50 y.o. male current smoker with a history of ESRD 2/2 renal artery stenosis on HD undergoing transplant evaluation, DM, HTN, CAD s/p CABG and Latent TB s/p 9 months INH with a 5.2 cm pleural-based desmoid tumor/fibromatosis of the L chest wal



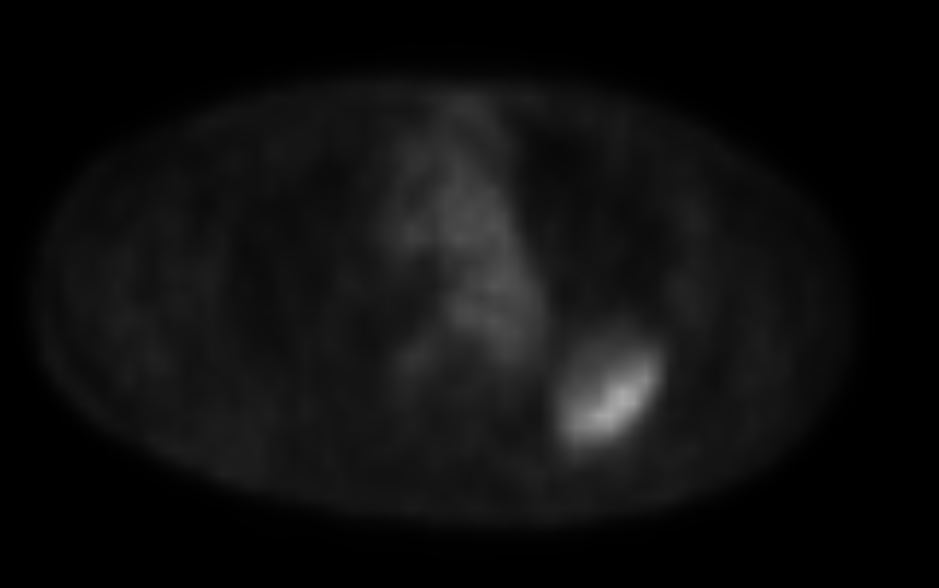
 PET CT
PET CT
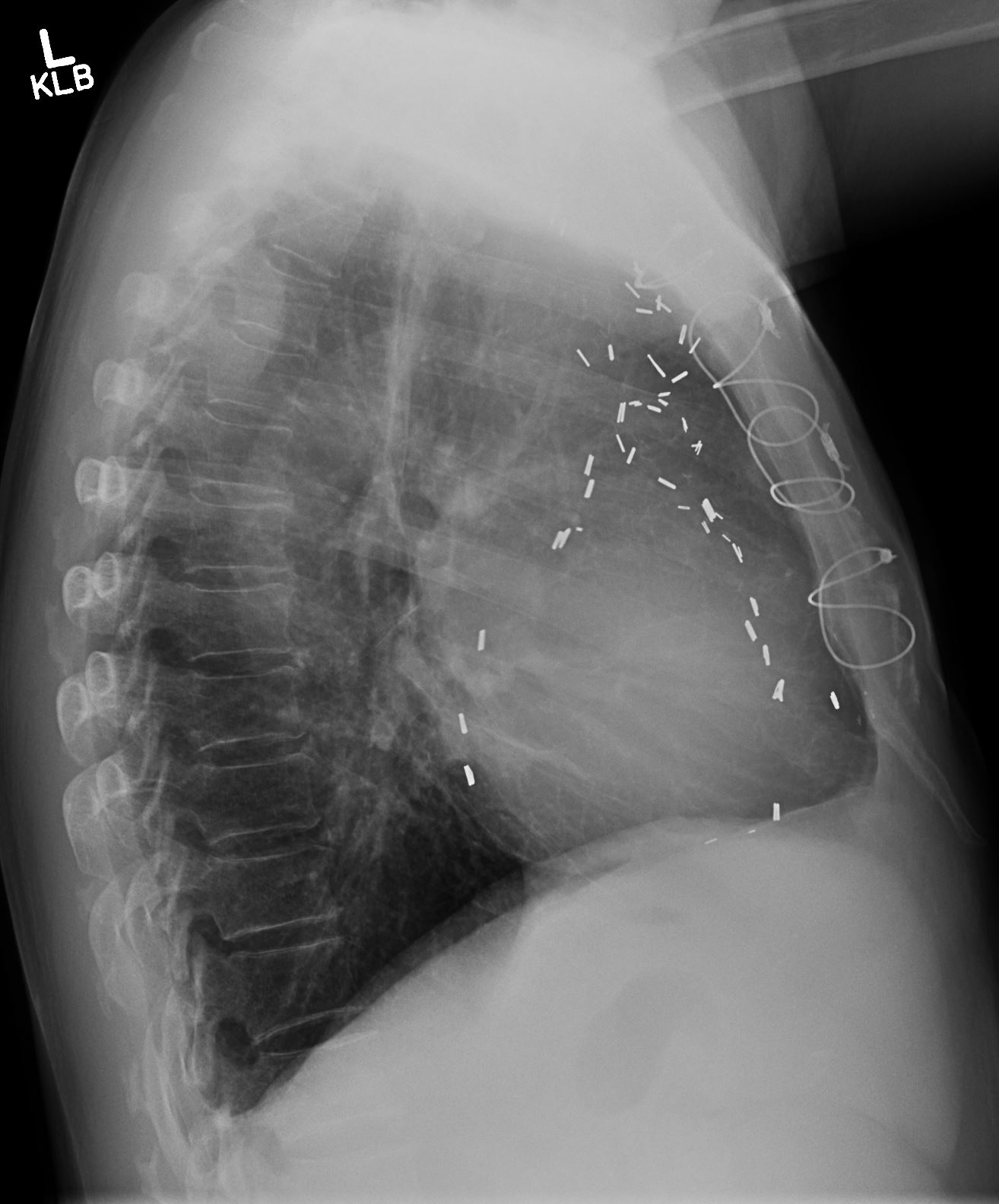
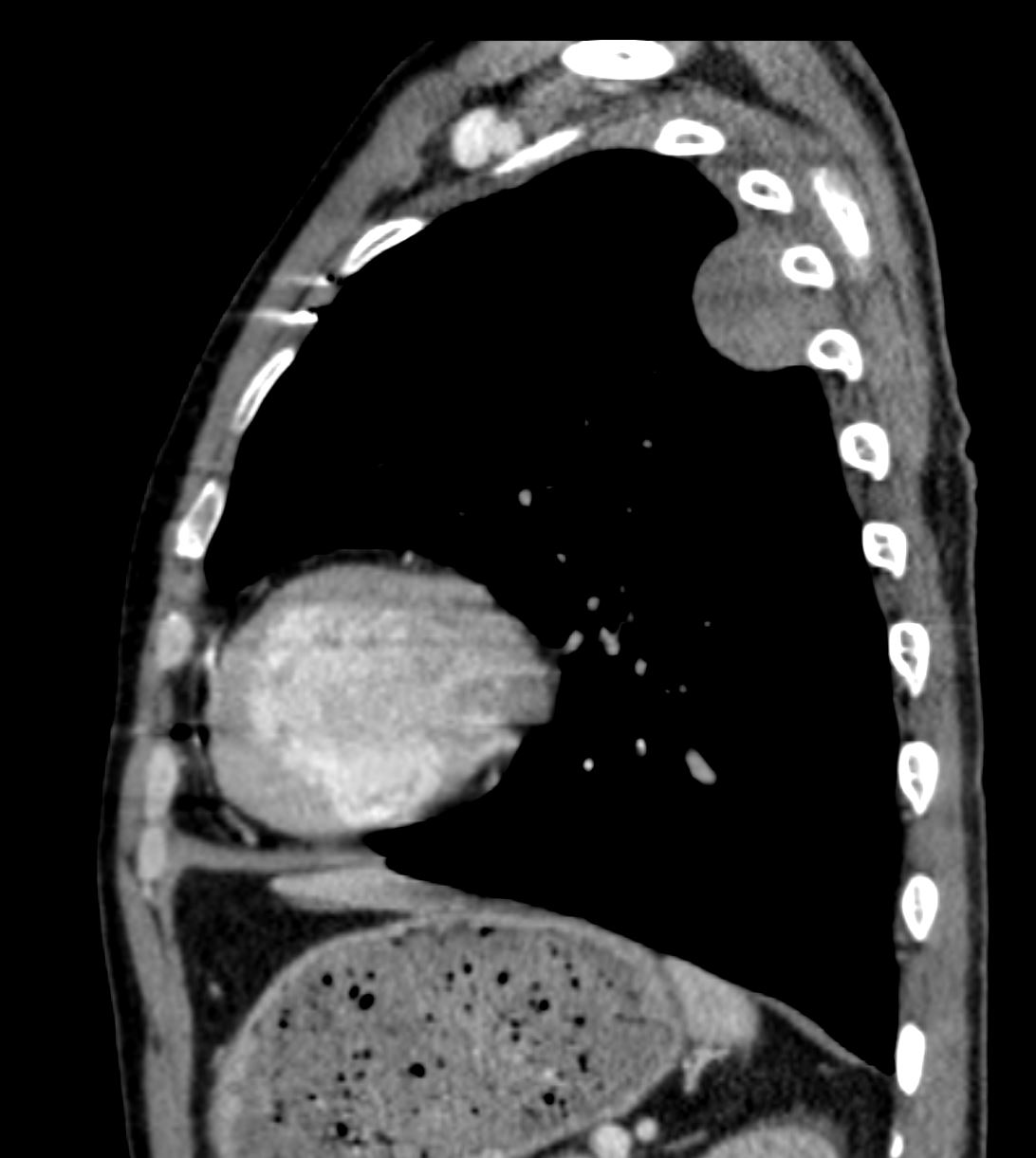
PET: There is a smoothly marginated pleural-based mass within the
left upper lobe which measures 3.9 x 5.5 cm in greatest axial
dimension with hypermetabolic activity along the posterolateral
aspect of the mass with SUV max of 5.5 with low level activity
elsewhere in the mass. This mass previously measured 2.8 x 4.2 cm 4 months prior
Interval growth hypermetabolic activity is most consistent with malignancy. There is approximately 5.5 cm of contact with the pleura. There evidence ofnvasion to the underlying rib 4th and 5th posterolateral ribs (no sclerosis or erosion). There are no additional areas of hypermetabolic activity to suggest local or distant metastasis. There is no hypermetabolic mediastinal or supraclavicular lymphadenopathy.
Positive margins on pathology resulted in XRT
CORE FRAGMENTS OF FIBROUS TISSUE WITH A VARIABLY PROMINENT POPULATION OF SPINDLE CELLS WITH BLAND HISTOLOGIC FEATURES MOST LIKELY REPRESENTING SUBMESOTHELIAL MESENCHYMAL CELLS.
AN IMMUNOHISTOCHEMICAL STUDY REVEALED POSITIVE STAINING OF THE SPINDLE CELLS FOR CALRETININ AND FOCALLY FOR MUSCLE SPECIFIC ACTIN. THE STAINS FOR CYTOKERATIN (AE1/3), D240, ALK-1, CD34 AND S-100 PROTEIN) ARE NEGATIVE.
NOTE: THE FINDINGS ARE MOST IN KEEPING WITH A REACTIVE/REPARATIVE PROCESS. THE DIFFERENTIAL DIAGNOSIS INCLUDES A CELLULAR PLEURAL PLAQUE OR FIBRO-HYALINE PLEURITIS. A DESMOPLASTIC MESOTHELIOMA IS IN THE DIFFERENTIAL DIAGNOSIS BUT APPEARS TO BE LESS
LIKELY.
The specimen consists of a well-circumscribed, firm mass measuring 7.5 x 4.5 x 2.5 cm with a tan-yellow,
fleshy, homogeneous cut surface. There are no areas of hemorrhage or necrosis.
SPINDLE CELL LESION.
THE TUMOR IS COMPOSED OF BLAND LOOKING CELLS GROWING IN FASCICLES WITH AREAS OF KELOID LIKE COLLAGEN. ADDITIONALLY, YOUR B-CATENIN STAIN DOES DEMONSTRATE SOME NUCLEAR STAINING. AS YOU KNOW FIBROMATOSIS IS A LOCALLY AGGRESSIVE TUMOR THAT CAN LOCALLY RECUR, ESPECIALLY IF THE RESECTION MARGIN IS POSITIVE AS APPEARS TO BE THE CASE WITH THIS TUMOR.
IMMUNOHISTOCHEMICAL STUDIES PERFORMED ON PARAFFIN EMBEDDED TISSUE (BLOCK 4) SHOWS POSITIVE STAINING FOR VIMENTIN AND B-CATENIN (FOCAL NUCLEAR STAINING NOTED) AND NEGATIVE STAINING FOR CYTOKERATIN AE1/AE3, DESMIN, MSA, S-100, BCL-2 AND CD34. THESE
FINDINGS SUPPORT THE ABOVE DIAGNOSIS.
This case was seen as a consult by Dr. Peter Nielsen at Massachusetts General Hospital, Pathology department and assigned their number NCS-1863.
Immunohistochemistry Disclaimer:
These tests were developed and their performance characteristics determined by the manufacturer. They have not been cleared or approved by the U.S. Food and Drug Administration, however, the FDA has determined that such clearance or approval is not
necessary. The tests were used for clinical purposes and should not be regarded as investigative or for research.
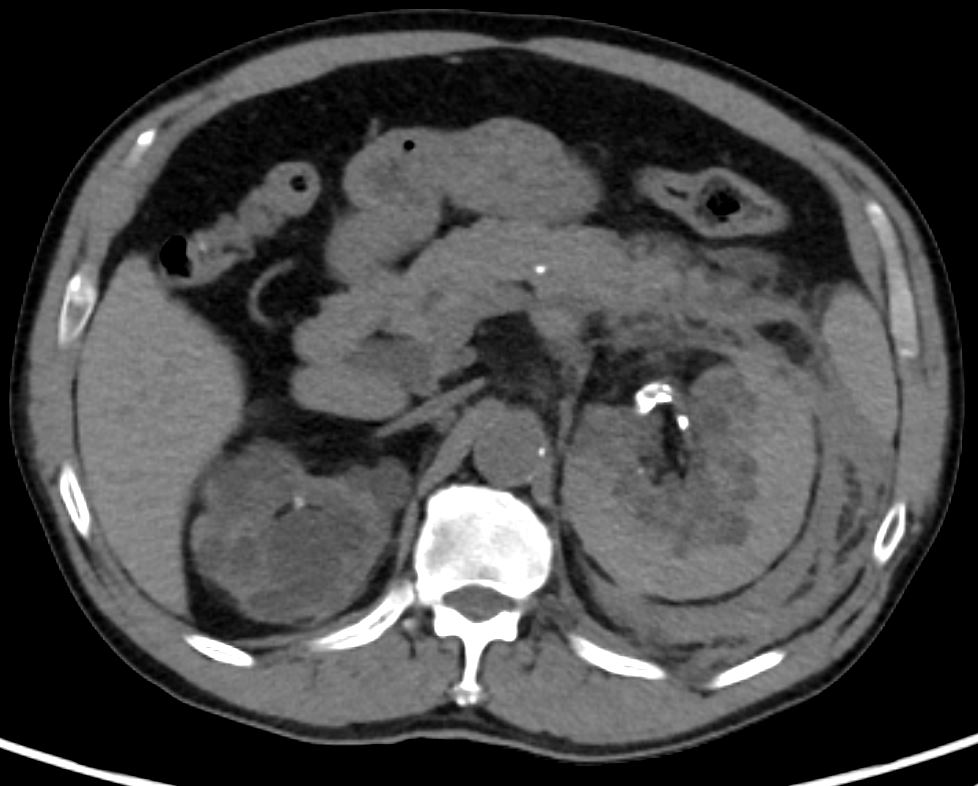
CT 6 ys later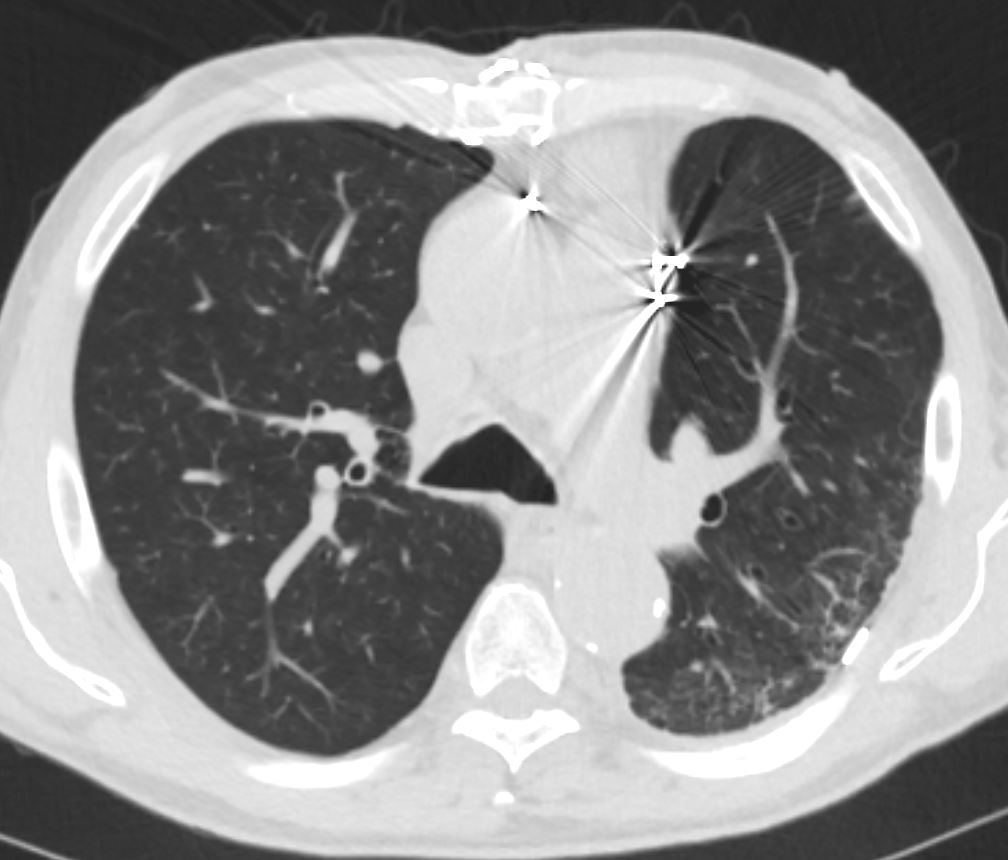
Also has acquired polycystic kidney disease with spontaneous bilateral subcapsular hematomas