
- is an obstructive lung disease
- Caused by
- infection
- pneumonia
- TB aspergillosis
- smoking
- radiation therapy
- cystic fibrosis
- immune disease
- autoimmune
- HIV/AIDS
- Resulting in
- permanent enlargement of parts of the airways
- Caused by
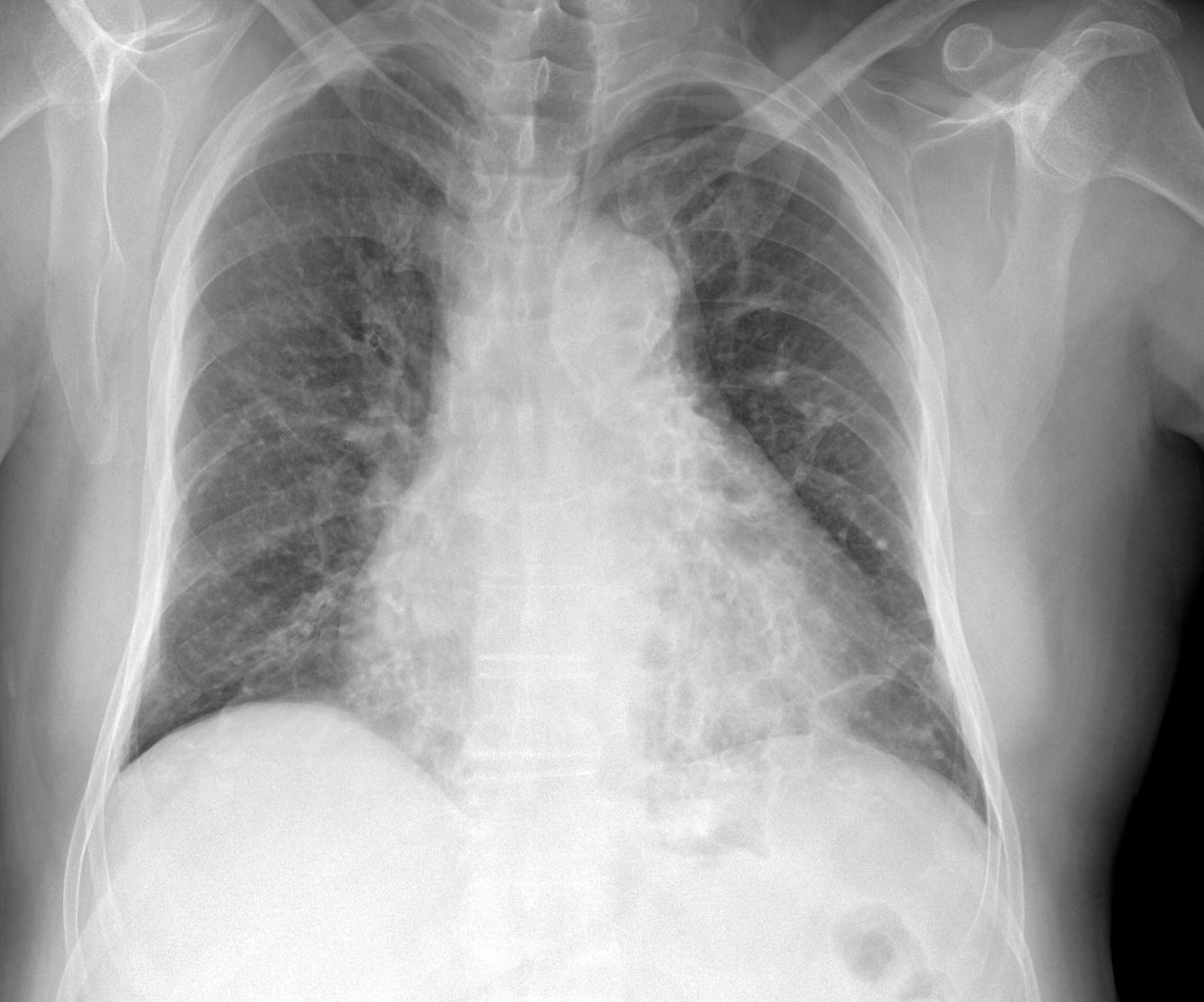
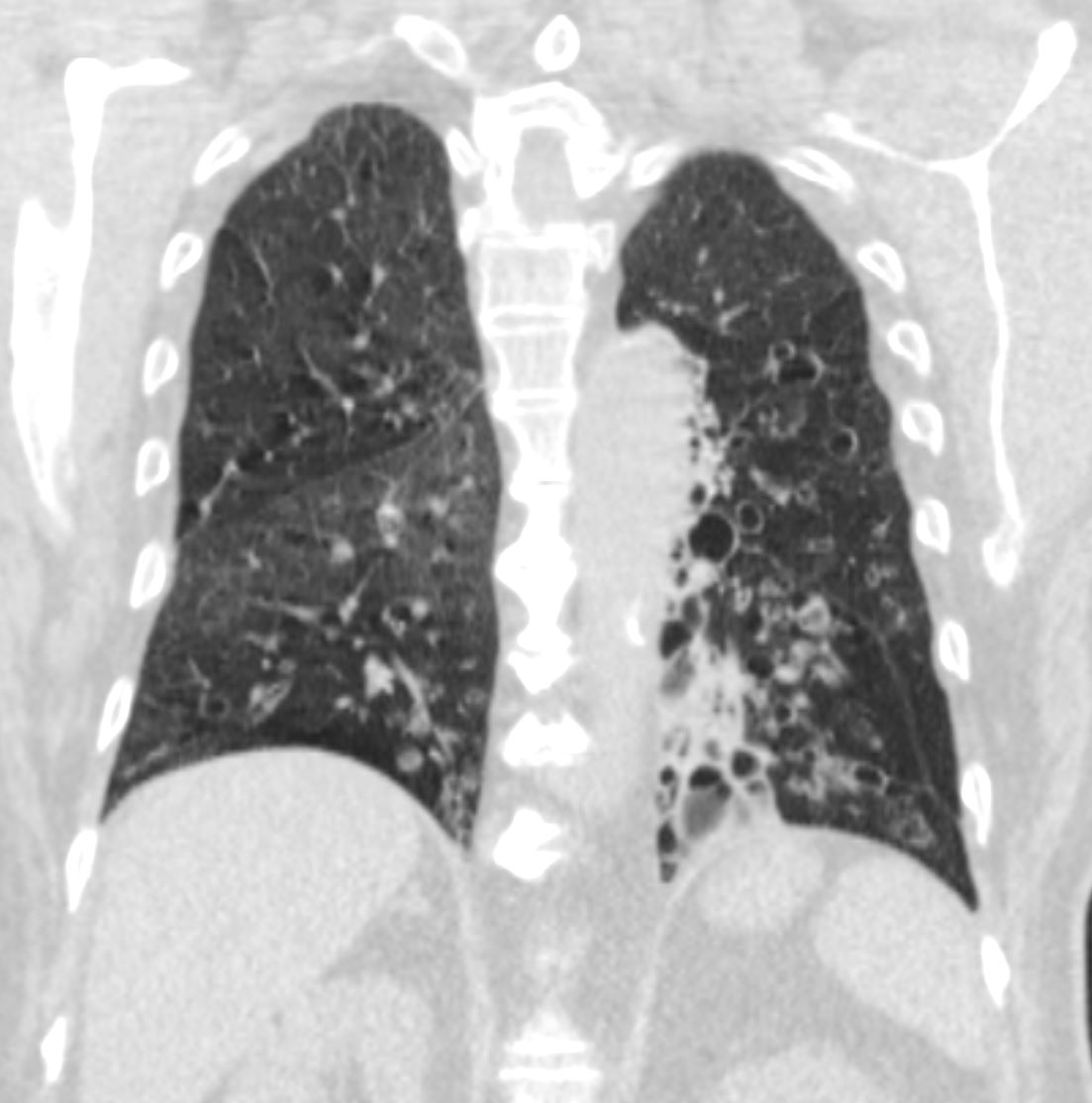
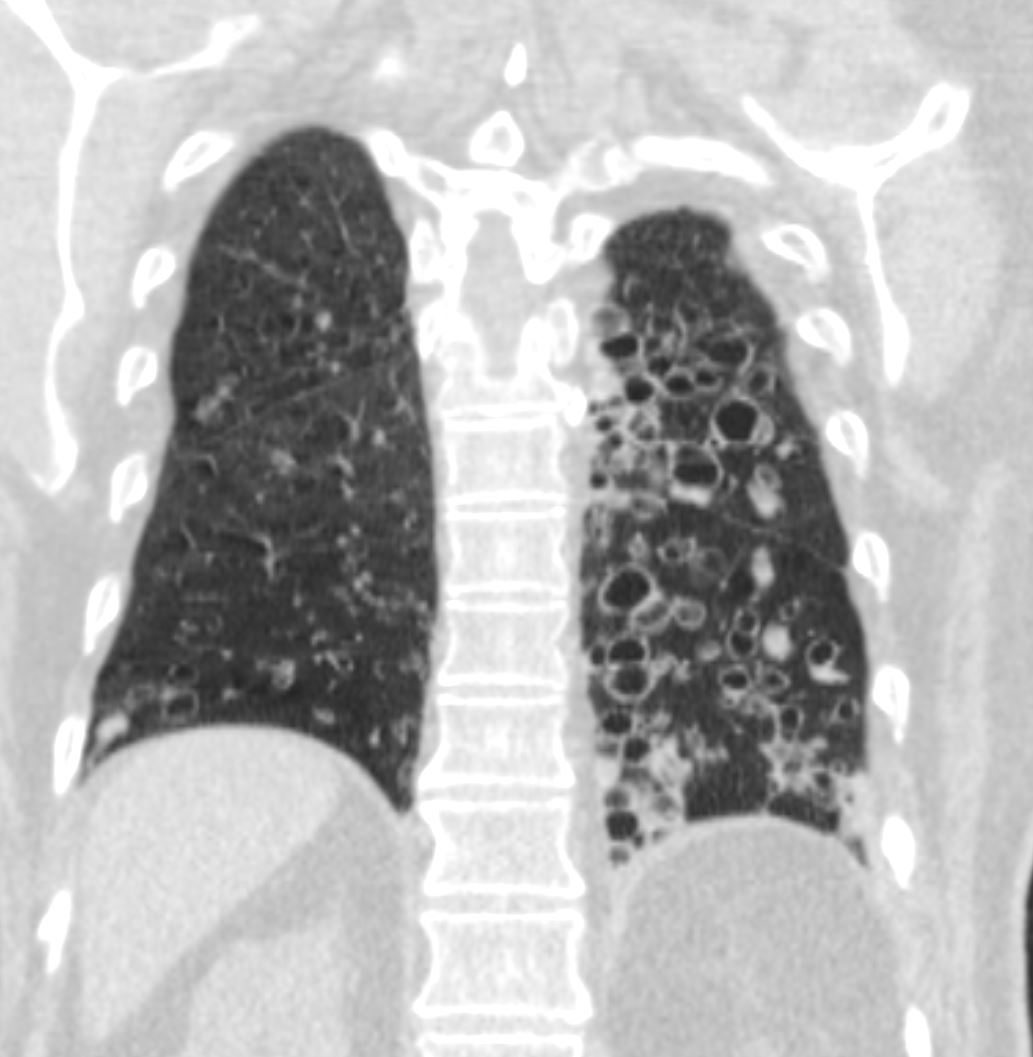
Apical Bronchiectasis – Possibly TB

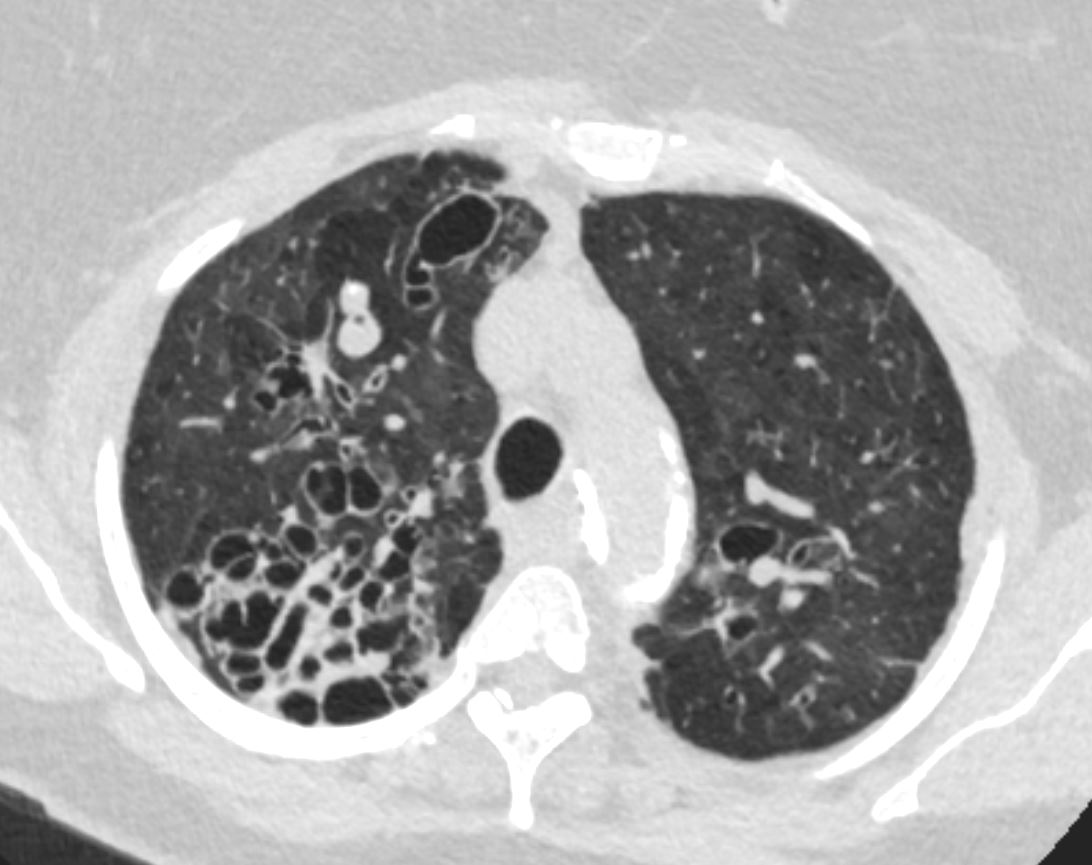
CT scan through the apex of the lungs of a 100 year old female showing evidence of bilateral apical bronchiectasis (top) with correlative plain film findings in the plain film (below) The most common cause is TB. The MPA is enlarged consistent with the diagnosis of pulmonary hypertension.
Ashley Davidoff MD
- Emphysema
- Smoking and Bronchiectasis –
-
- Loss of ciliary function by cigarette smoke
- Increase mucus production with decrease clearing
- Increase infection
-
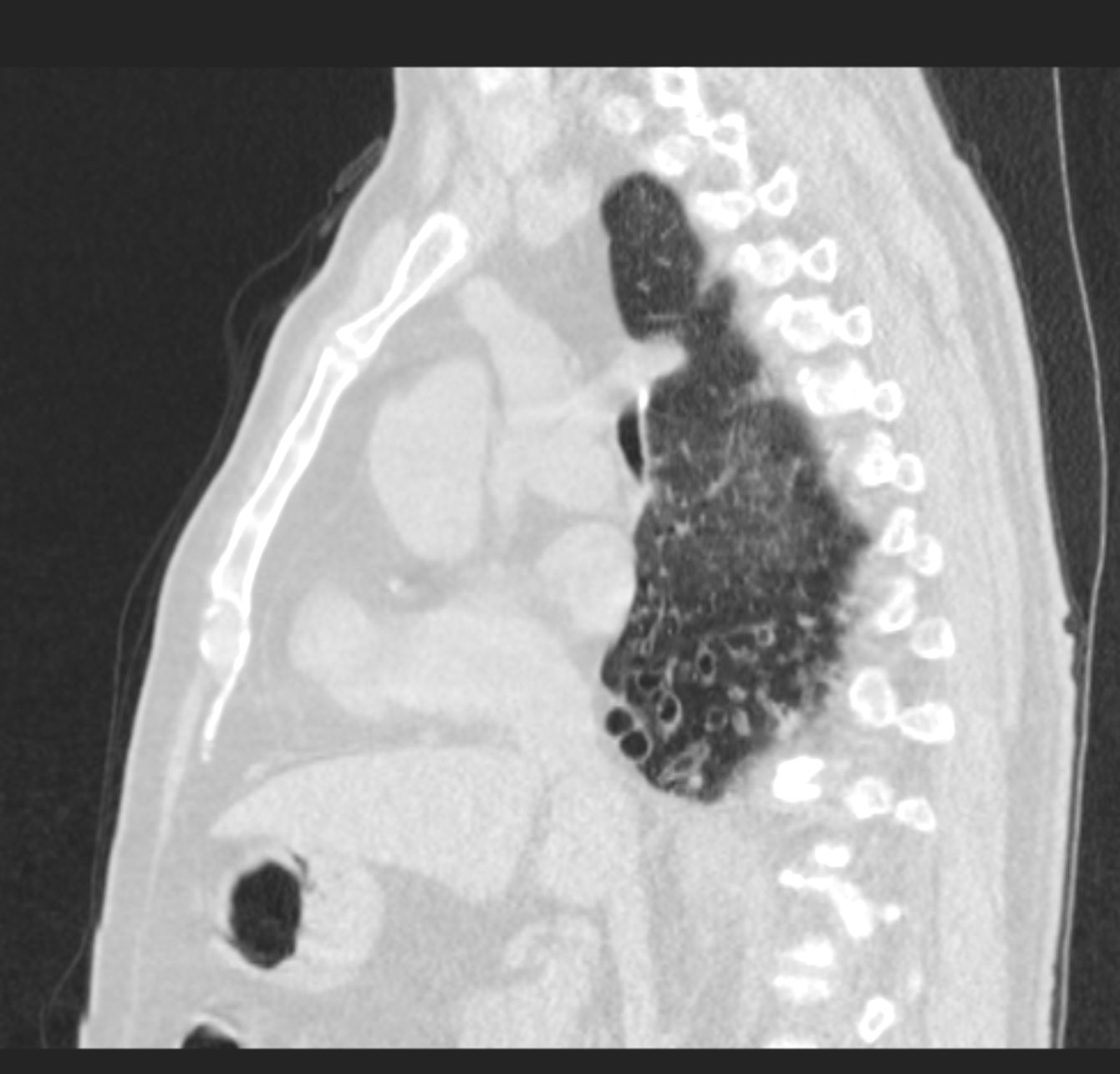
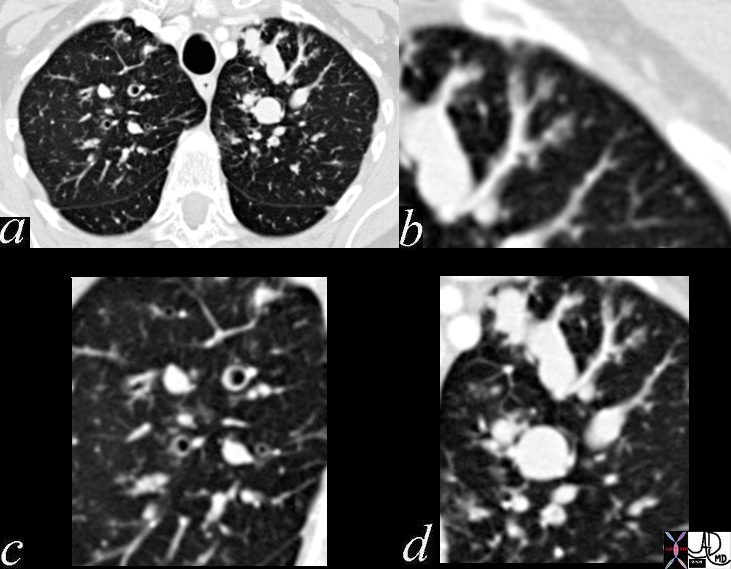
Saccular Bronchiectasis

Ashley Davidoff MD TheCommonVein Bronchiectasis 001
Ashley Davidoff
TheCommonVein.net

Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net

Ashley Davidoff
TheCommonVein.net
Mucus Filled airway with Distal Hyperinflation

Ashley Davidoff MD TheCommonVein.net bronchiectasis 006b
Ashley Davidoff MD TheCommonVein.net bronchiectasis 005
Ashley Davidoff MD TheCommonVein.net bronchiectasis 006
Bronchiectasis and Atelectasis
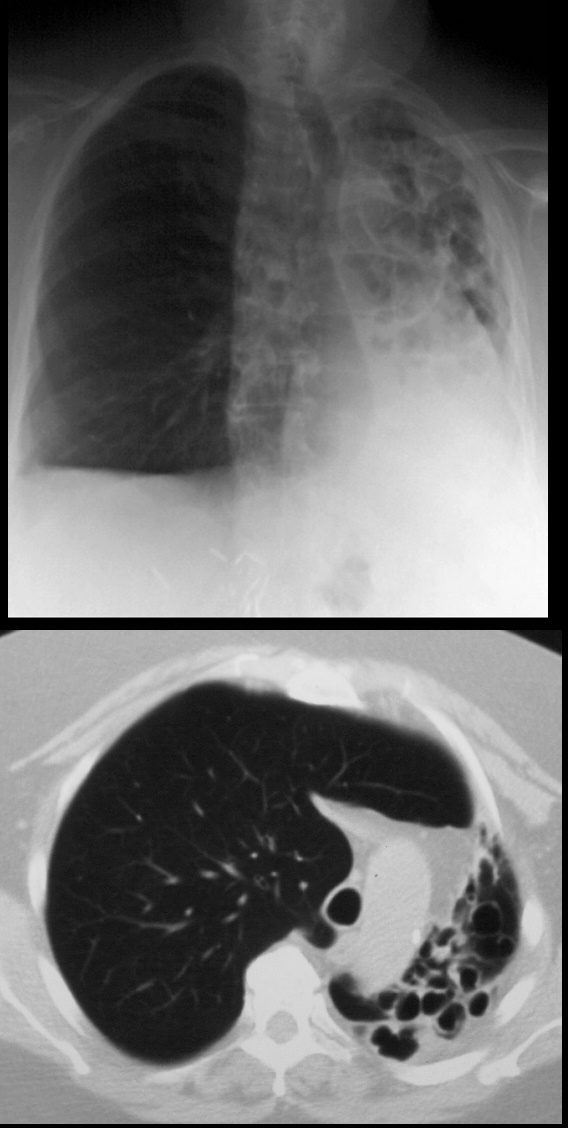
68year old male presents with chronic cough. Chest Xray reveals evidence of tram tracking and bronchiectasis in the left lung with volume loss of the entire right lung with secondary hyperinflation of the right lung, and mediastinal shift. CT scan shows severe volume loss and hyperinflation of the right lung.
Ashley Davidoff MD TheCommonVein.net
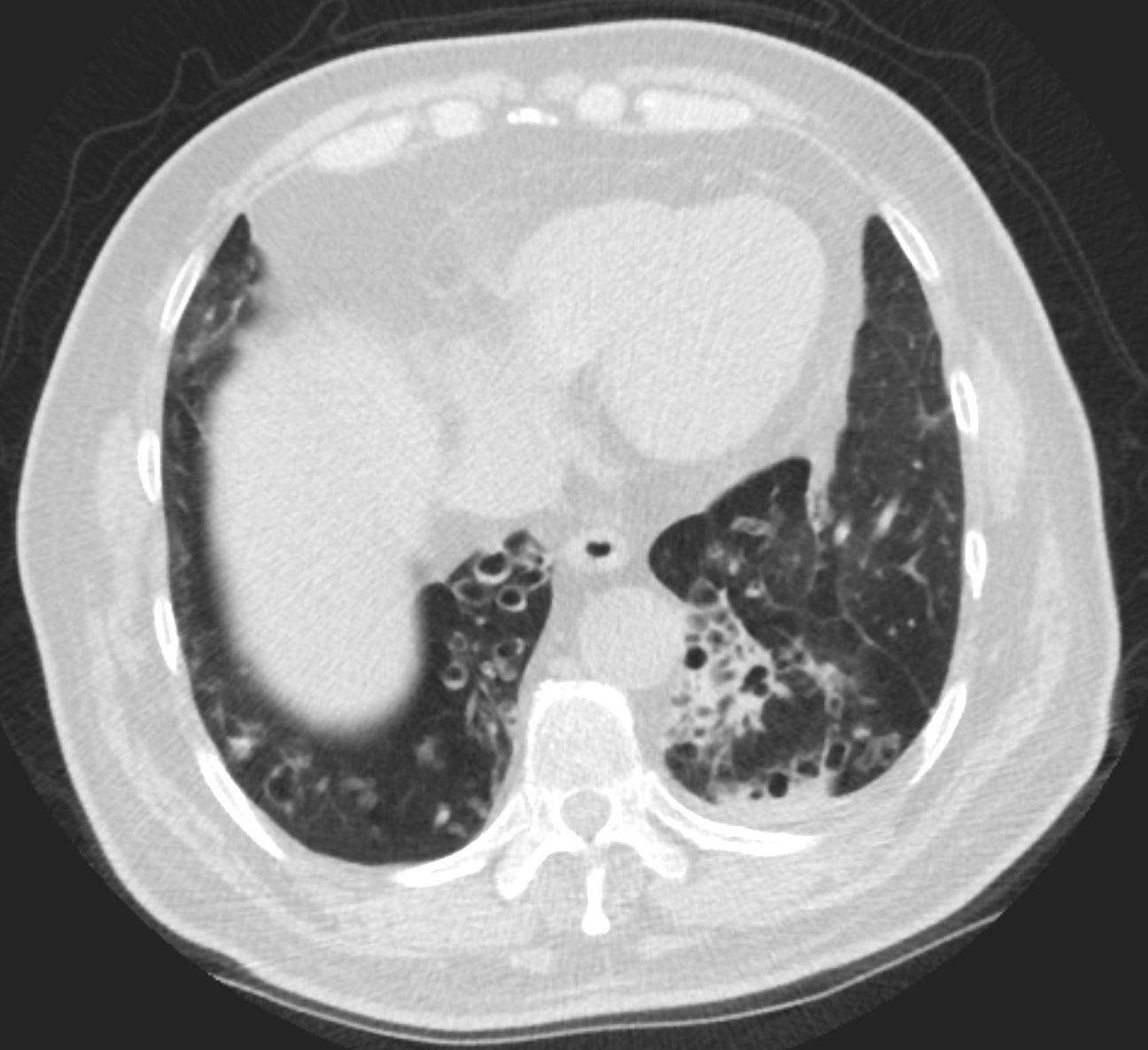
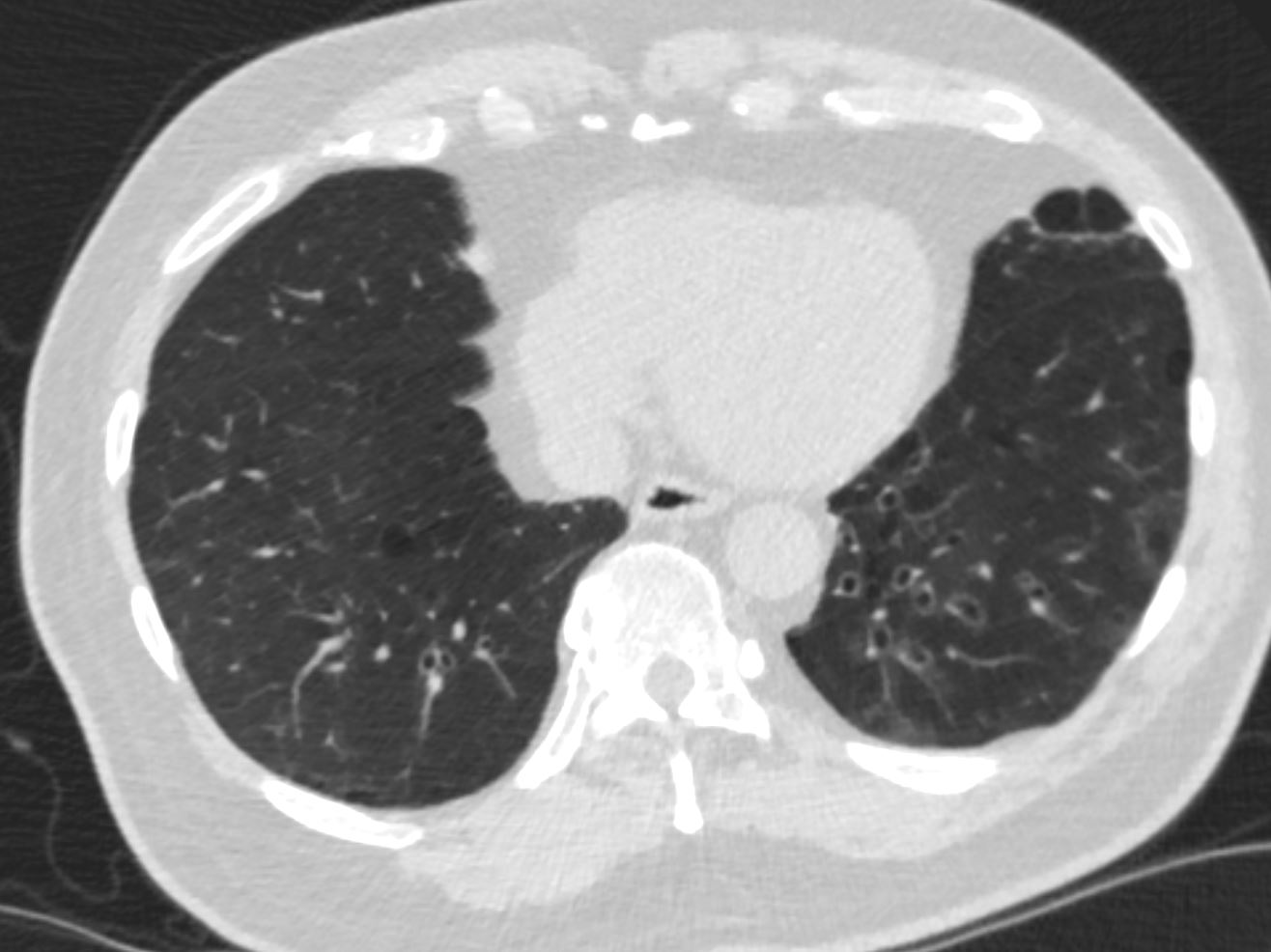
CT scan through the chest shows medium sized bronchi, bronchioles and small airways impacted with fluid. This collage is presented to reveal tree in bud changes resulting from impaction in the smaller terminal bronchioles and respiratory units. The tree-in-bud pattern also results in small centrilobular nodules connected to multiple branching linear structures of similar caliber from a single stalk. Originally it was felt to result from endobronchial spread of Mycobacterium tuberculosis, but is is now recognized in diverse entities including peripheral airway diseases caused by infection (bacterial, fungal, viral, or parasitic), congenital disorders, idiopathic disorders (obliterative bronchiolitis, pan bronchiolitis), aspiration or inhalation of foreign substances, immunologic disorders, connective tissue disorders and peripheral pulmonary vascular diseases such as neoplastic pulmonary emboli.
In this case there are also dilated medium sized airways, impacted with soft tissue characteristic of the finger in glove sign and most likely due to allergic bronchopulmonary aspergillosis (ABPA)
Ashley Davidoff MD Ashley Davidoff MD TheCommonVein.net
47113c01
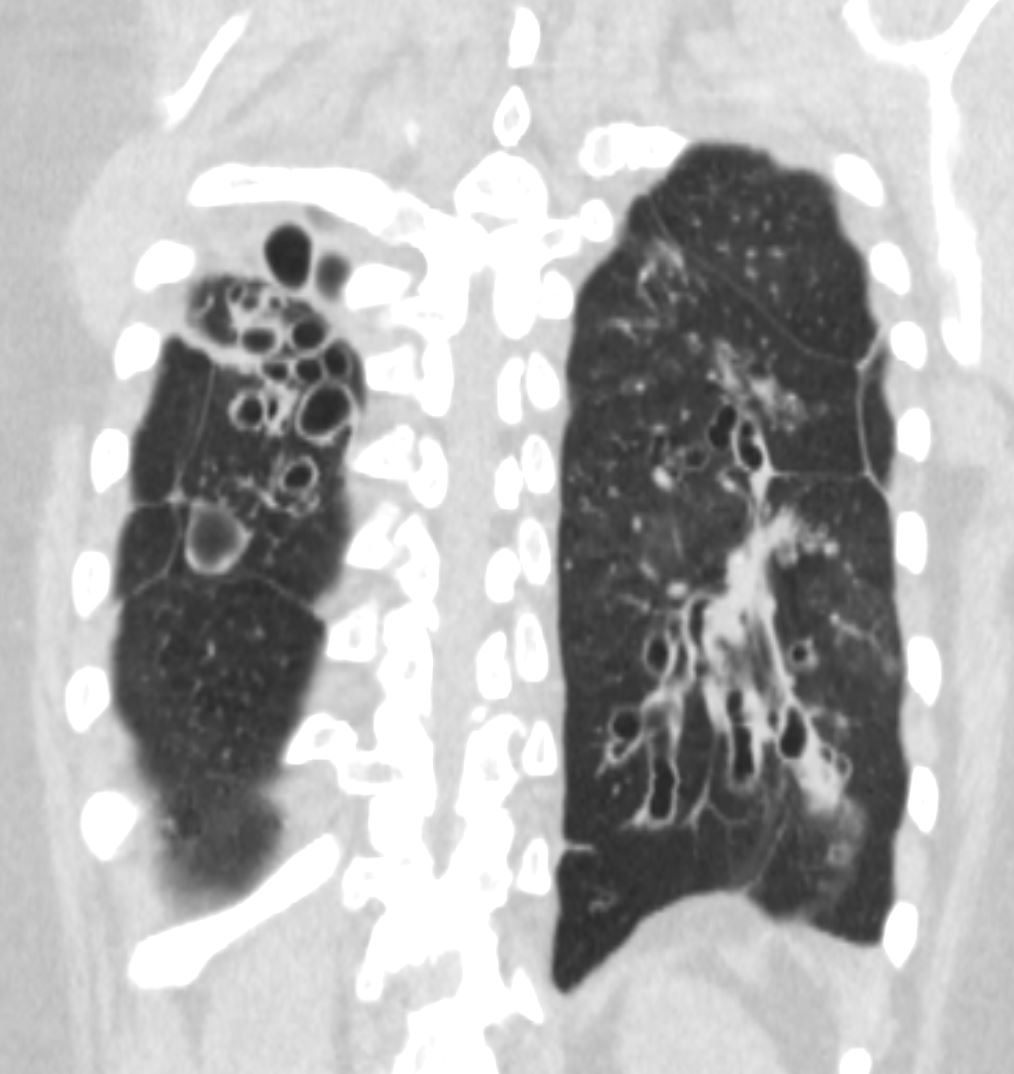
Compare the two Sides
Compare the 2 bases
Ashley Davidoff MD TheCommonVein.net
Links and References
Milliron B, et al Bronchiectasis: Mechanisms and Imaging Clues of Associated Common and Uncommon Diseases RadioGraphicsVol. 35, No. 4 2015
- TCV
- Bronchiectasis
- 032Lu Bronchiectasis and Emphysema
- 034Lu Basal Bronchitis Bronchiectasis Young Female
- 044Lu Chronic Inactive TB Lymphatic Distribution
- 003MC Kartagener’s and Bronchiectasis
- 054 LU Right Middle Lobe Syndrome – Bronchiectasis probable TB
- 063LU Sarcoidosis and Bronchiectasis
- 72LU TB and Bronchiectasis
- 73Lu TB Bronchiectasis
- Bronchiectasis
Kartagener’s syndrome TCV page
Fleischner Society
Pathology.—Bronchiectasis is irreversible localized or diffuse bronchial dilatation, usually resulting from chronic infection, proximal airway obstruction, or congenital bronchial abnormality (,26). (See also traction bronchiectasis.)
Radiographs and CT scans.—Morphologic criteria on thin-section CT scans include bronchial dilatation with respect to the accompanying pulmonary artery (signet ring sign), lack of tapering of bronchi, and identification of bronchi within 1 cm of the pleural surface (,27) (,Fig 11). Bronchiectasis may be classified as cylindric, varicose, or cystic, depending on the appearance of the affected bronchi. It is often accompanied by bronchial wall thickening, mucoid impaction, and small-airways abnormalities (,27–,29). (See also signet ring sign.)