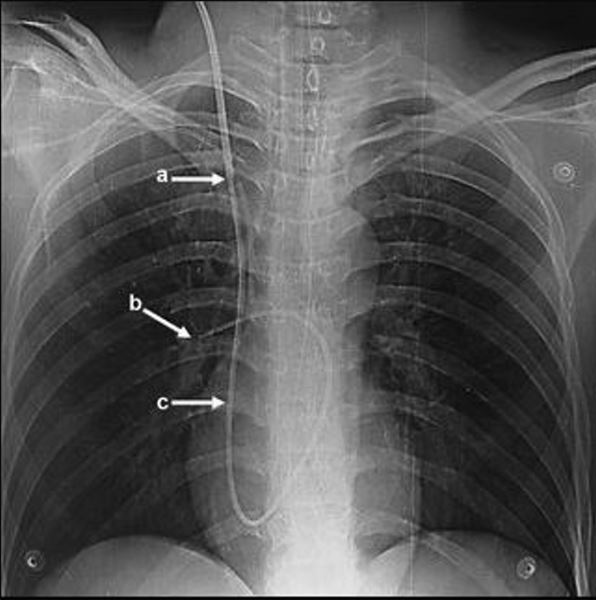
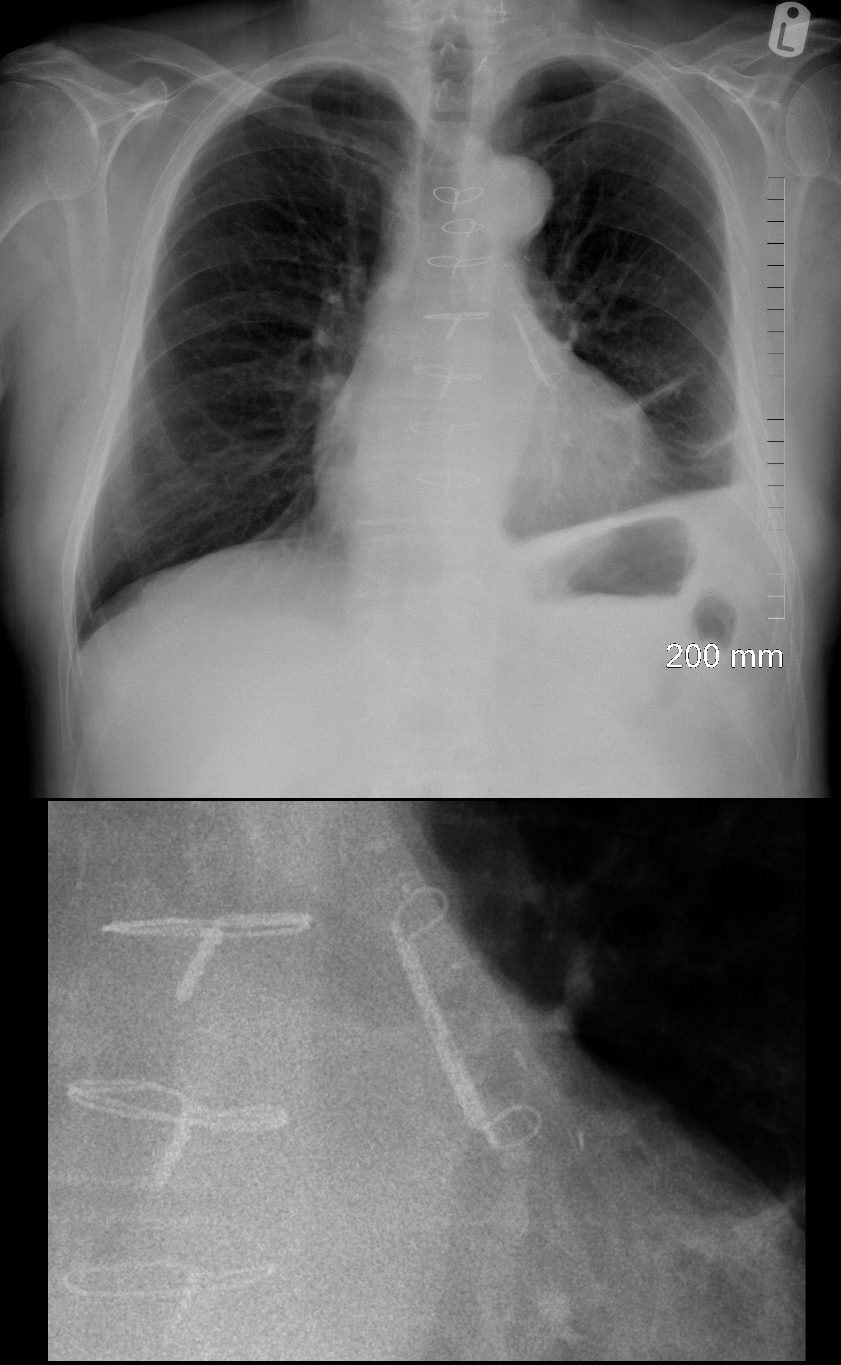
Swan Ganz Line
No further than the right main stem bronchus. Should not extend beyond the proximal interlobar artery (within 2cms of the hilum)
NG Tubes


NG Tube needs Advancement
CXR
Ashley Davidoff MD
thecommonvein.net

CXR
Ashley Davidoff MD
thecommonvein.net
Chest Tubes
Apical for pneumothorax and basilar for pleural effusion

Ashley Davidoff MD
thecommonvein.net
Pacemakers
Dual Lead Pacemaker
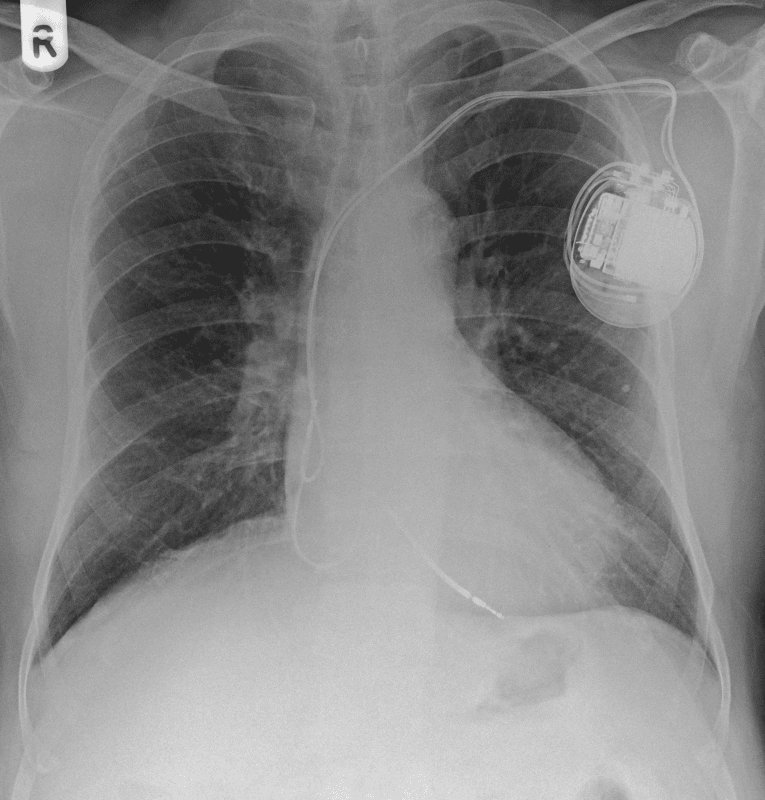
Courtesy Stephanie C Torres-Ayala, Guido Santacana-Laffitte, and José Maldonado
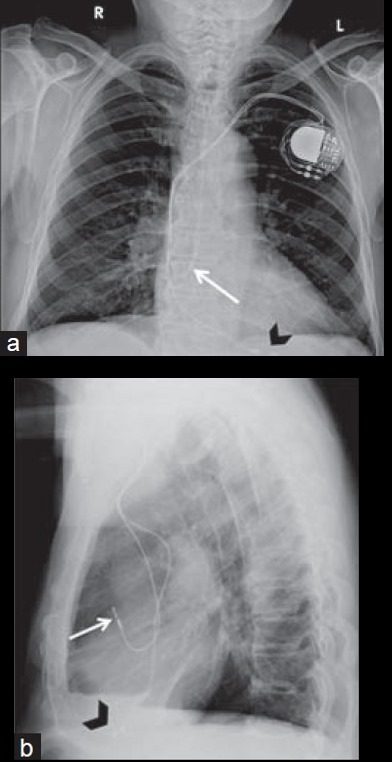
Biventricular Leads and Defibrillators
Gregory Marcus, MD, MAS, FACC
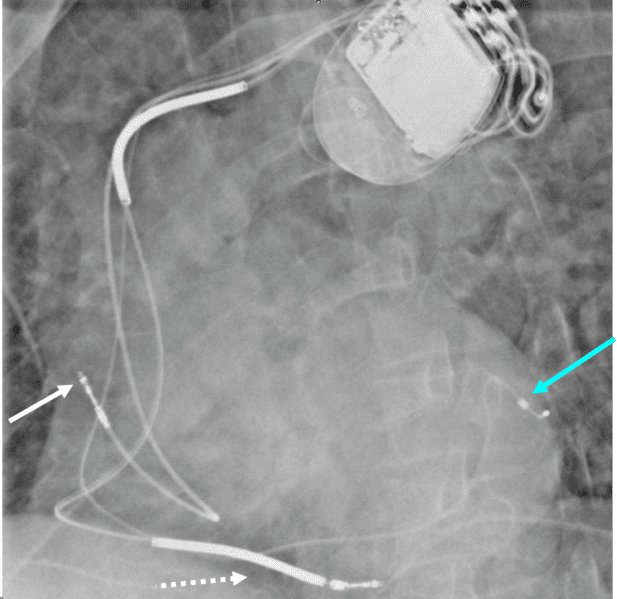
Dual lead pacemaker with defibrillator, with one electrode in the right atrial appendage and the second in the right ventricle. The thickened portions on the leads reflect the defibrillator component.
Ashley Davidoff MD
thecommonvein.net
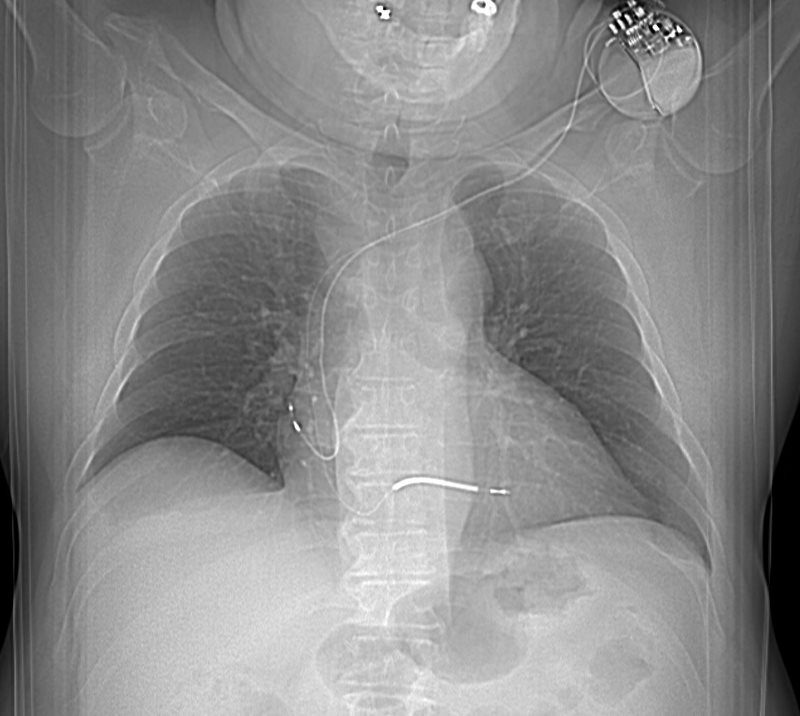
Dual lead pacemaker with defibrillator, with one electrode in the right atrial appendage and the second in the right ventricle. The thickened portions on the leads reflect the defibrillator component.
Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net
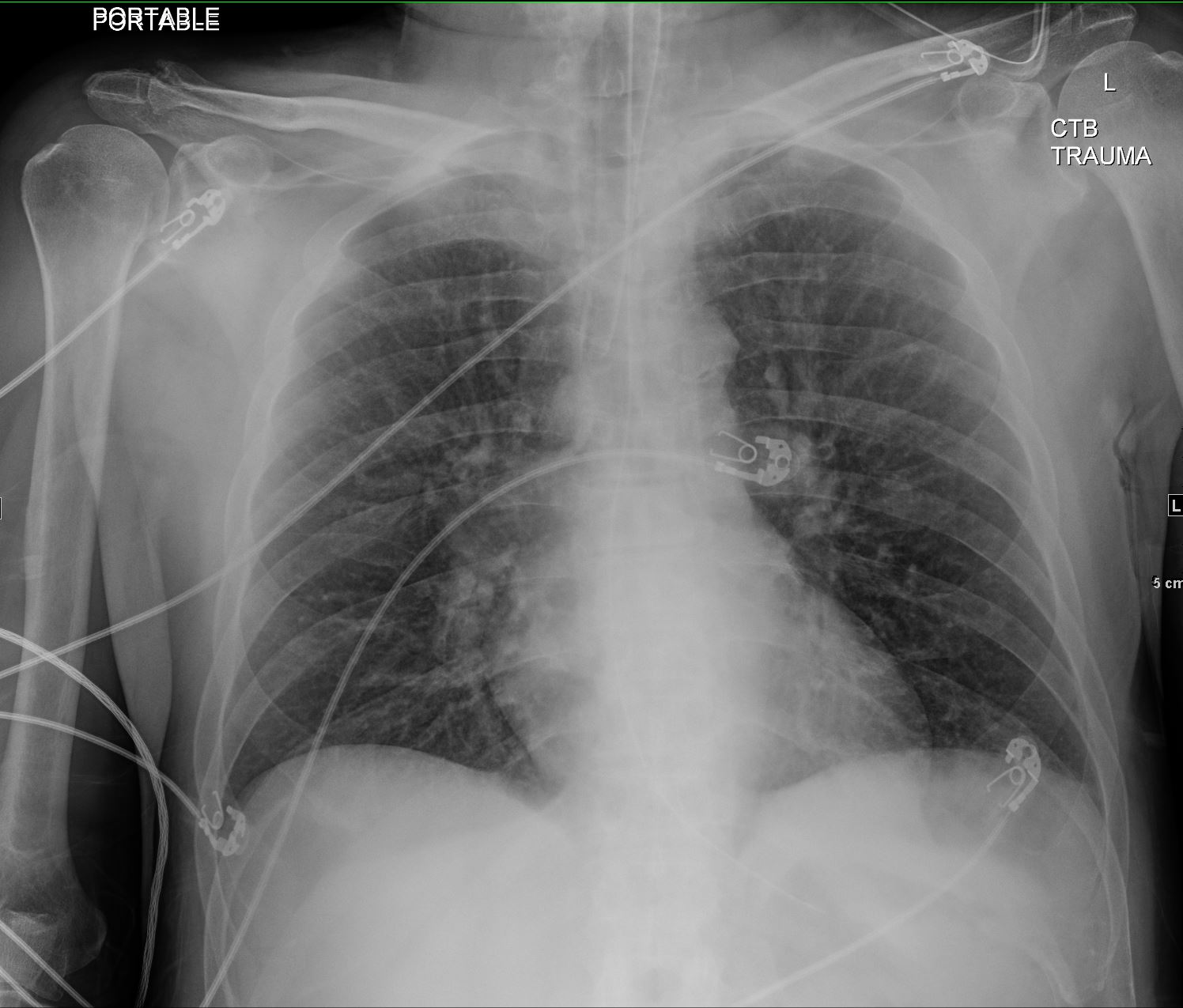
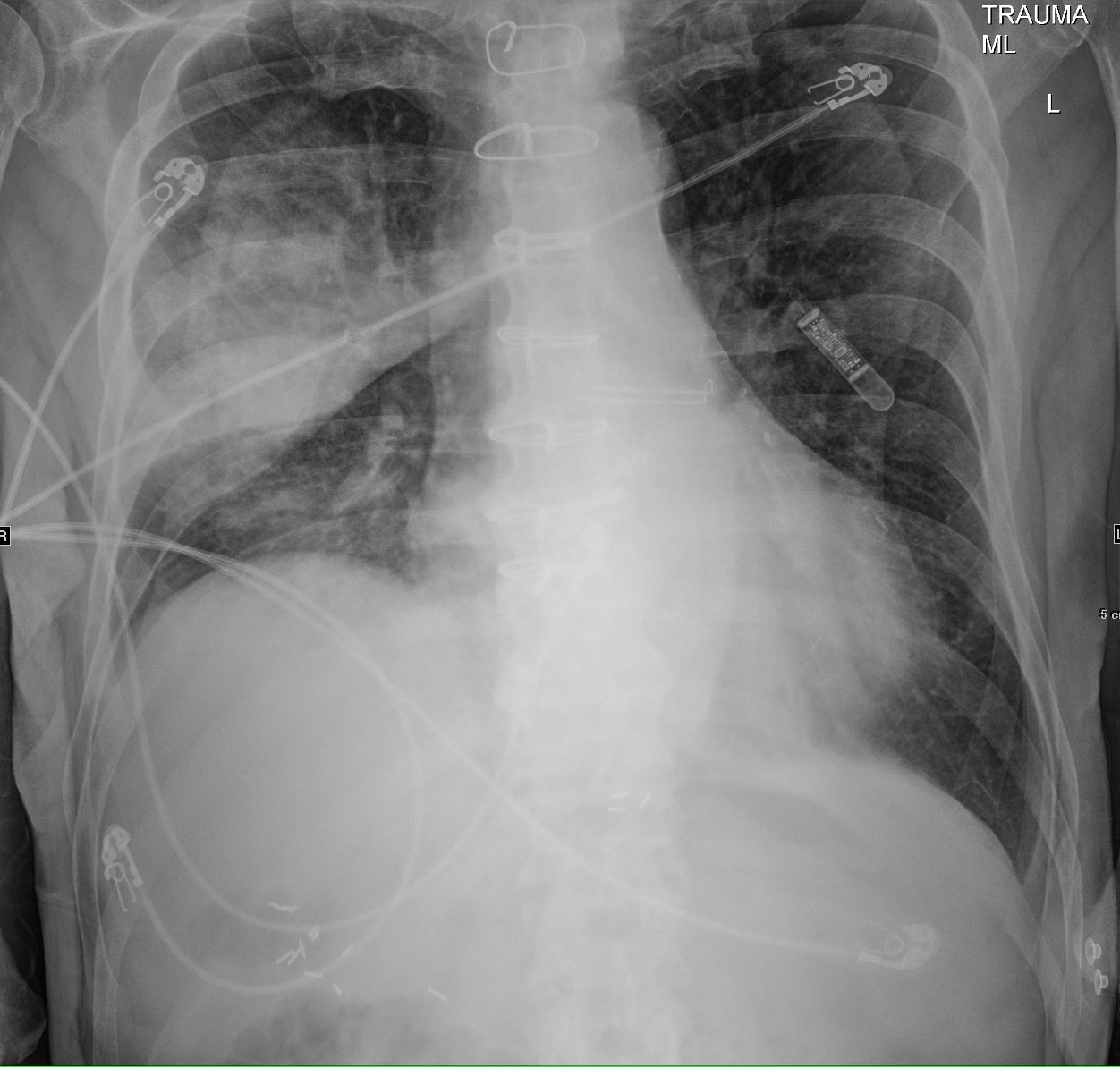
External Defibrillator
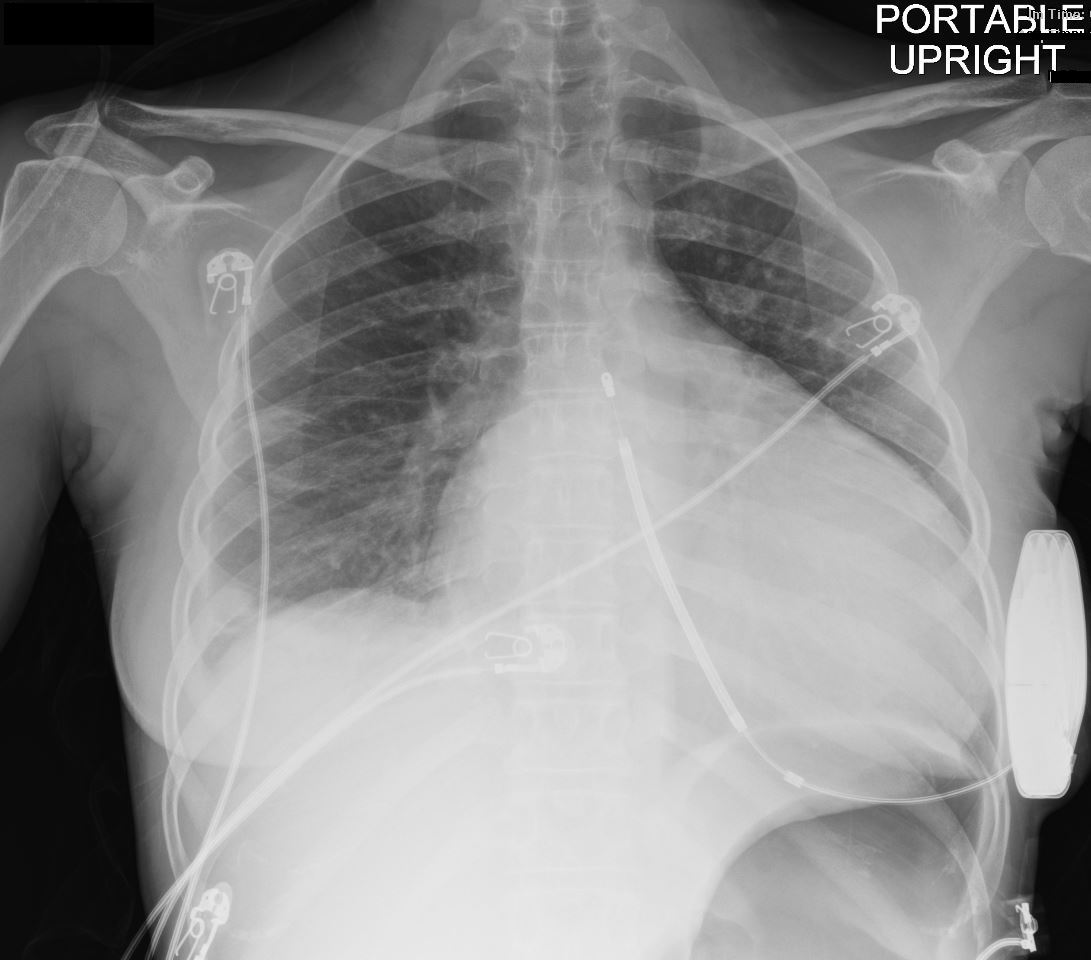
35-year-old female with a 8 year history of post- partum cardiomyopathy presents with of chest pain. Frontal CXR shows global cardiomegaly, blunting of the right costophrenic angle with a suggestion of a subsegmental infiltrate in the right costophrenic angle, and a region of linear atelectasis in the right mid lung field. A small loculated right effusion is present. An external defibrillator is noted. No definite CHF
Ashley Davidoff MD TheCommonVein.net 258Lu 136164

35-year-old female with an 8-year history of post- partum cardiomyopathy presents with a history of chest pain. CT of chest with contrast in an axial projection, at the level of the heart, shows an enlarged left ventricle. The right lower lobe segmental arteries show filling defects and absence of contrast compared to the left lower lobe arteries. An external defibrillator is present.
Ashley Davidoff MD TheCommonVein.net 258Lu 136165
Leadless Pacemaker
Case courtesy of Hilary Bowman, Radiopaedia.org, rID: 85742
Case courtesy of Hilary Bowman, Radiopaedia.org, rID: 85742

Case courtesy of Hilary Bowman, Radiopaedia.org, rID: 85742
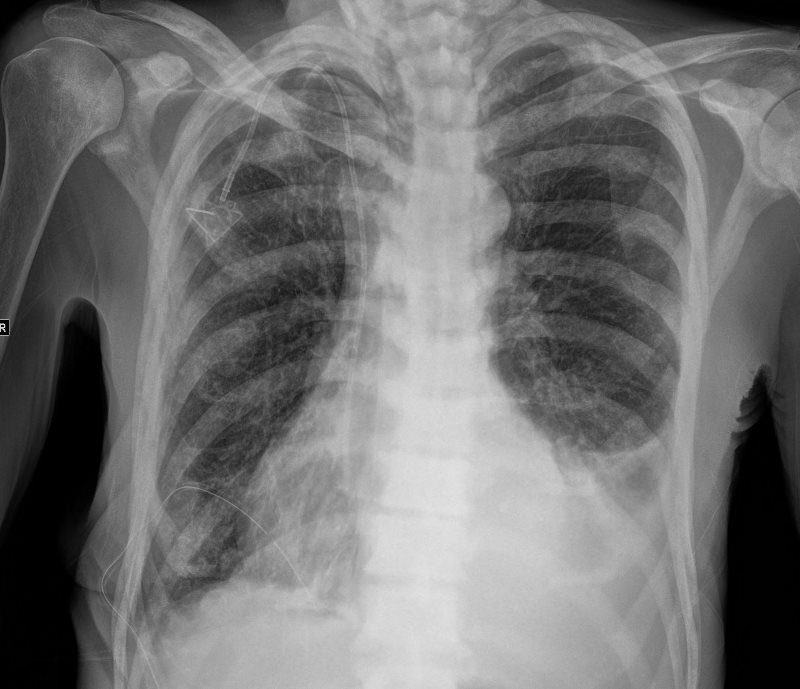
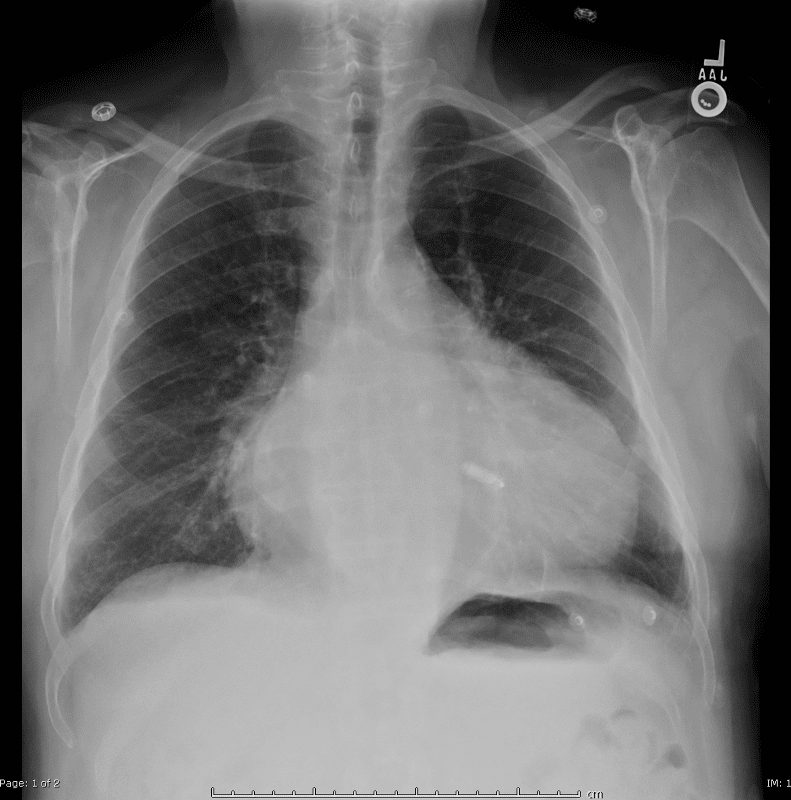
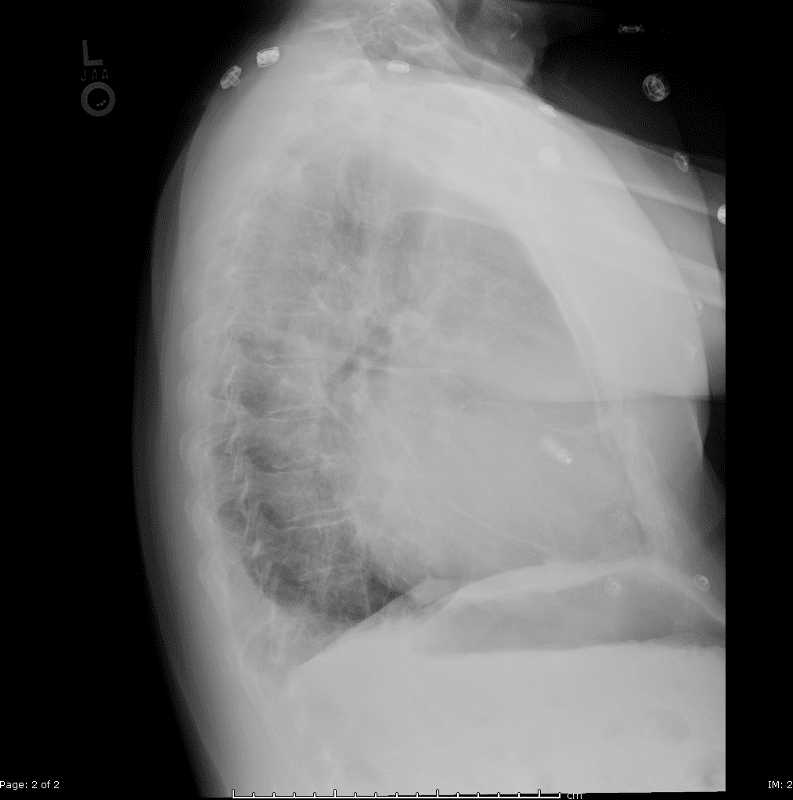
Loop recorder
75-year-old man on blood thinners s/p aortic valve replacement s/p trauma, presents with hemoptysis. He was afebrile and without an elevated white count
A loop recorder is noted overlying the left upper chest.
Ashley Davidoff MD TheCommonVein.net 165Lu 135849
Atrial Appendage Hardware
Watchman Device
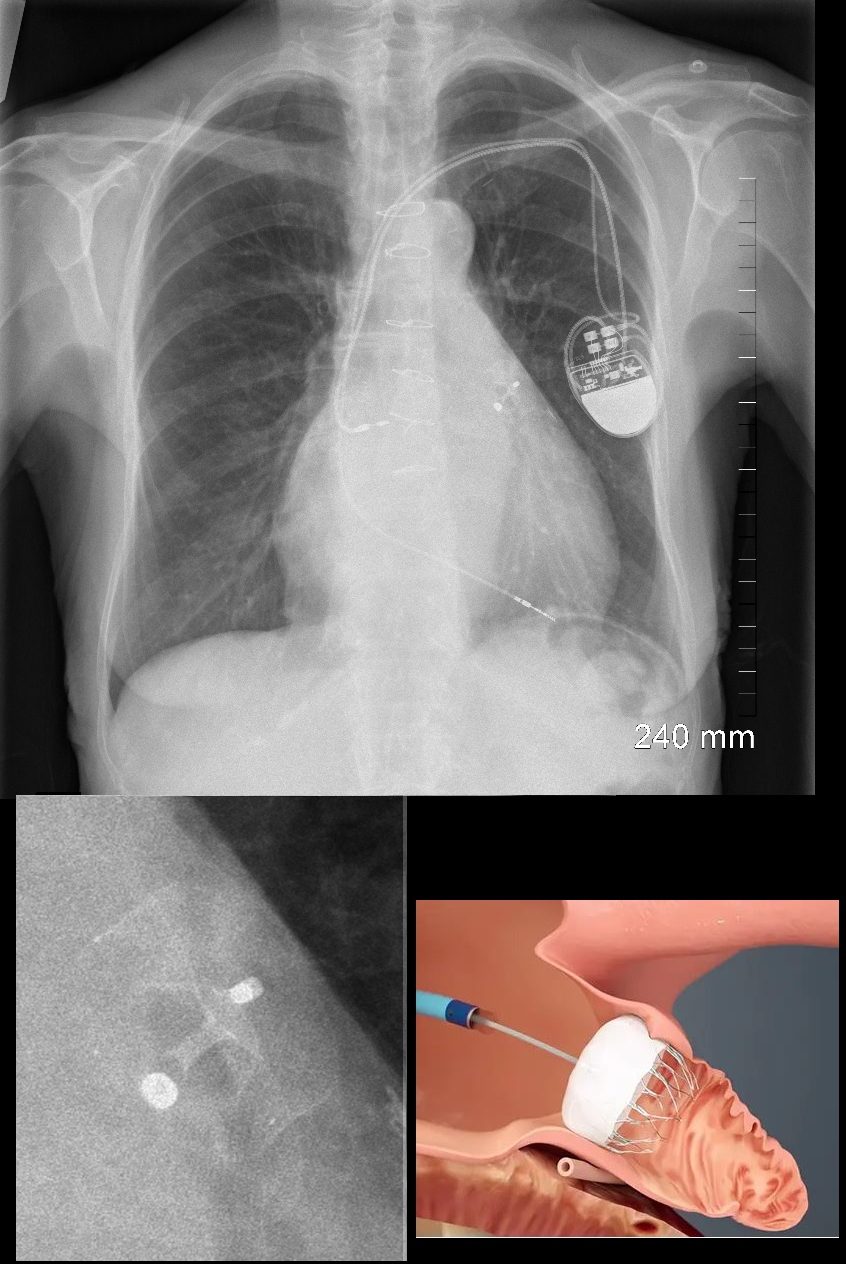
Xray – Case courtesy of Dr Aneta Kecler-Pietrzyk, Radiopaedia.org, rID: 52875
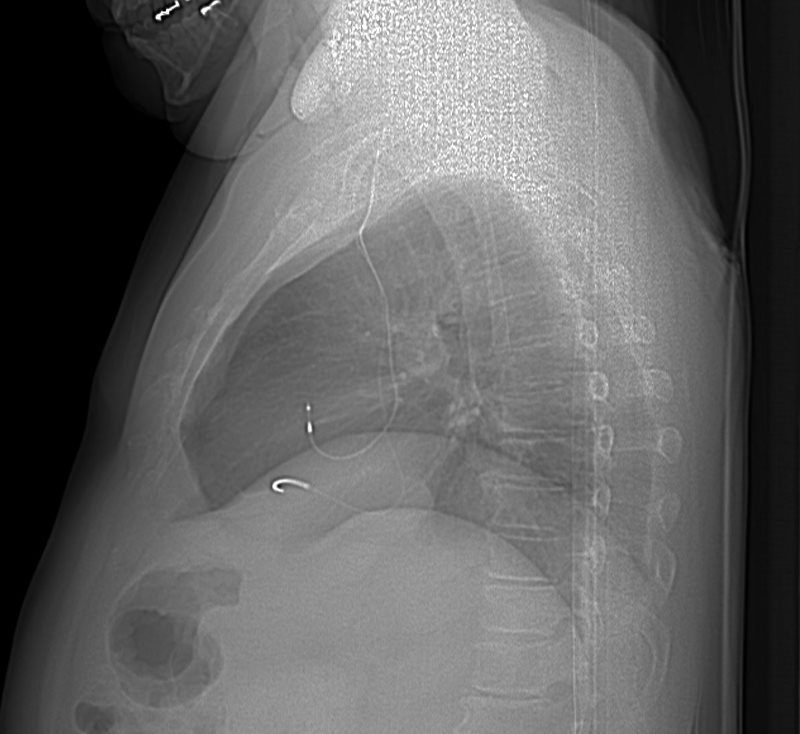
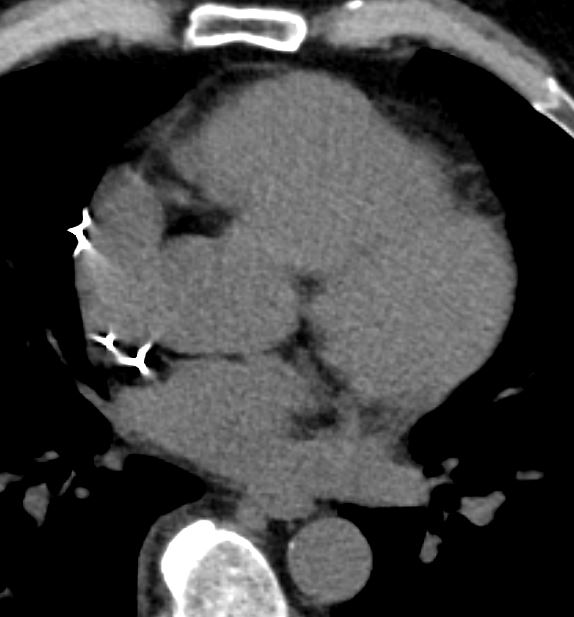
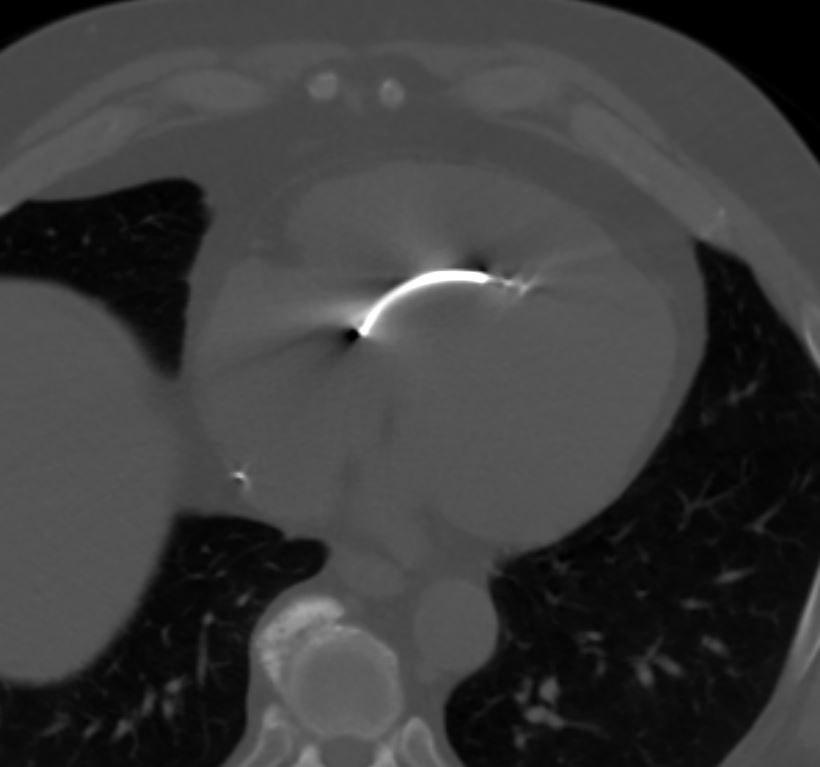
AtriClip
Resembles a hair pin
Case courtesy of Dr Aneta Kecler-Pietrzyk, Radiopaedia.org, rID: 52156
Courtesy Wellington ICU
Links and References
Jain S A pictorial essay: Radiology of lines and tubes in the intensive care unit Indian J Radiol Imaging. 2011 Jul-Sep; 21(3): 182–190.