
Infection
Infective Endocarditis
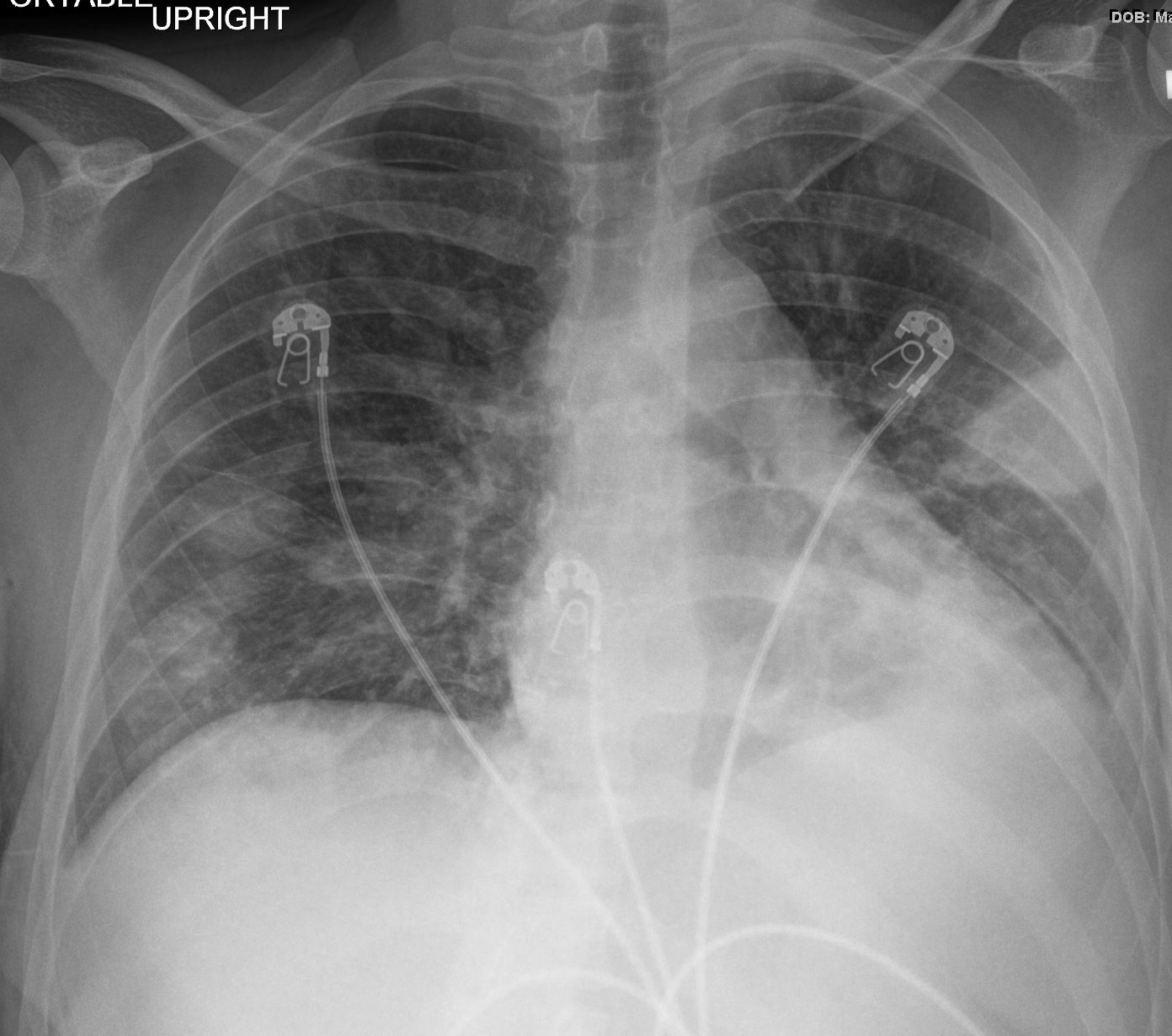
Ashley Davidoff MD TheCommonvein.net 24f PE Hampton’s hump 001

Ashley Davidoff MD TheCommonvein.net 24f PE Hampton’s hump 002
Neoplasm
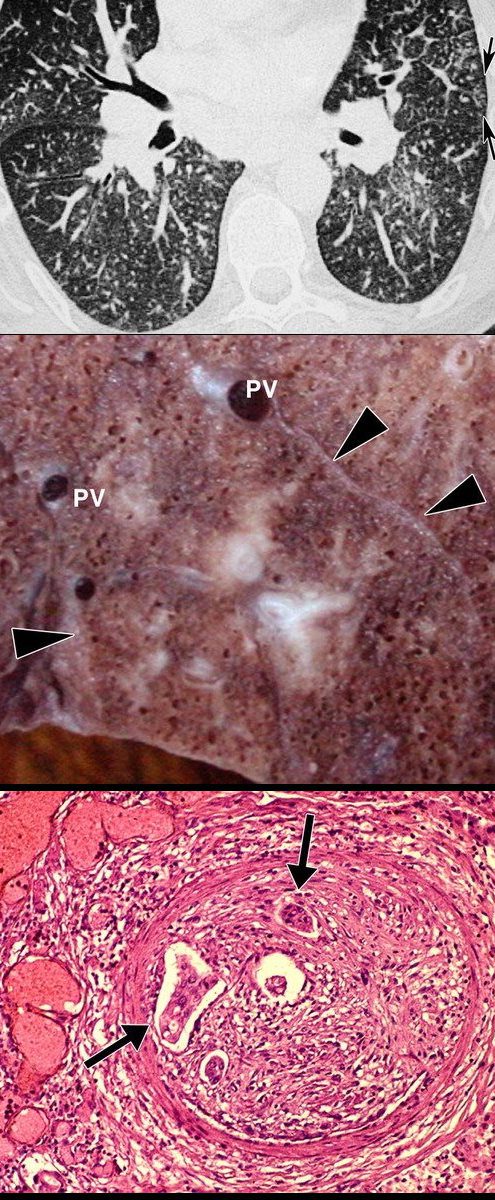
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphicsVol. 25, No. 3 2005
Circulatory
Main Pulmonary Arteries
Saddle Embolus
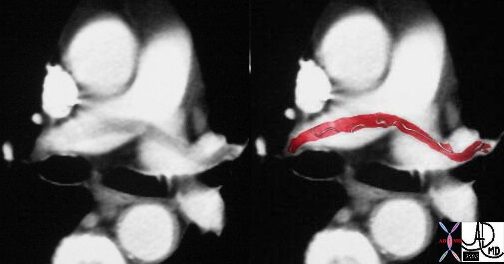
This case of a saddle embolus shows a thrombus sitting astride the left and right pulmonary arteries. Contemporary CTA is able to identify emboli in secondary and tertiary branches just as well. CTA has become the gold standard and study of choice in the patient with chest pain or acute desaturation with suspected PE.
Ashley Davidoff MD TheCommonVein.net 30008c

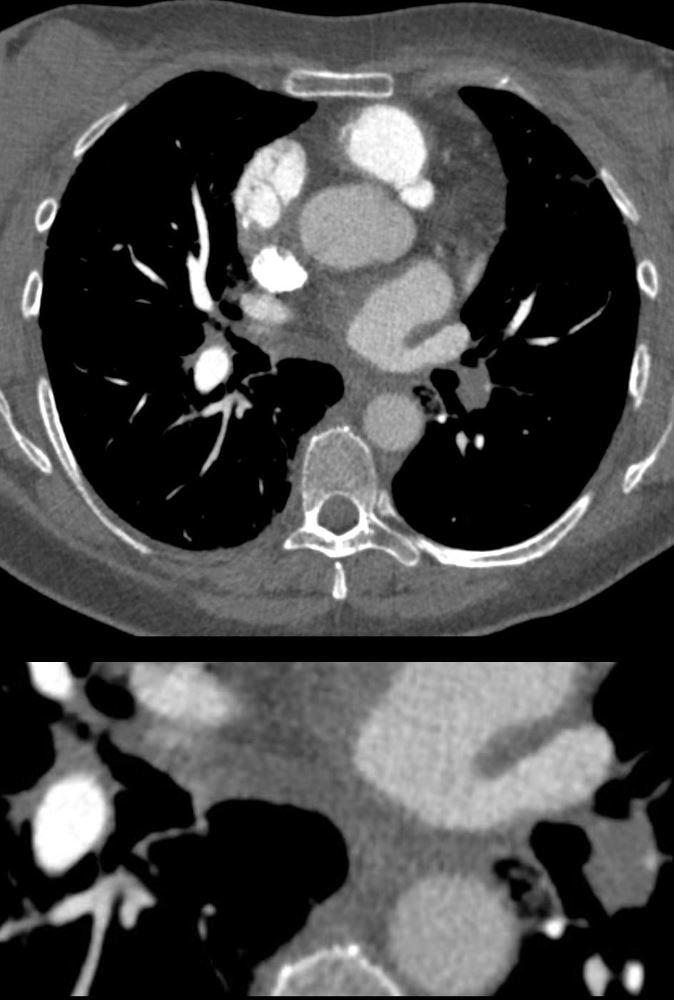
CT in the axial plane in a patient with acute dyspnea and chest pain shows embolic filling defects almost occluding the right pulmonary artery and partially occluding the left pulmonary artery consistent with acute occluding pulmonary emboli
Ashley Davidoff MD TheCommonVein.net 86257c
56 -year-old female with a history of amyloidosis presenting with tachycardia and dyspnea. CTPA shows an occlusive embolus (PE) in the left lower lobe pulmonary artery.
Ashley Davidoff MD TheCommonVein.net 135738c
Mismatched Ventilation- Perfusion (V/Q) Scan Multiple Bilateral Pulmonary Emboli
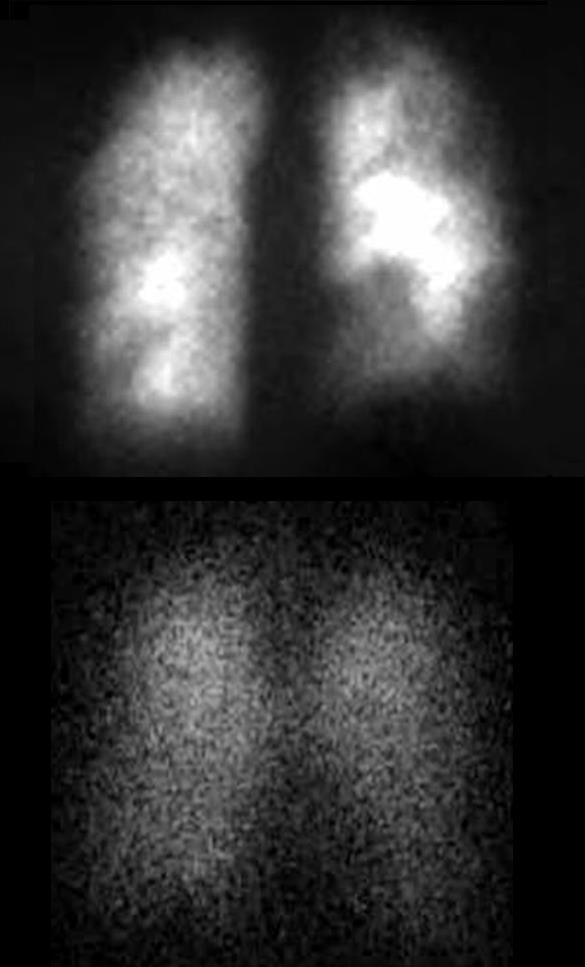
28-year-old female on OCP with leg swelling, chest pain and dyspnea.
Previously performed CXR was normal. Perfusion scan (above) shows multiple bilateral perfusion defects which are not matched on the ventilation scan (below). These findings are consistent with multiple pulmonary emboli
Ashley Davidoff MD TheCommonVein.net 274Lu 11006c02
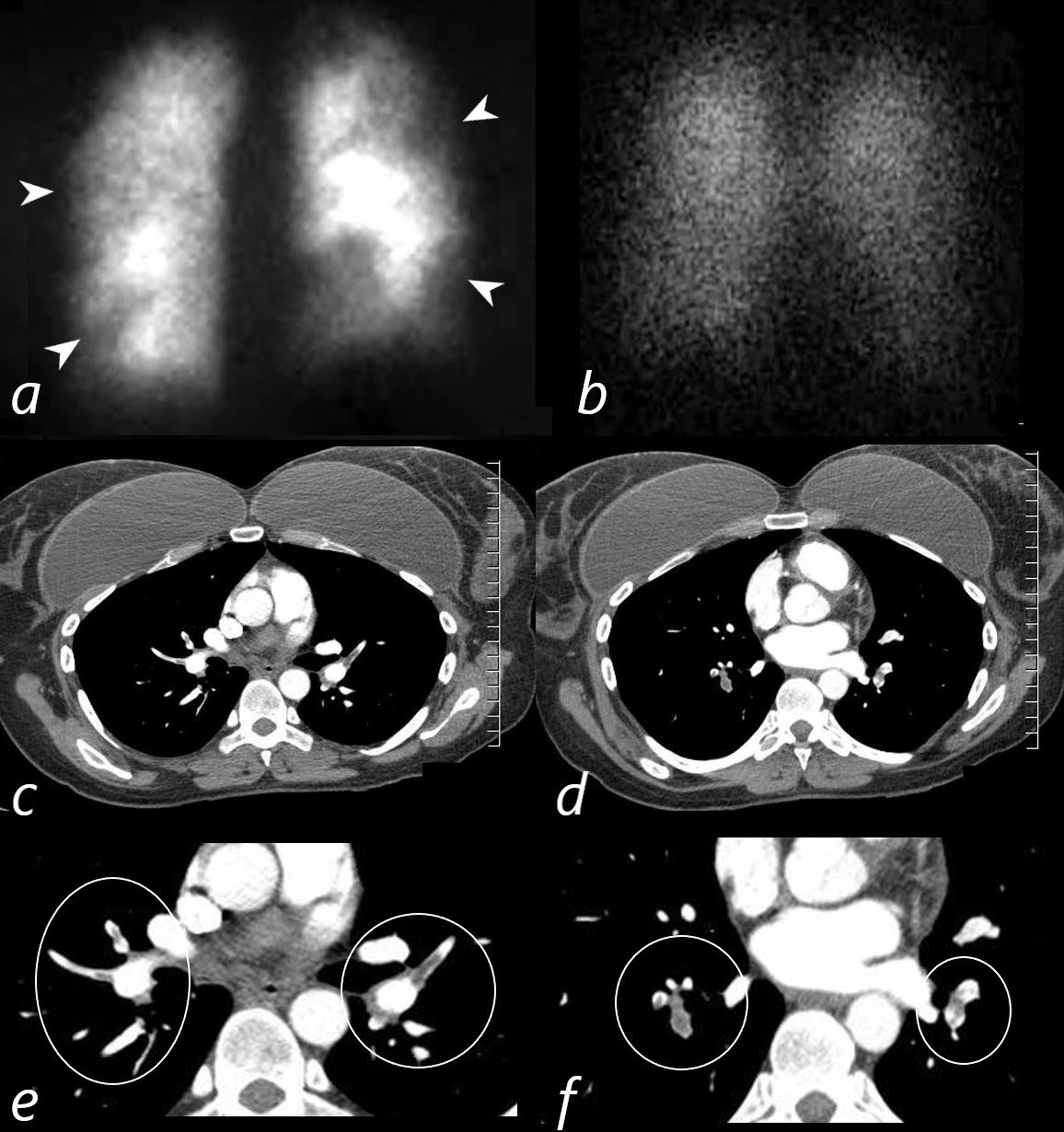
28-year-old female on OCP with leg swelling, chest pain and dyspnea.
Previously performed CXR was normal. Perfusion scan (a) shows multiple bilateral perfusion defects (white arrowheads) which are not matched on the normal ventilation scan (b). These findings are consistent with multiple pulmonary emboli. CT scan through the upper and mid portions of the chest (c,d) confirm the presence of multiple occlusive and non-occlusive pulmonary emboli magnified and ringed (e,f)
Ashley Davidoff MD TheCommonVein.net 274Lu 11006c03L
PE and No Enhancement of the Left Lower Lobe Arterial Segments and Small Wedge Shape Infarction (Hamptons Hump)

56 -year-old female with a history of amyloidosis presenting with tachycardia and dyspnea. CTPA shows no contrast enhancement of the pulmonary arteries subtending the left lower lobe compared to the right and a subsegmental wedge shaped defect (Hampton’s hump) in the lateral segment of the left lower lobe
Ashley Davidoff MD TheCommonVein.net 135739c
PE and No Enhancement of the Left Lower Lobe-
Dual Energy Iodine Map
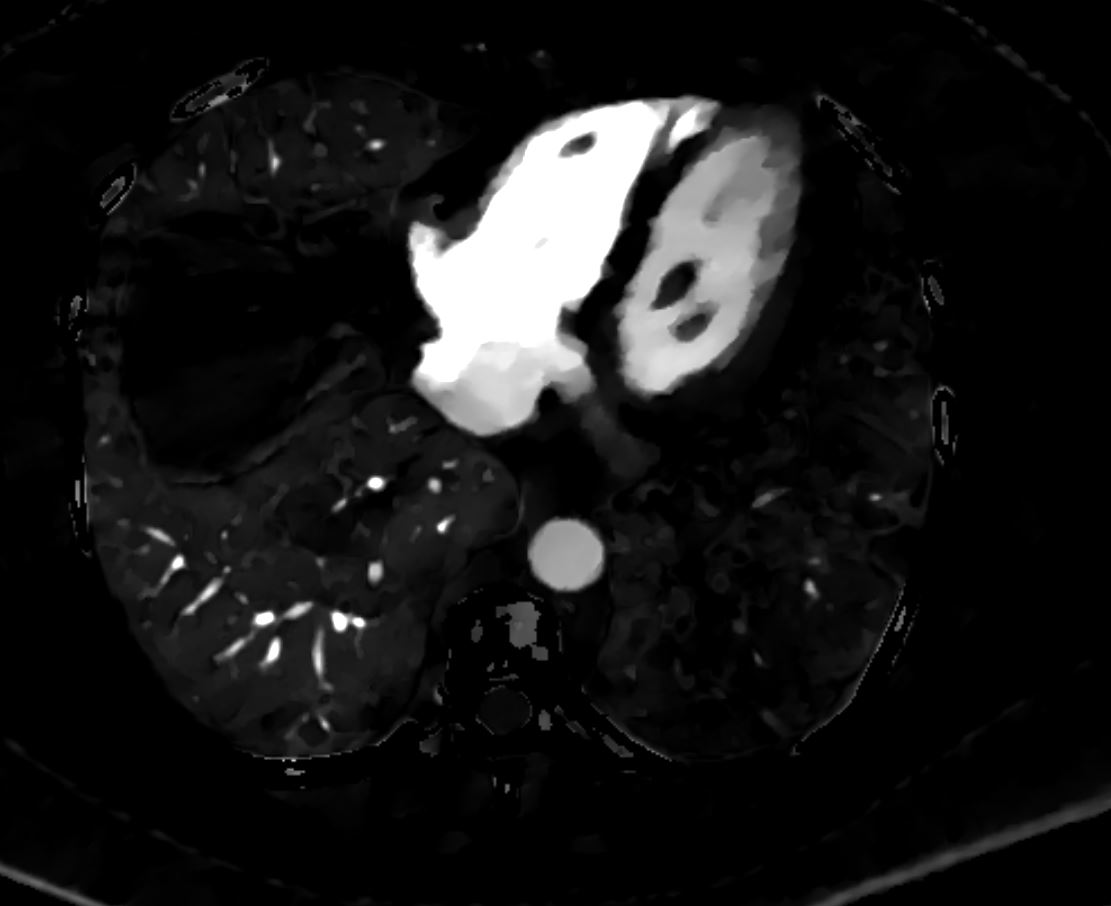
Perfusion Defect of the Left Lower Lobe from Occlusive Pulmonary Embolus
56 -year-old female with a history of amyloidosis presenting with tachycardia and dyspnea. Dual energy CT with an iodine map shows shows an almost lobar perfusion defect of the left lower lobe compared
Ashley Davidoff MD TheCommonVein.net 135740
Subsegmental Infarction
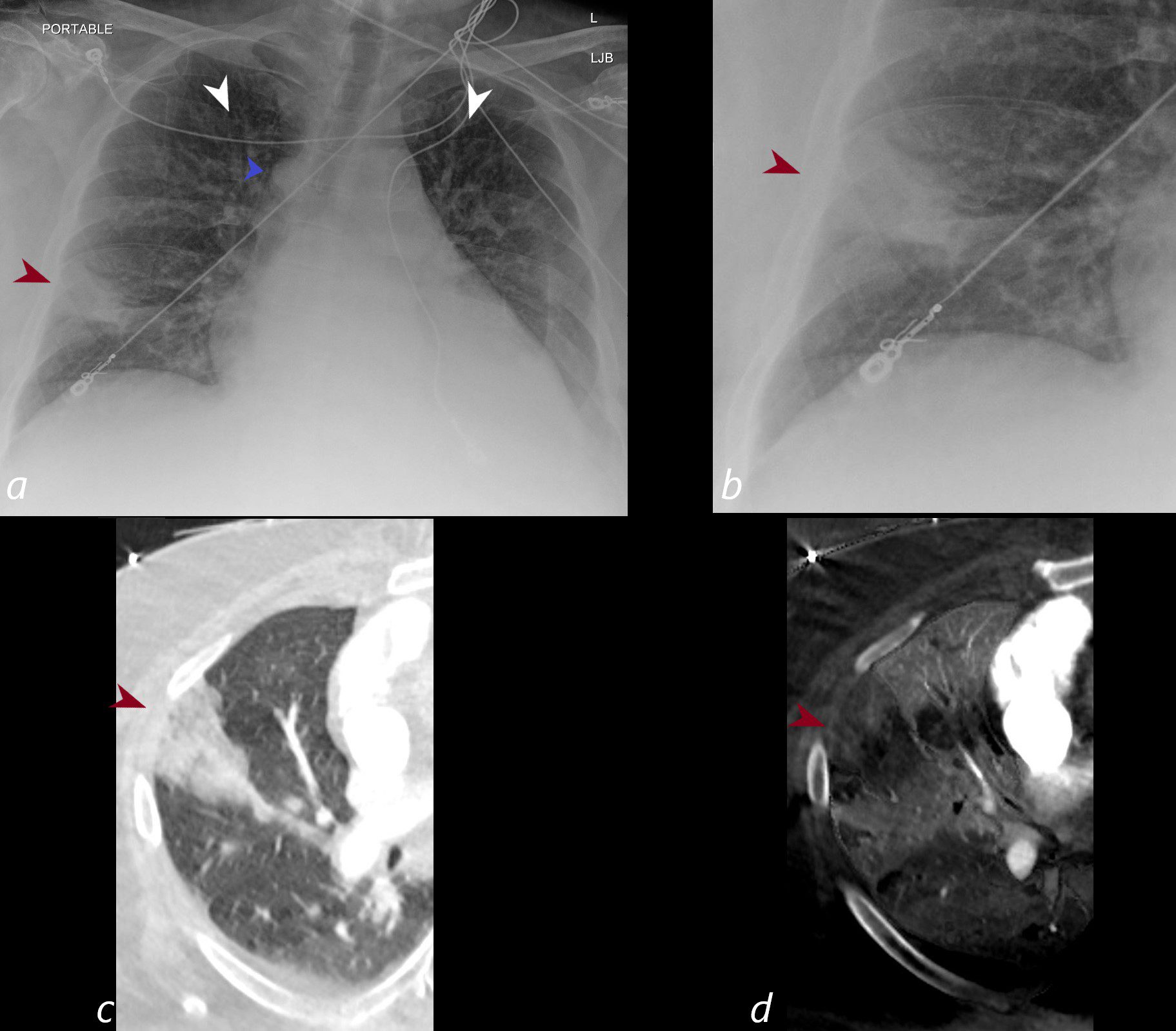
CXR shows a wedge shaped infiltrate in the middle lobe of the lung secondary to a pulmonary embolus (PE) characteristic of a Hampton’s hump (maroon arrowheads a,b) The infarction is confirmed on the CT with contrast (maroon arrowhead c) as well as the region of a perfusion defect (d- maroon arrowhead) In addition there is evidence of CHF on the CXR with cephalization of the vessels (white arrowheads c) cardiomegaly with left atrial enlargement, and enlargement of the azygous vein (blue arrowhead a)
Ashley Davidoff MD TheCommonVein.net)
Segmental Infarction
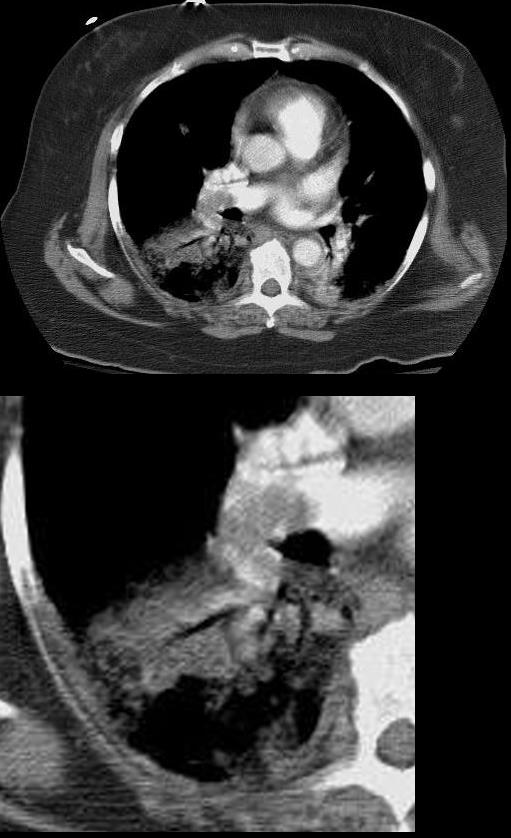
Patient presented with dyspnea and chest pain. CTPA shows large pulmonary embolus subtending a region of right lower lobe infarction.
Ashley Davidoff MD TheCommonVein.net 19443L
Iatrogenic Coils

Courtesy Ashley Davidoff MD TheCommonVein.net 24137