
Buzz The COPS are Everywhere and can Disguise as almost anything
- Structural
- peribronchial consolidation
- Interstitial
- alveoli
- bronchioles
- COPS All Lung Zones COPS can go anywhere
- bronchovascular
- peripheral
- Interstitial
- Path
- interstitial inflammation
- globs of tissue Masson bodies in in distal airspaces and bronchioles
- Imaging CT
- Ground Glass
- Patchy Consolidation
- Atoll Inverted Halo
- Nodules which can cavitate
“When an underlying cause is unknown it is classified as cryptogenic organizing pneumonia (COP; also referred to as primary organizing pneumonia) whereas if a cause is known it is then termed a secondary organizing pneumonia.”
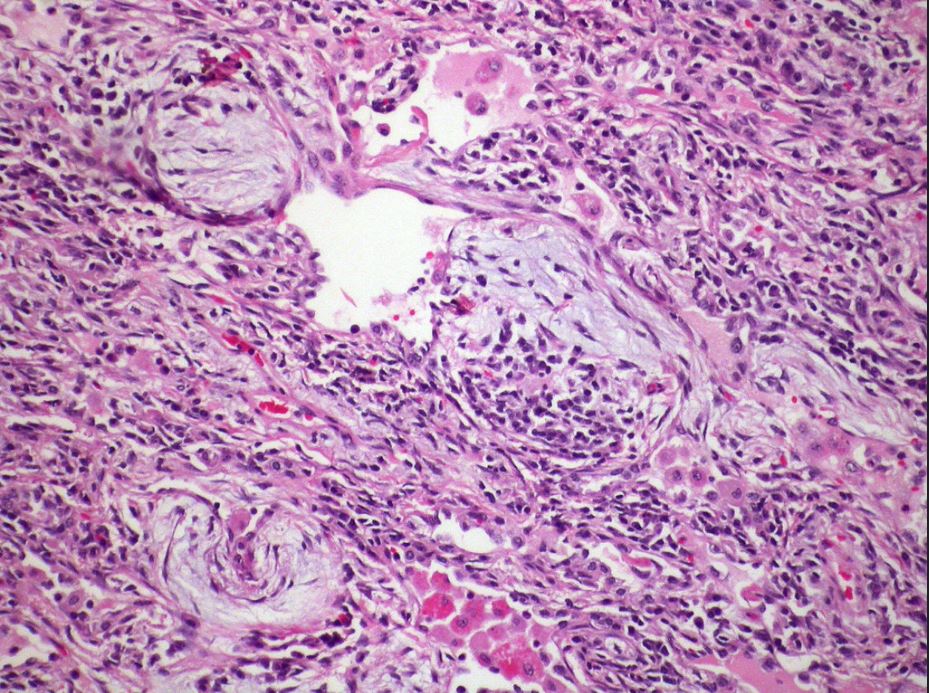
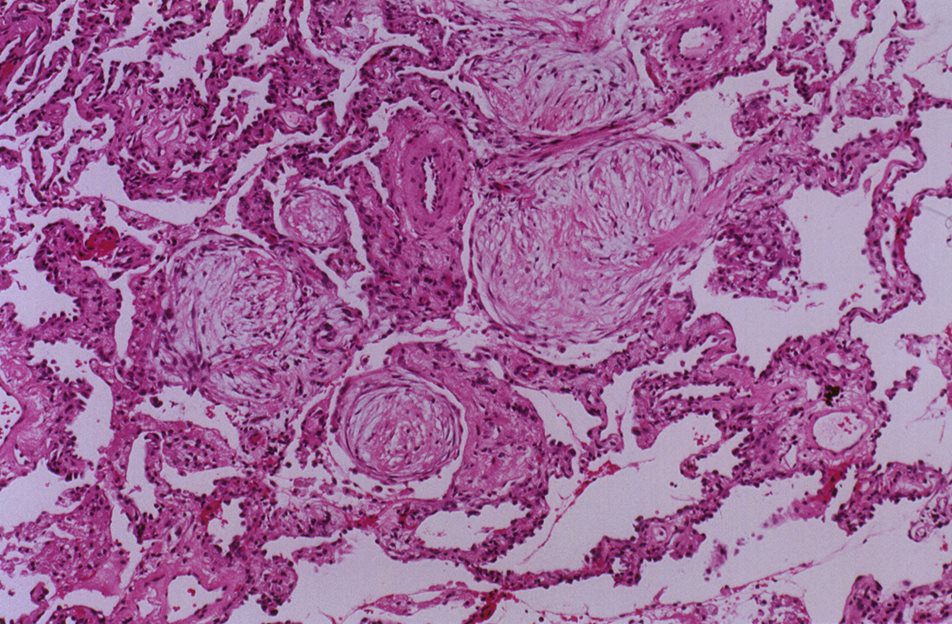
Pathology – “characterized by granulation tissue polyps within alveolar ducts and alveoli and with chronic inflammation involving the adjacent lung parenchyma. ”
Most cases are cryptogenic
- Small Airway Disease – Organizing Pneumonia – Terminal Bronchiole

Hypersensitivity pneumonitis-organizing pneumonia Case 129
Areas of organizing pneumonia are frequently seen in hypersensitivity pneumonitis.
Courtesy Dr Yale Rosen- cryptogenic or secondary organizing pneumonia (OP),
-
Histopathology of organizing pneumonia (or BOOP), characterized by intraluminal plugs of proliferating fibroblasts that fill distal airways and peribonchiolar air spaces
Ryu, J Pulmonary Medicine Bronchiolitis Pulmonology Advisor
COP Pattern

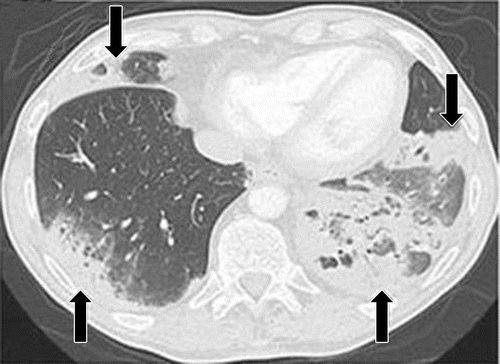
PD-1 inhibitor pneumonitis: COP pattern in a 69-year-old man with advanced NSCLC who was treated with nivolumab. At 6 months of therapy, the patient presented with increased shortness of breath and cough, without fever. Axial chest CT image shows multifocal areas of consolidation and GGOs in a predominantly peripheral and basilar distribution (arrows), representing a COP pattern of PD-1 inhibitor–related pneumonitis. Bronchial dilatation was noted within the areas of consolidation. Nivolumab was withheld, and the patient was treated with corticosteroids, with subsequent improvement.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5
a
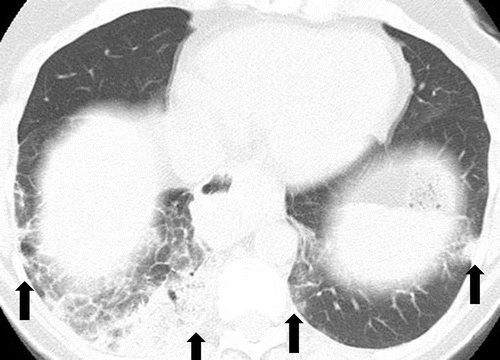
PD-1 inhibitor pneumonitis flare in a 72-year-old man with stage IV squamous NSCLC who was treated with nivolumab and presented with progressive dyspnea with cough and wheezing but no fever. (a) Axial chest CT image at 15 weeks of therapy demonstrates multifocal areas of GGOs, reticular opacities, and consolidation (arrows) involving all lobes, as well as centrilobular nodularity and traction bronchiectasis in a predominantly peripheral distribution. The overall features demonstrate a COP pattern. The patient was treated with prednisone for pneumonitis.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5

b
Axial follow-up CT image after 4 weeks of prednisone therapy shows a significant decrease in the findings, with residual GGOs. Note the “reversed halo” sign manifesting as a central GGO surrounded by a crecent-shaped dense airspace consolidation (arrow), a finding that has been reported as a radiologic manifestation of COP. (c) Axial CT image obtained 4 weeks after the completion of prednisone therapy shows the development of a bilateral dense consolidation with GGOs and reticular opacities (arrows) in peripheral and multifocal distributions, again demonstrating a COP pattern as noted during the first episode of PD-1 inhibitor pneumonitis. Given the similarity of the radiologic and clinical manifestations to those of the first episode, the patient restarted prednisone for treatment of pneumonitis flare. Follow-up chest CT images obtained 2 weeks after starting the second course of prednisone therapy (not shown) demonstrated a decrease in the findings, indicative of improving pneumonitis in response to corticosteroid therapy. (Figure 7 reprinted from reference 21.)
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5

a
PD-1 inhibitor pneumonitis flare in a 72-year-old man with stage IV squamous NSCLC who was treated with nivolumab and presented with progressive dyspnea with cough and wheezing but no fever. (a) Axial chest CT image at 15 weeks of therapy demonstrates multifocal areas of GGOs, reticular opacities, and consolidation (arrows) involving all lobes, as well as centrilobular nodularity and traction bronchiectasis in a predominantly peripheral distribution. The overall features demonstrate a COP pattern. The patient was treated with prednisone for pneumonitis.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5
Pneumonitis in a 66-year-old woman with Waldenström macroglobulinemia treated with mTOR inhibitor therapy. Axial CT image at 6 months of therapy shows consolidation, GGOs, and reticular opacities (arrows) that represent a COP pattern.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5

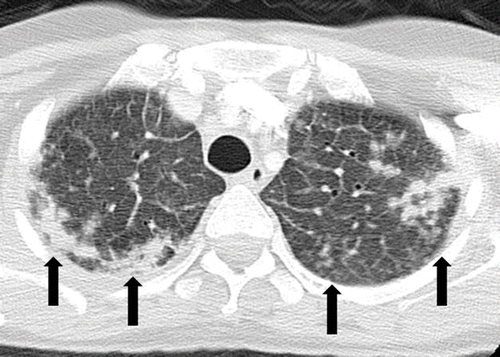
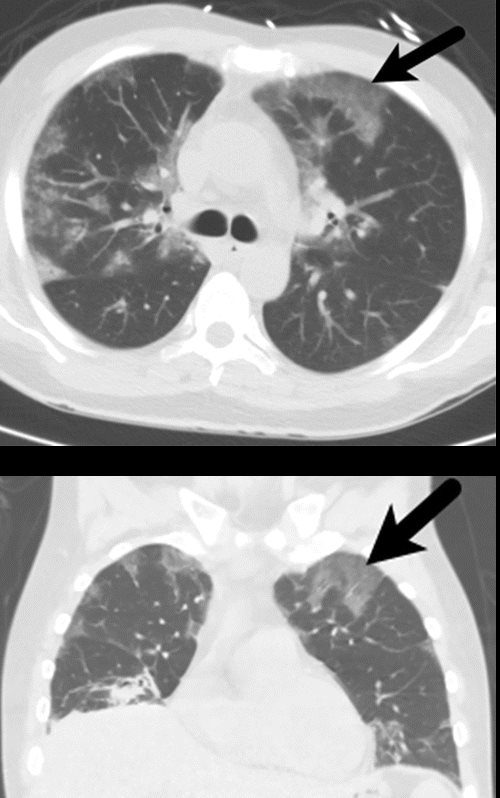
ALK inhibitor–related pneumonitis in a 55-year-old woman with ALK-positive stage IV adenocarcinoma of the lung. The patient experienced disease progression while taking a first-generation ALK inhibitor (crizotinib) and was then treated with a second-generation ALK inhibitor (ceritinib). She presented with an increasing dry cough and dyspnea at 7 months of ceritinib therapy. (a, b) Axial (a) and coronal (b) CT images show biapical consolidation and GGOs in both upper lobes (arrows) in a striking peripheral distribution, indicative of a COP pattern.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5
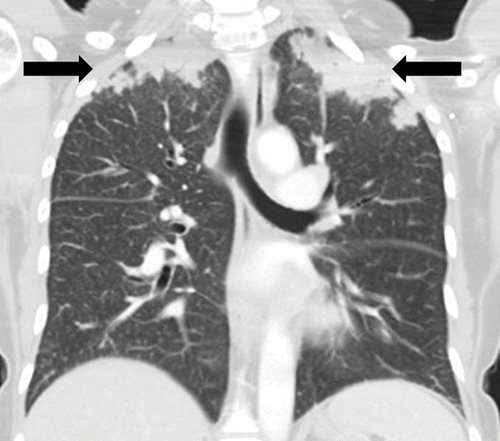
ALK inhibitor–related pneumonitis in a 55-year-old woman with ALK-positive stage IV adenocarcinoma of the lung. The patient experienced disease progression while taking a first-generation ALK inhibitor (crizotinib) and was then treated with a second-generation ALK inhibitor (ceritinib). She presented with an increasing dry cough and dyspnea at 7 months of ceritinib therapy. (a, b) Axial (a) and coronal (b) CT images show biapical consolidation and GGOs in both upper lobes (arrows) in a striking peripheral distribution, indicative of a COP pattern.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5
ALK inhibitor–related pneumonitis in a 55-year-old woman with ALK-positive stage IV adenocarcinoma of the lung. The patient experienced disease progression while taking a first-generation ALK inhibitor (crizotinib) and was then treated with a second-generation ALK inhibitor (ceritinib). She presented with an increasing dry cough and dyspnea at 7 months of ceritinib therapy. (a, b) Axial (a) and coronal (b) CT images show biapical consolidation and GGOs in both upper lobes (arrows) in a striking peripheral distribution, indicative of a COP pattern.
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care Radio Graphics Vol. 37, No. 5
c
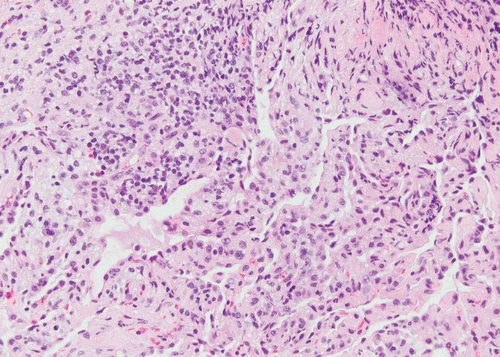
(c, d) Photomicrographs from transbronchial lung biopsy specimen show organizing interstitial pneumonia characterized by alveolar interstitial widening by lymphocytic infiltrates, increased extracellular matrix material, reactive pneumocyte hyperplasia, scattered eosinophils (arrow in d), and numerous airspace foamy macrophages. There was no evidence of tumor in the biopsy specimen. (Hematoxylin-eosin stain; original magnification, ×200 in c, ×400 in d.)
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
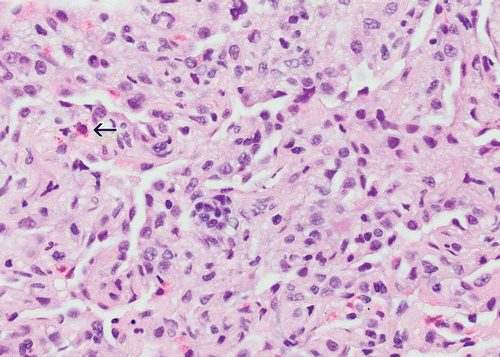
d
(c, d) Photomicrographs from transbronchial lung biopsy specimen show organizing interstitial pneumonia characterized by alveolar interstitial widening by lymphocytic infiltrates, increased extracellular matrix material, reactive pneumocyte hyperplasia, scattered eosinophils (arrow in d), and numerous airspace foamy macrophages. There was no evidence of tumor in the biopsy specimen. (Hematoxylin-eosin stain; original magnification, ×200 in c, ×400 in d.)
Nishino, M et al Thoracic Complications of Precision Cancer Therapies: A Practical Guide for Radiologists in the New Era of Cancer Care RadioGraphicsVol. 37, No. 5
-
Organizing pneumonia. (a) Axial and (b) coronal images in lung windows in a 43-year-old man with a history of follicular lymphoma demonstrate predominantly peripheral ground-glass opacities (arrow). The patient had undergone chemotherapy and was admitted for respiratory failure. Lung biopsy yielded organizing pneumonia. The patient did well on steroids and was discharged.
Parekh, M et al Review of the Chest CT Differential Diagnosis of Ground-Glass Opacities in the COVID Era Radiology Vol. 297, No. 3 July 2020
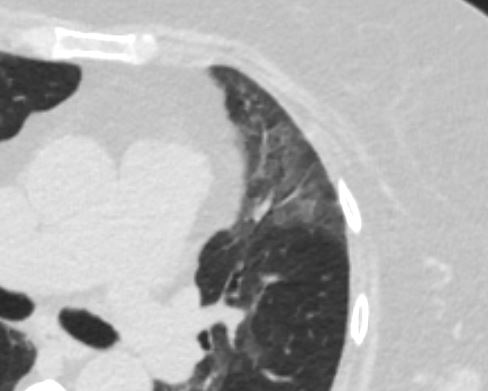
Case of a patient in remission from adult T-cell lymphoma/leukemia, now with multiple PET, AVID lung nodules Pathology showed Acute organizing pneumonitis which could be part of any condition in the lung such as an infection. CT showed cavitating nodules and solid nodules which were PET AVID The conclusion was that even though the pathology showed organizing pneumonitis, it could still be a response to the infection
Cavitating and solid nodules PATH Acute organizing pneumonitis
Ashley Davidoff thecommonvein.net
Ashley Davidoff thecommonvein.net
Ashley Davidoff thecommonvein.net

Ashley Davidoff thecommonvein.net
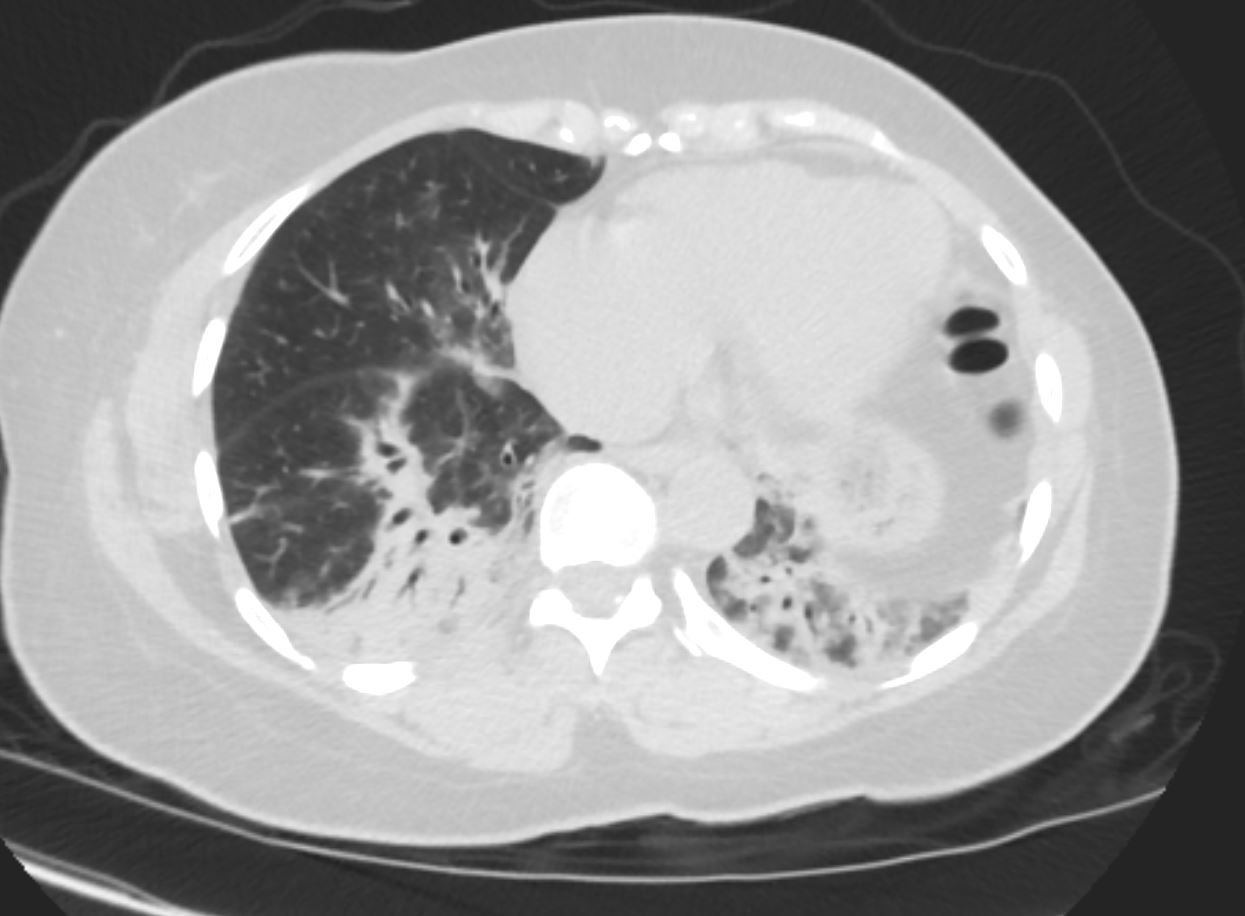
COP vs NSIP

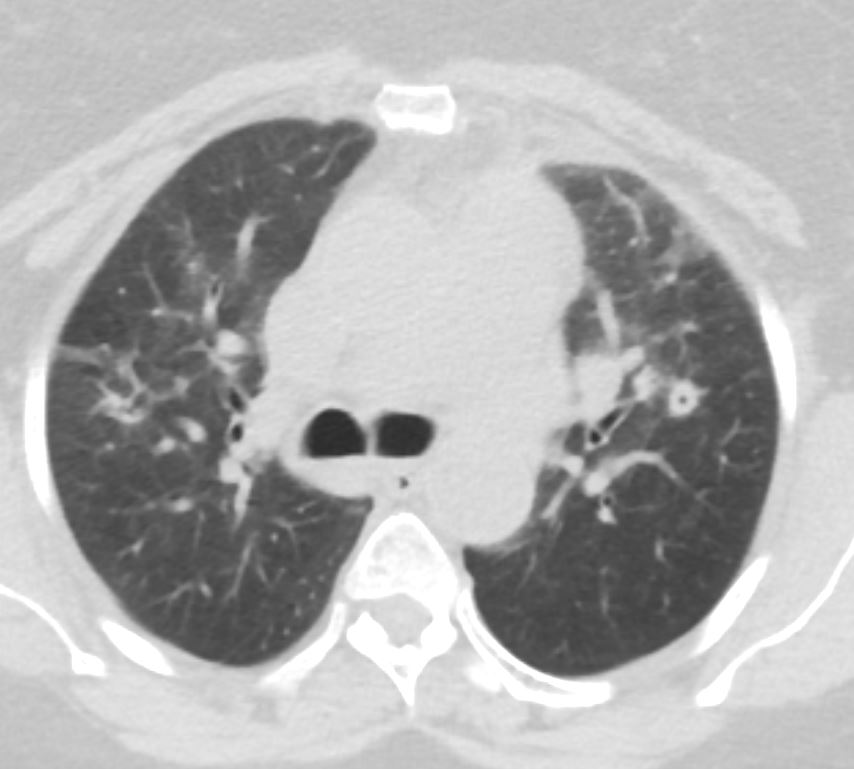
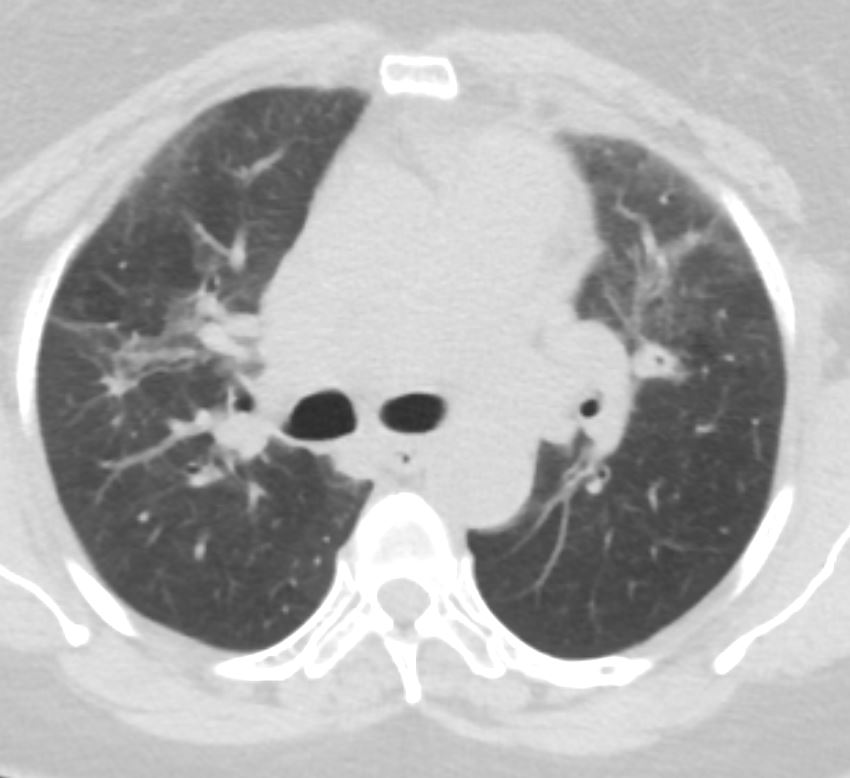
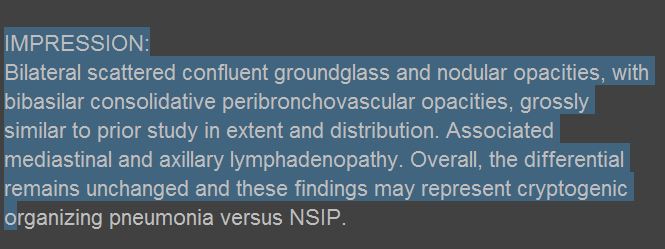
56 year old female presents with CT findings of basilar bronchovascular infiltrates, almost symmetrical, associated with mediastinal and axillary adenopathy.
Pathological report was complex but suggested a diagnosis of cryptogenic organizing pneumonia Ashley Davidoff MD TheCommonVein.net
56 year old female presents with CT findings of basilar bronchovascular infiltrates, almost symmetrical, associated with mediastinal and axillary adenopathy.
Pathological report was complex but suggested a diagnosis of cryptogenic organizing pneumonia
Ashley Davidoff MD TheCommonVein.net
1 Year Later
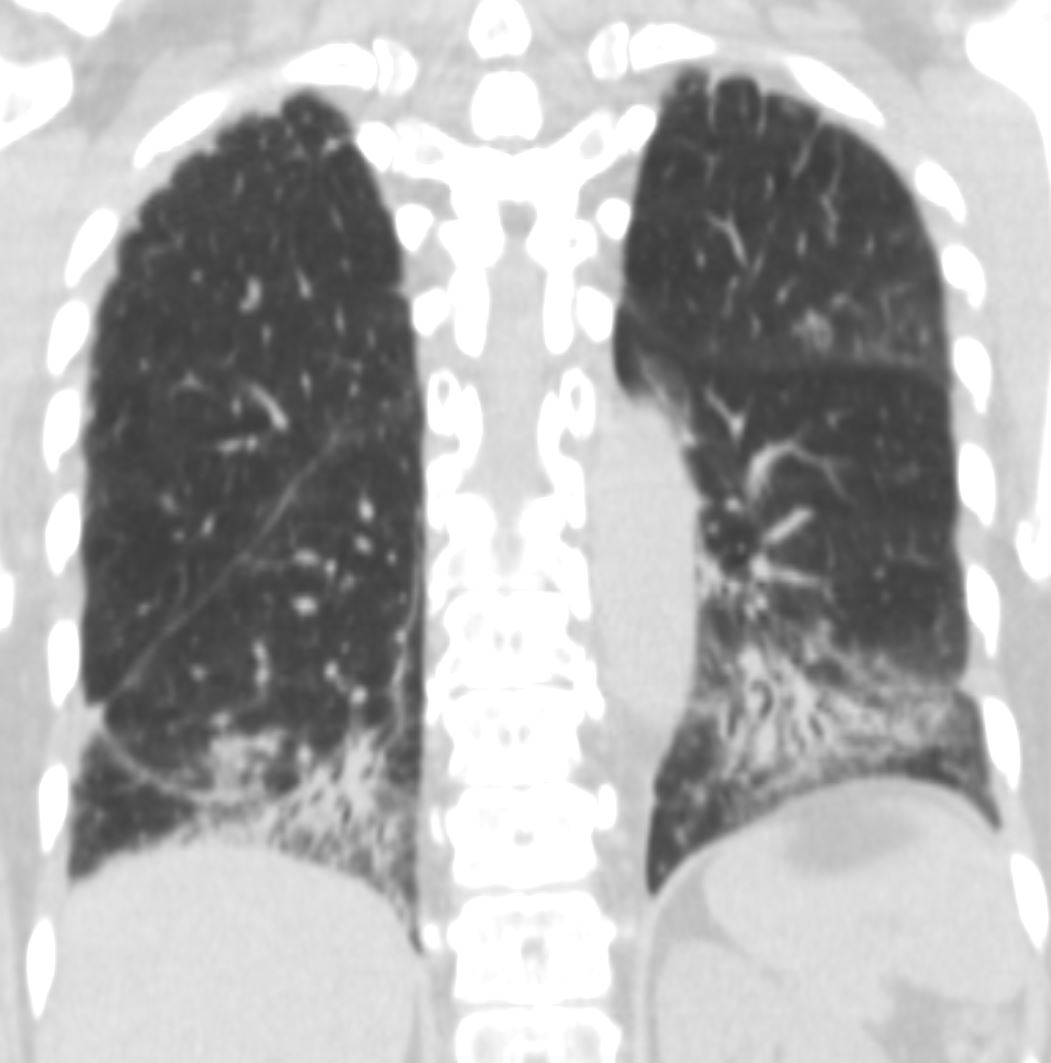
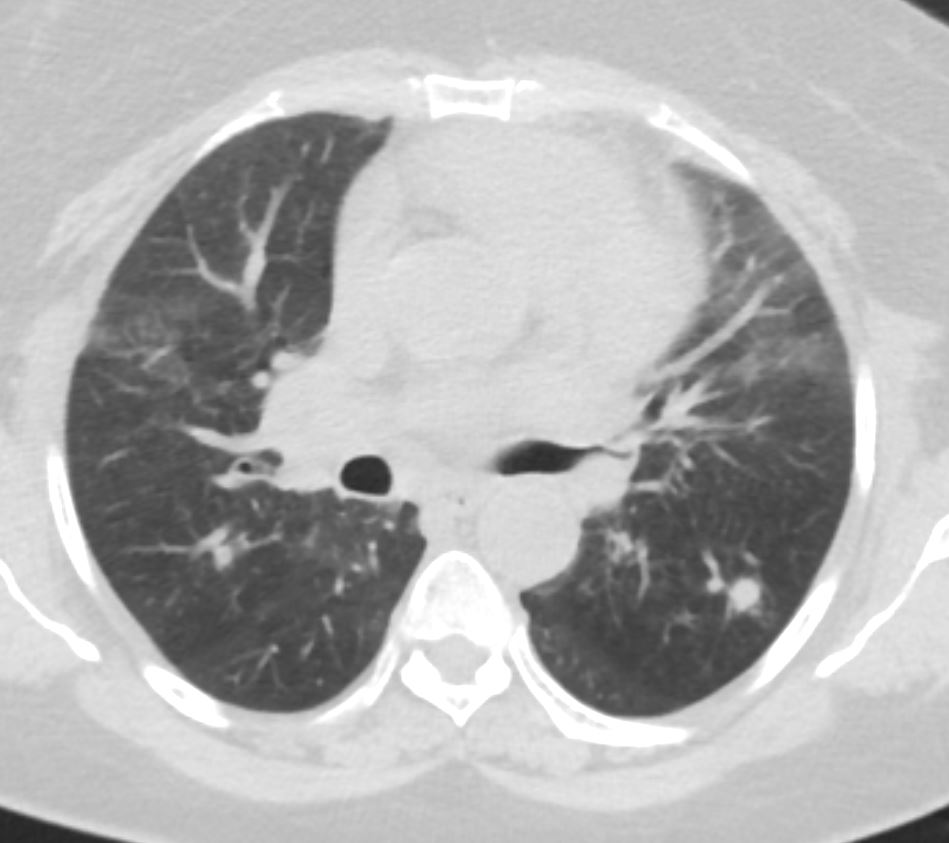
57 year old female presents 1 year later with similar CT findings of basilar bronchovascular infiltrates, almost symmetrical, associated with mediastinal and axillary adenopathy.
Pathological report was complex but suggested a diagnosis of cryptogenic organizing pneumonia
Ashley Davidoff MD
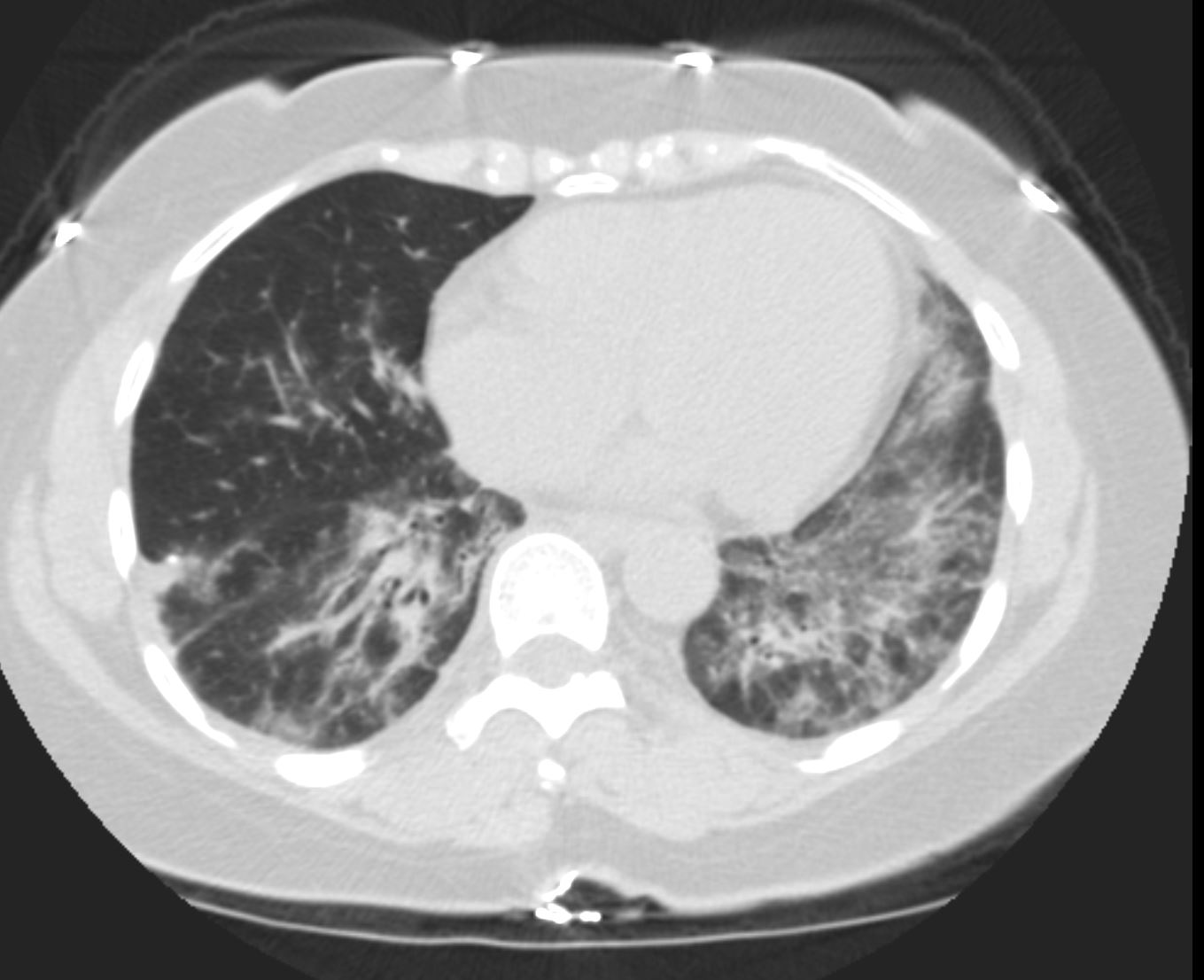
COP vs NSIP
57 year old female presents 1 year later with similar CT findings of basilar bronchovascular infiltrates, almost symmetrical, associated with mediastinal and axillary adenopathy.
Pathological report was complex but suggested a diagnosis of cryptogenic organizing pneumonia
Ashley Davidoff MD TheCommonVein.net
Pathology proven diagnosis
Ashley Davidoff MD TheCommonVein.net
References and Links
Tiralongo et al Cryptogenic Organizing Pneumonia: Evolution of Morphological Patterns Assessed by HRCT Diagnostics 2020, 10(5), 262;
- TCV
- Cases