
Infection and Inflammation
Another Case of Extensive Segmental Subsegmental and Small Airway Disease with Centrilobular Nodules
Ashley Davidoff MD TheCommonVein.net
lungs airways segmental subsegmental small airway disease micronodules
Ashley Davidoff MD
TheCommonVein.net
lungs airways segmental subsegmental small airway disease micronodules
Ashley Davidoff MD
TheCommonVein.net
lungs airways segmental subsegmental small airway disease micronodules
Ashley Davidoff MD
TheCommonVein.net

lungs airways segmental subsegmental small airway disease micronodules
Ashley Davidoff MD TheCommonVein.net
RSV Pneumonia

Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
Cytomegalovirus Pneumonia
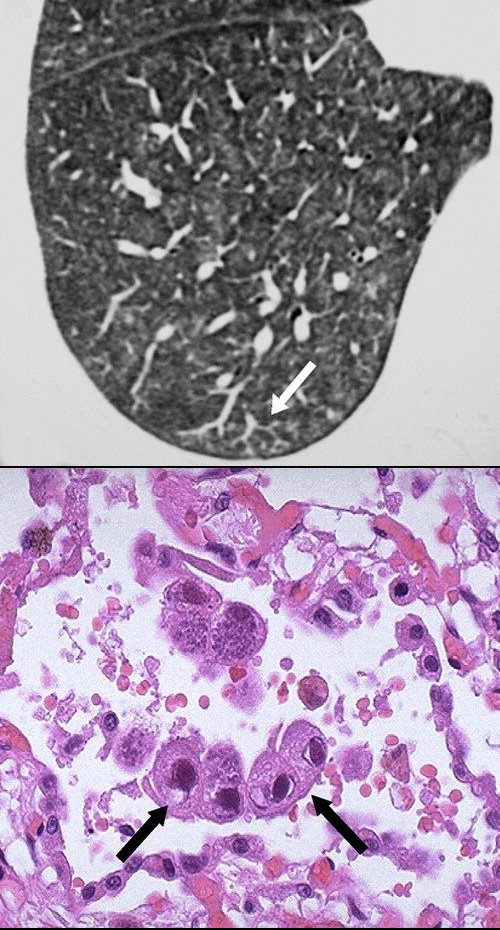
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
H influenzae Pneumonia
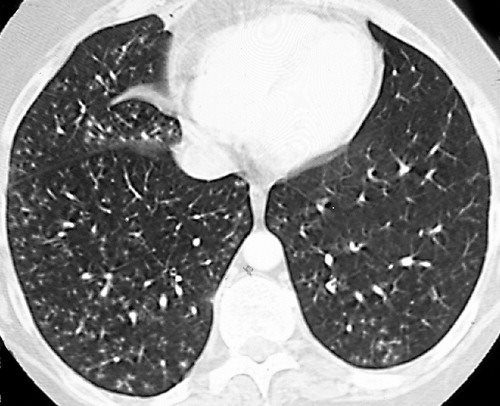
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
Staph Aureus
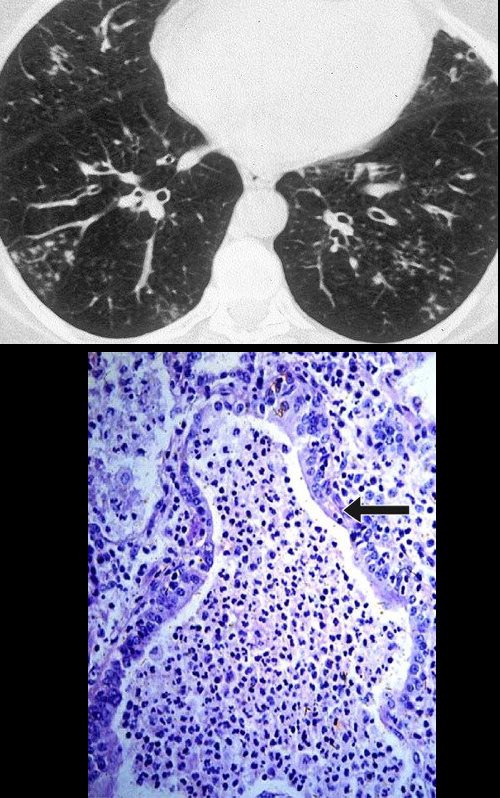
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
TB
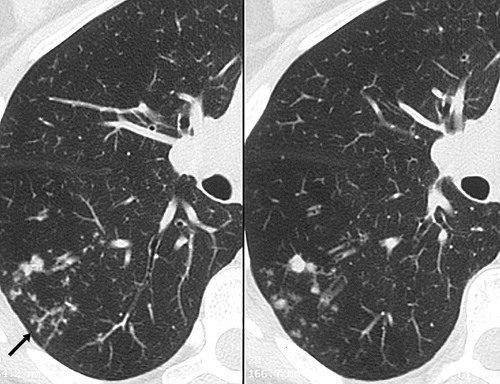
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Burgel, P-R et al Small airways diseases, excluding asthma and COPD: an overview European Respiratory Review 2013 22: 131-147; figs only web lungs 368

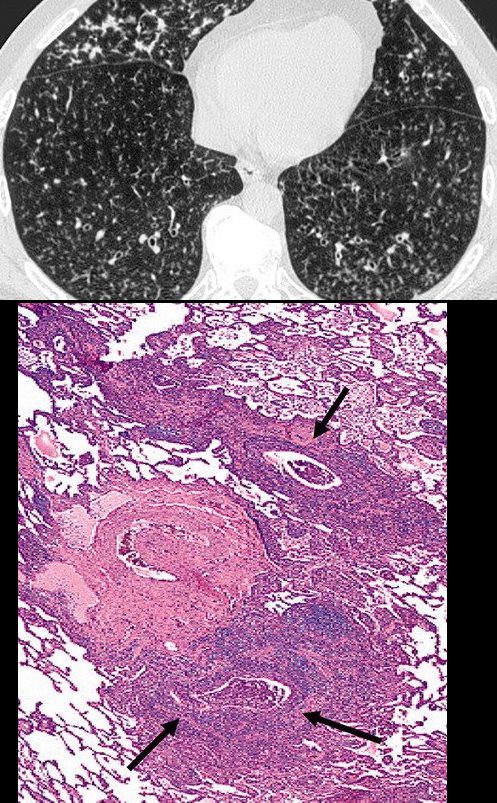
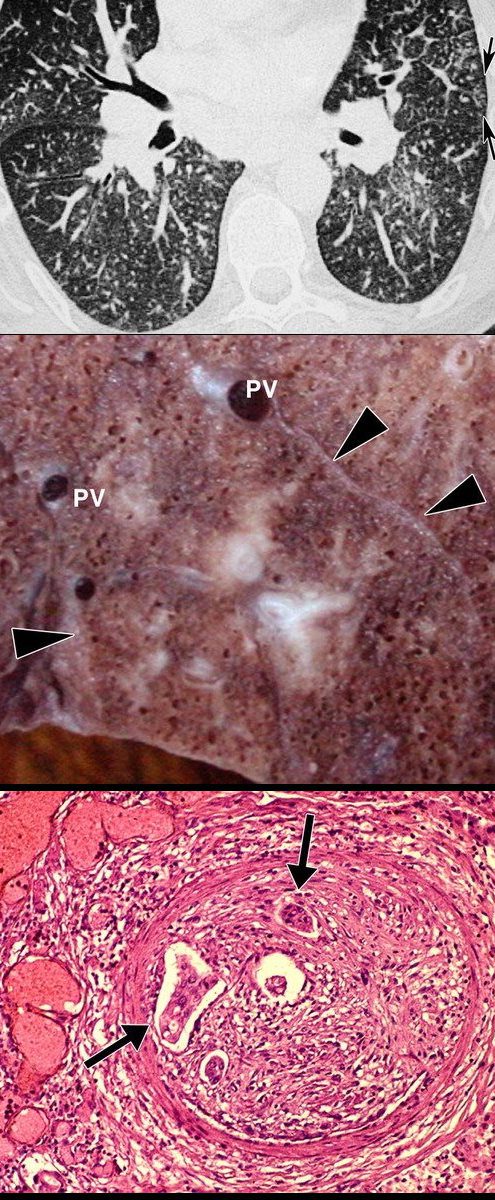
INACTIVE SECONDARY TB WITH EXTENSIVE PARENCHYMAL AND LYMPHOVASCULAR INVOLVEMENT
48-year-old male with history of TB presents with back pain
AP view of the spine shows complex lesion in the right apex characterized by fibronodular opacities. There are scattered calcifications throughout the lungs but some are centered around the lymphatics, including the interlobular septa and centrilobular region
Ashley Davidoff MD TheCommonVein.net
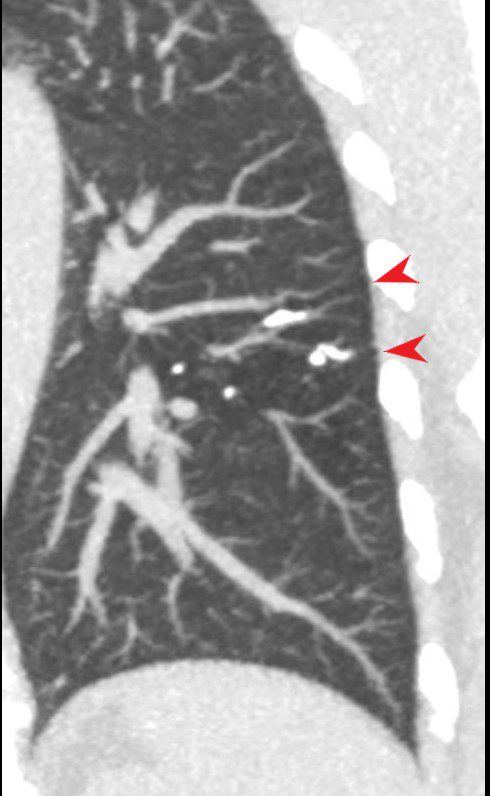
CALCIFICATION ALONG LYMPHOVASCULAR BUNDLES (red arrows)
INACTIVE SECONDARY TB WITH EXTENSIVE PARENCHYMAL AND LYMPHOVASCULAR INVOLVEMENT
48-year-old male with history of TB presents with back pain
AP view of the spine shows complex lesion in the right apex characterized by fibronodular opacities. There are scattered calcifications throughout the lungs but some are centered around the lymphatics, including the interlobular septa and centrilobular region
Ashley Davidoff MD TheCommonVein.net

INACTIVE SECONDARY TB WITH EXTENSIVE PARENCHYMAL AND LYMPHOVASCULAR INVOLVEMENT
48-year-old male with history of TB presents with back pain
AP view of the spine shows complex lesion in the right apex characterized by fibronodular opacities. There are scattered calcifications throughout the lungs but some are centered around the lymphatics, including the interlobular septa and centrilobular region
Ashley Davidoff MD TheCommonVein.net
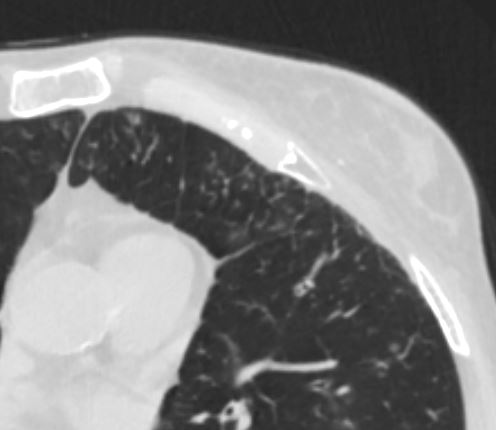
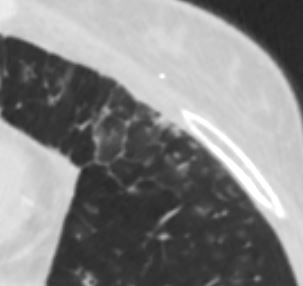
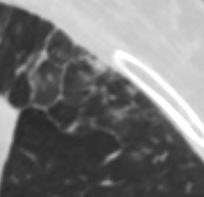
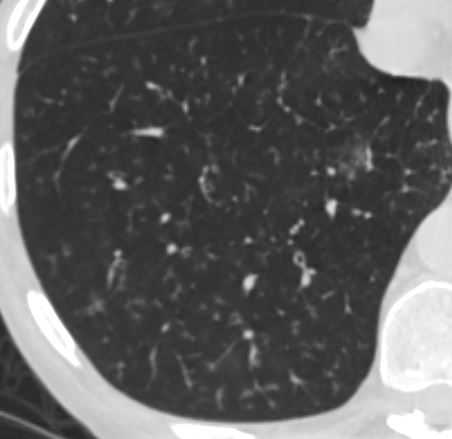
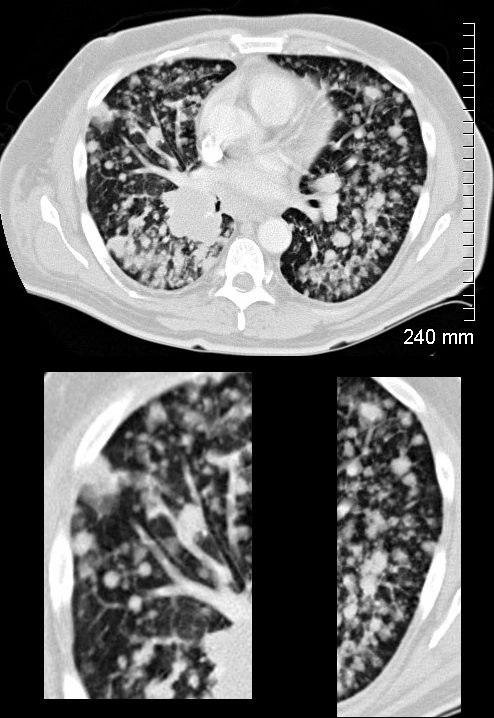
Aspergillosis
CT scan through the chest shows medium sized bronchi, bronchioles and small airways impacted with fluid. This collage is presented to reveal tree in bud changes resulting from impaction in the smaller terminal bronchioles and respiratory units. The tree-in-bud pattern also results in small centrilobular nodules connected to multiple branching linear structures of similar caliber from a single stalk. Originally it was felt to result from endobronchial spread of Mycobacterium tuberculosis, but is is now recognized in diverse entities including peripheral airway diseases caused by infection (bacterial, fungal, viral, or parasitic), congenital disorders, idiopathic disorders (obliterative bronchiolitis, pan bronchiolitis), aspiration or inhalation of foreign substances, immunologic disorders, connective tissue disorders and peripheral pulmonary vascular diseases such as neoplastic pulmonary emboli.
In this case there are also dilated medium sized airways, impacted with soft tissue characteristic of the finger in glove sign and most likely due to allergic bronchopulmonary aspergillosis (ABPA)
Ashley Davidoff MD Ashley Davidoff MD TheCommonVein.net
47113c01
Sarcoidosis

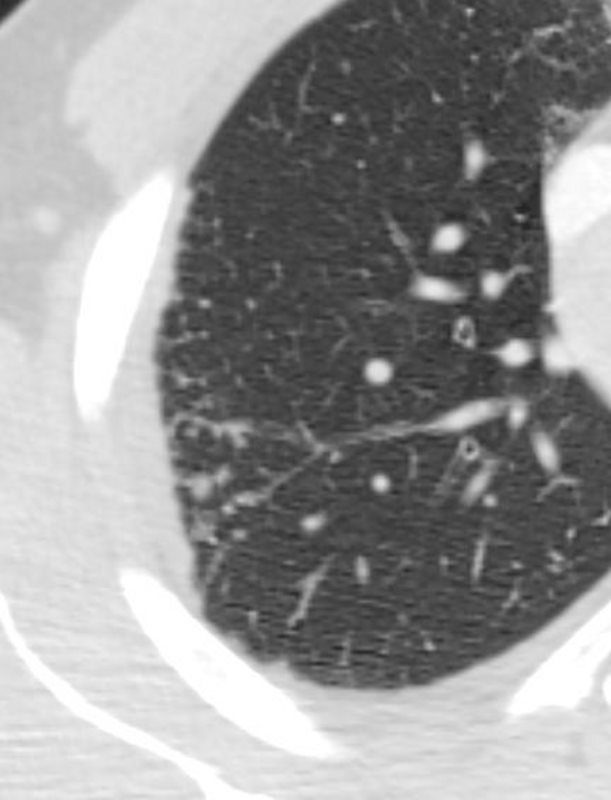
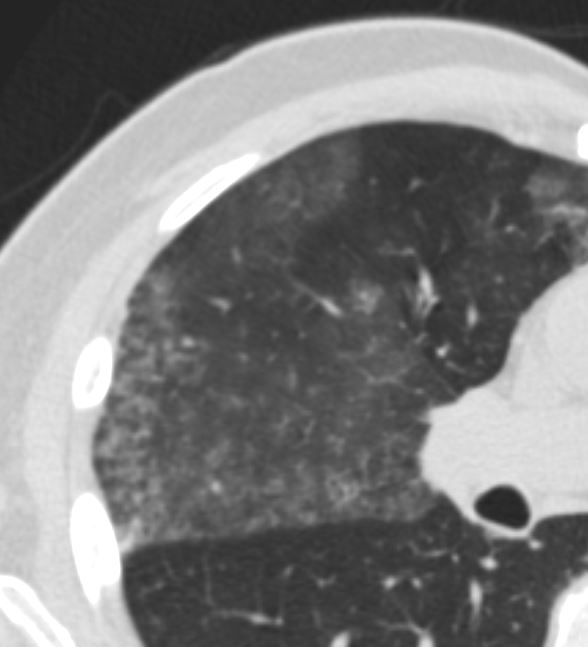
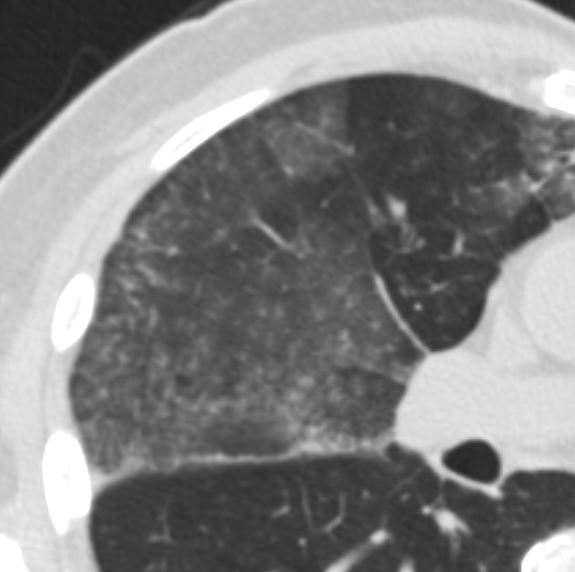
77F with long history of dyspnea and cough showing medium and small airway disease, centri-lobular nodules, para-septal nodules ground glass changes and mosaic attenuation Diagnosis includes Stage 3 sarcoidosis
Ashley Davidoff
TheCommonVein.net
77F with long history of dyspnea and cough showing medium and small airway disease, centri-lobular nodules, para-septal nodules ground glass changes and mosaic attenuation Diagnosis includes Stage 3 sarcoidosis
Ashley Davidoff TheCommonVein.net
77F with long history of dyspnea and cough showing medium and small airway disease, centri-lobular nodules, para-septal nodules ground glass changes and mosaic attenuation Diagnosis includes Stage 3 sarcoidosis
Ashley Davidoff TheCommonVein.net
77F with long history of dyspnea and cough showing medium and small airway disease, centri-lobular nodules, para-septal nodules ground glass changes and mosaic attenuation Diagnosis includes Stage 3 sarcoidosis
Ashley Davidoff TheCommonVein.net

77F with long history of dyspnea and cough showing medium and small airway disease, centrii-lobular nodules, paraseptal nodules ground glass changes and mosaic attenuation Diagnosis includes Stage 3 sarcoidosis
Ashley Davidoff TheCommonVein.net
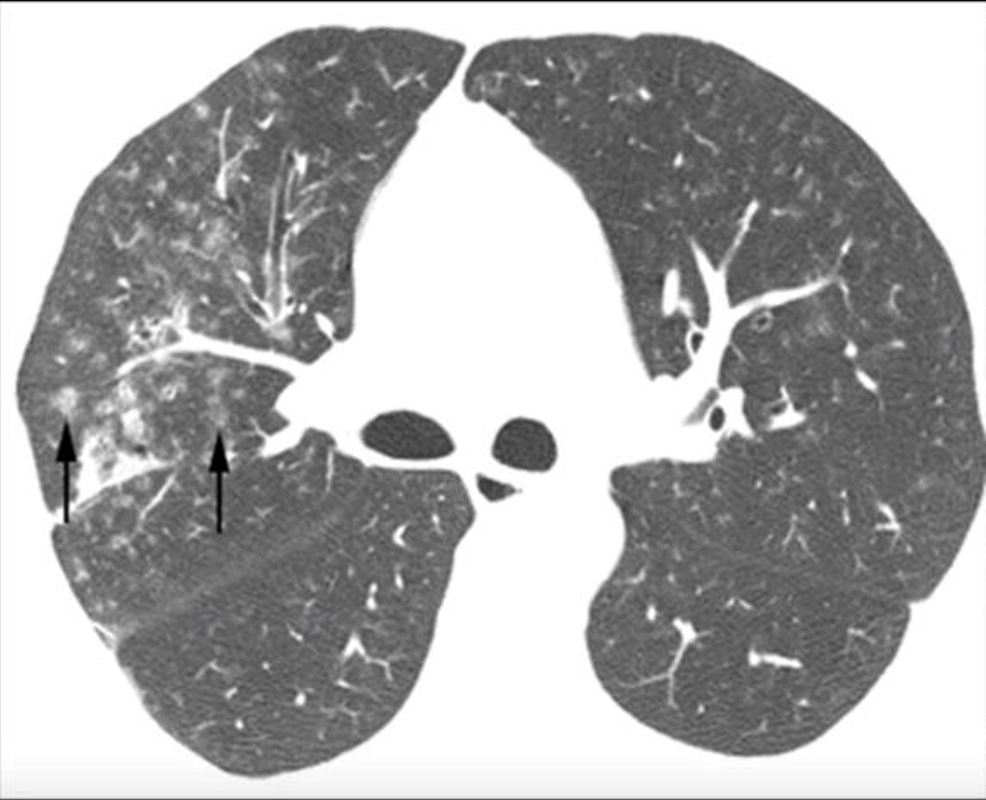
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
48-year-old previously well presented with dyspnea and initial CXR showed an infiltrate at the right base, and clinically resolved. He presented a year later with right chest pain and low grade ever and the CXR showed patchy opacities in the LUL and in the RLL
A subsequent CT showed LUL nodular opacities and subpleural rim of consolidation in the LUL and more prominently at both lung bases, associated with significant mediastinal adenopathy. Lymphovacscular nodularity was noted in the bronchovascular bundles as well as in the interlobular septa, consistent with sarcoidosis
CXR and CT 4 years later showed almost complete resolution of the parenchymal findings and the CT findings except for minimal reticulation and scarring in the subpleural regions
Ashley Davidoff MD
Hypersensitivity Pneumonitis
Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD thecommonvein.net
Carcinoma

50 year old female with primary adenocarcinoma of the left lung with diffuse bilateral lymphangitic spread of disease characterized by lymphovascular distribution.
The nodularity on the fissures characterize the lymphatic distribution and the nodules are likely of a mixed nature, some being in the interlobular septa, and some in a centrilobular distribution .
Ashley Davidoff MD
50 year old female with primary adenocarcinoma of the left lung with diffuse bilateral lymphangitic spread of disease characterized by lymhovascular distribution.
The nodularity on the fissures characterize the lymphatic distribution and the nodules are likely of a mixed nature, some being in the iinterlobular septa, and some in a centrilobular distribution .
Ashley Davidoff MD
The lower panels demonstrate centrilobular distribution of someof the nodules
Ashley Davidoff MD
TheCommonVein.net
134336c
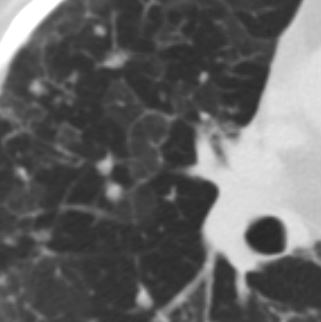
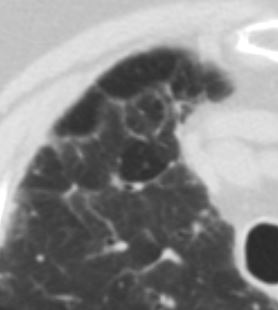
Micronodules in ILD is another CT feature of interstitial lung disease and is characterised by nodules of a variety of shapes and sizes and likely centrilobular in origin. Sometimes they are ill defined such as in this case.
Obliterative bronchiolitis after bone marrow transplantation
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
Tumor Emboli from Gastric Adenocarcinoma
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
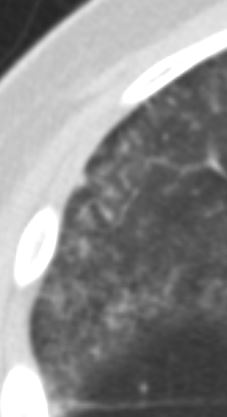
CHF and Centrilobular Nodules
Pre Dialysis 3 days earlier
Ground Glass Changes Kerley B Lines Centrilobular Nodular Congestion
Ground Glass Changes Kerley B Lines Centrilobular Nodular Congestion
Ashley Davidoff MD TheCommonVein.net 04
Ground Glass Changes Significantly Improved, Kerley B Lines and Centrilobular Congestion Resolved with Possible Mosaic Attenuation and Mosaic Attenuation
Ashley Davidoff MD TheCommonVein.net 04
Focused View of the Region Pre Dialysis 3 days earlier
Ground Glass Changes Kerley B Lines Centrilobular Nodular Congestion
Ground Glass Changes Kerley B Lines Centrilobular Nodular Congestion
Ashley Davidoff MD TheCommonVein.net 05
Focused View of the Region Post dialysis – 6.5 Liters
Ground Glass Changes Significantly Improved, Kerley B Lines and Centrilobular Congestion Resolved with Possible Mosaic Attenuation and Mosaic Attenuation
Ground Glass Changes Significantly Improved, Kerley B Lines and Centrilobular Congestion Resolved with Possible Mosaic Attenuation
Ashley Davidoff MD TheCommonVein.net 05
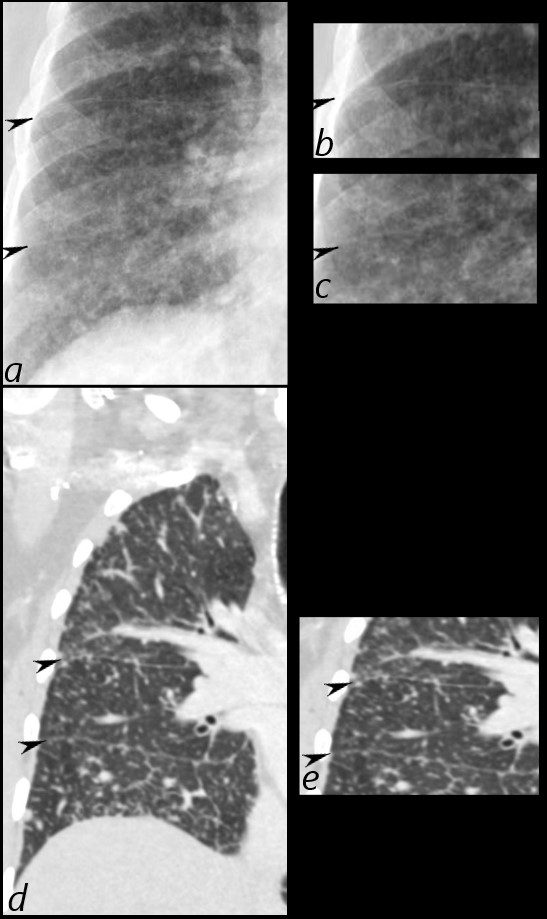
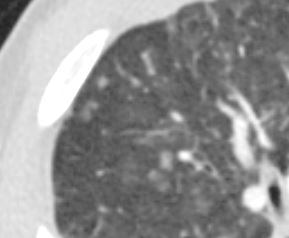
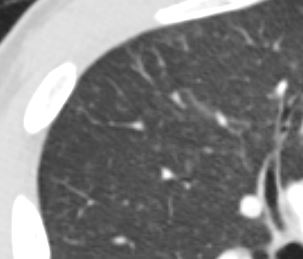
Amyloidosis
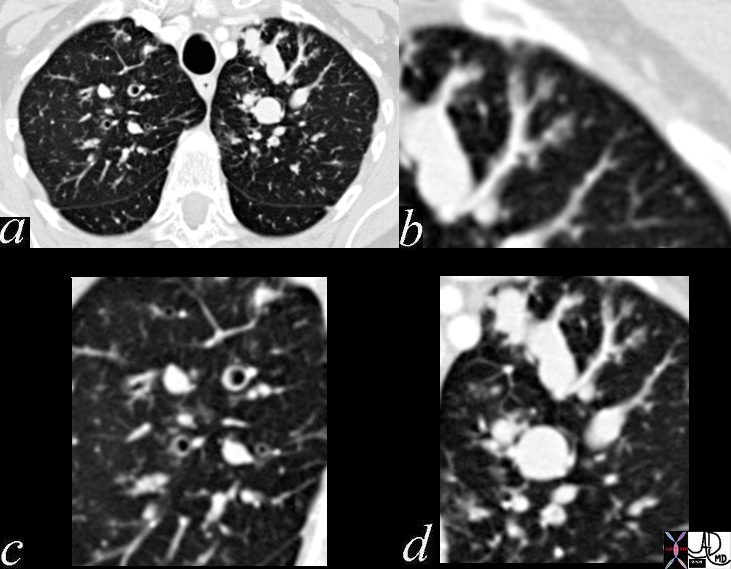
Both Small Vessels and Small Airway are Involved
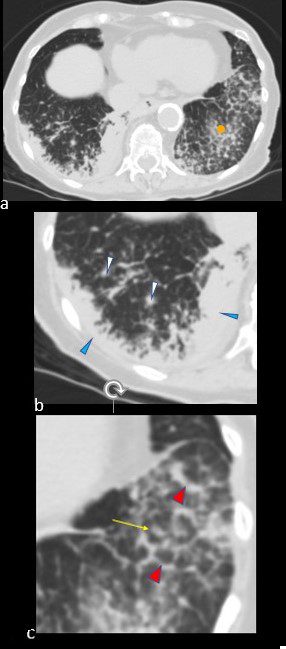
CT scan in the axial projection at the base of the lungs show many features of amyloidosis including lung nodules (white arrowheads) and infiltrates (b), and diffuse deposition within the alveolar septa (red arrowheads, c) and centrilobular nodules(yellow arrow c)
Ashley Davidoff MD Boston Medical Center
TheCommonVein.net septal-amyloidosis-001b