- male approximately middle aged
- polytrauma
- automobile versus motorcycle.
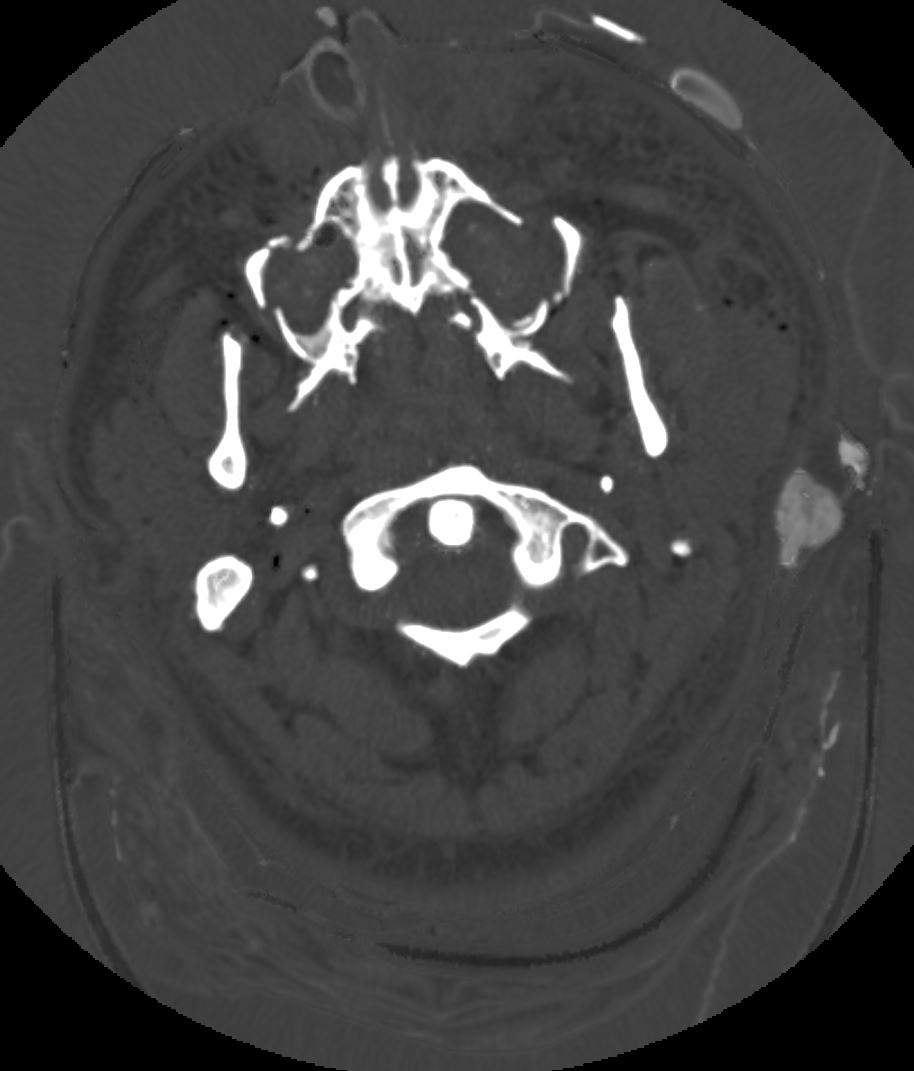
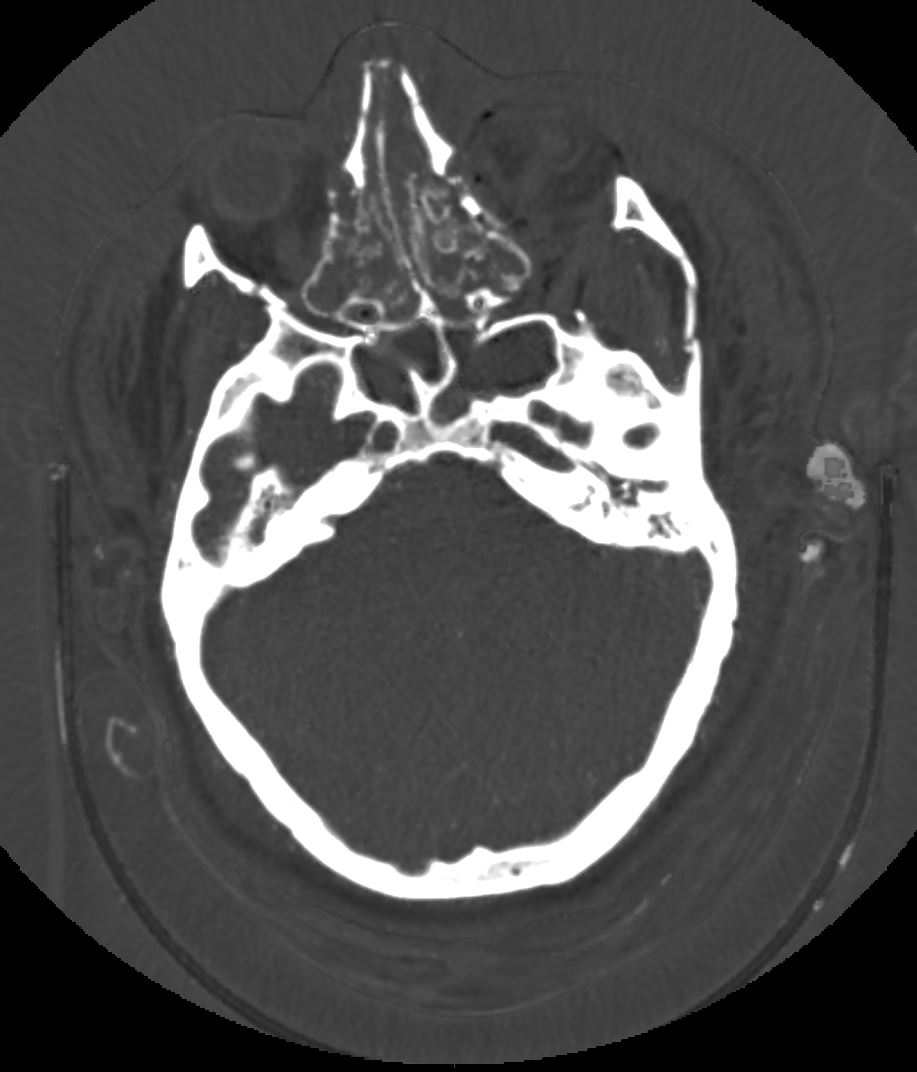
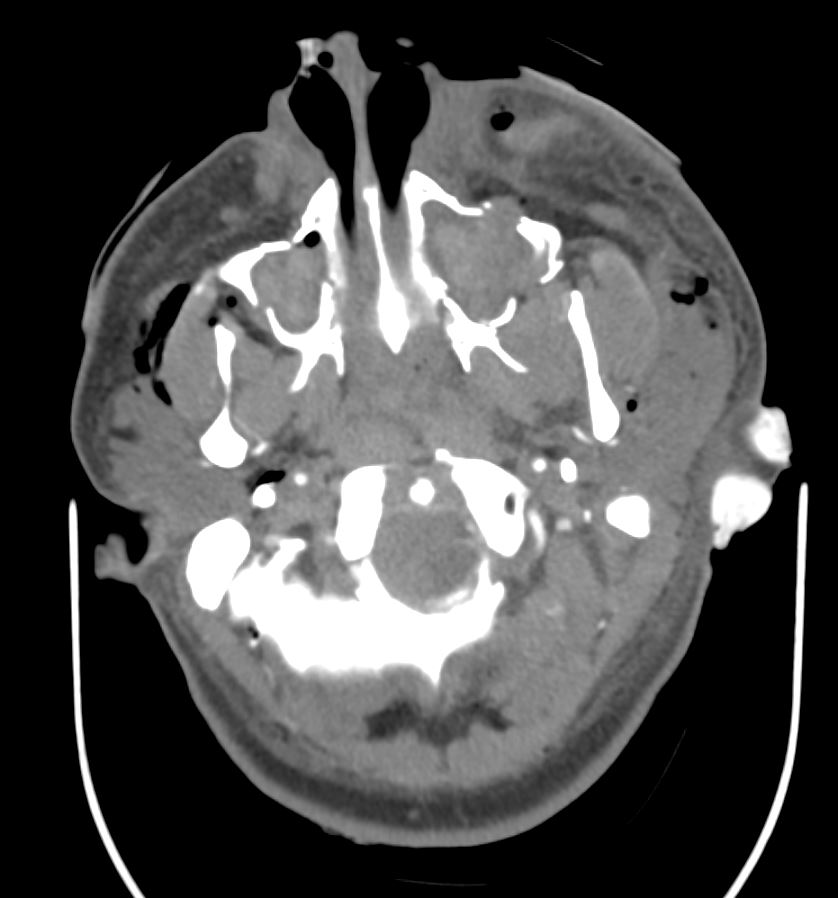
- severe facial trauma,
- attempted intubation at the scene
- attempted needle cricothyrotomy
- outside hospital
- bilateral chest tubes placed
- transfused with 3 units of packed red cells, FFP, platelets
hypotensive, tachycardic to the 160s sinus rhythm
- EFAST
- absent lung sliding on the left,
- lung sliding present on the right,
- positive intra-abdominal fast in the right upper quadrant.
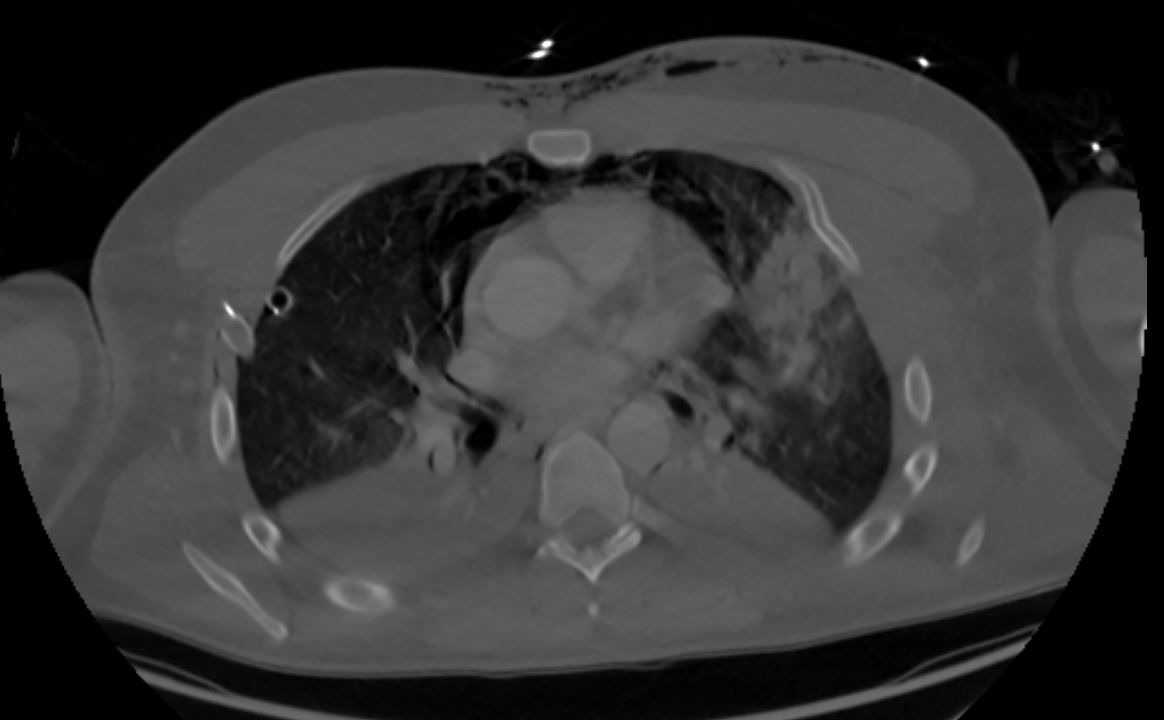
CXR Pneumomediastinum Air Along the left heart Border
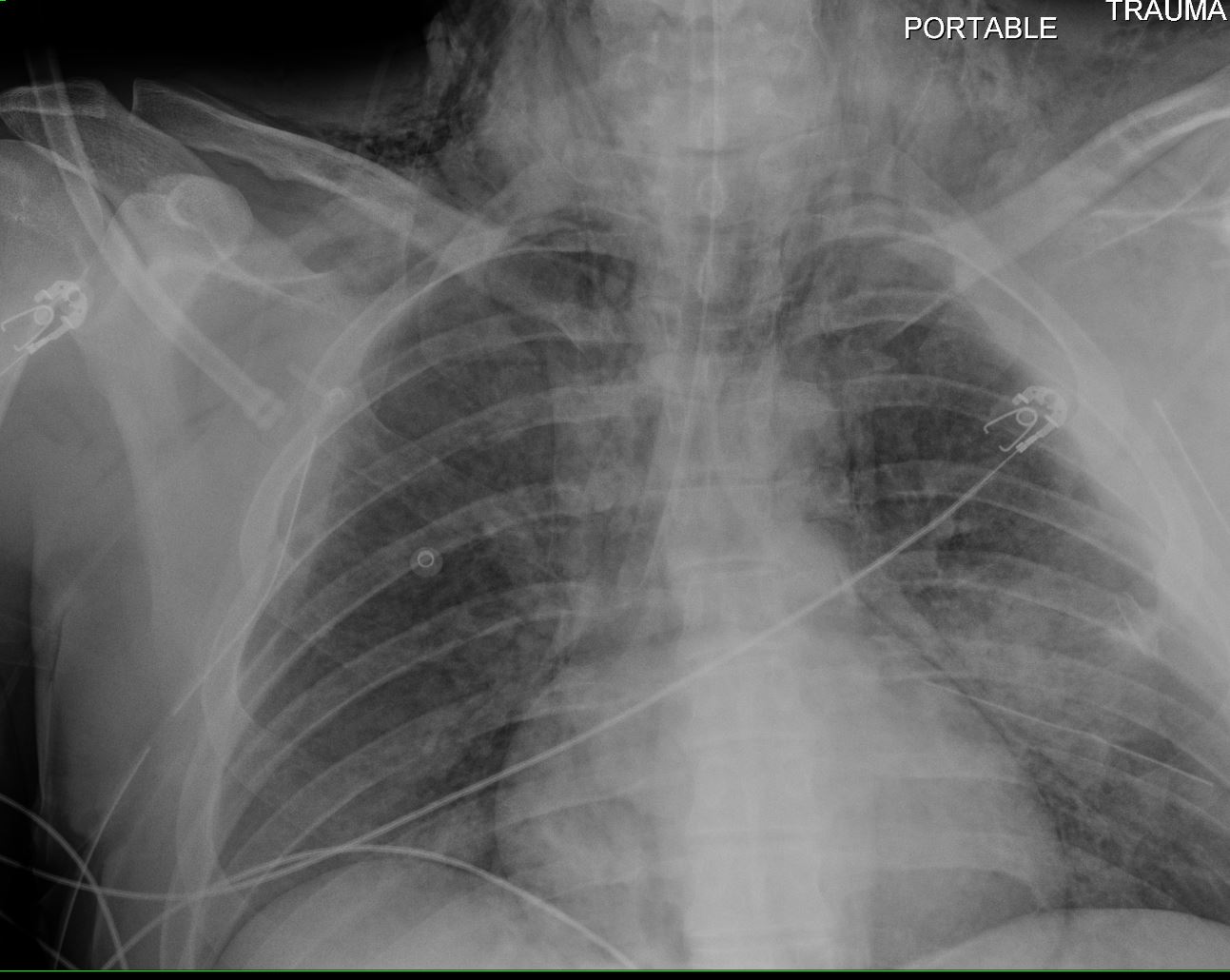
CXR shows left mid to lower lung infiltrate and left pleural soft tissue density. CT noted left sided rib fractures and a left scapular fracture, making the diagnosis of a lung contusion likely in this clinical context.
Ashley Davidoff MD TheCommonvein.net
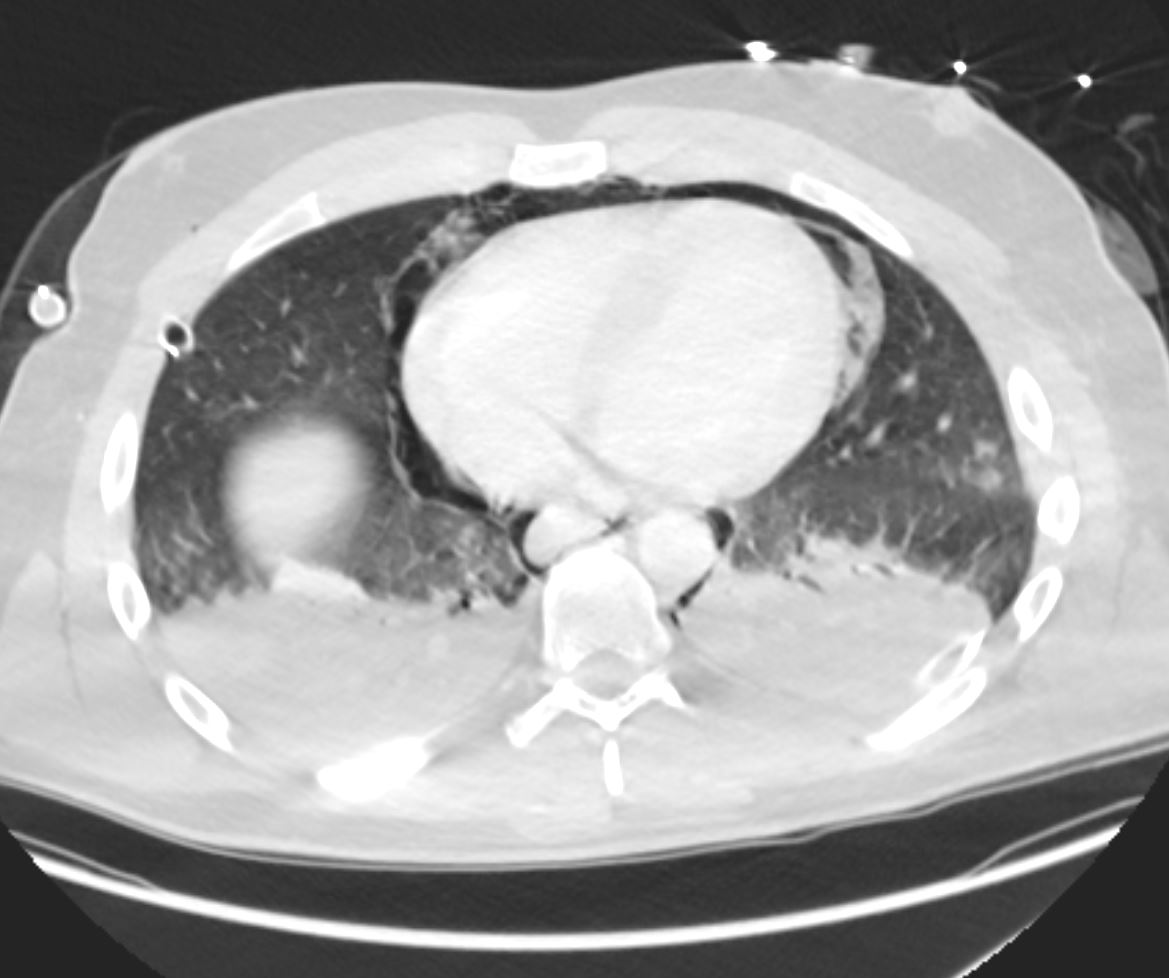
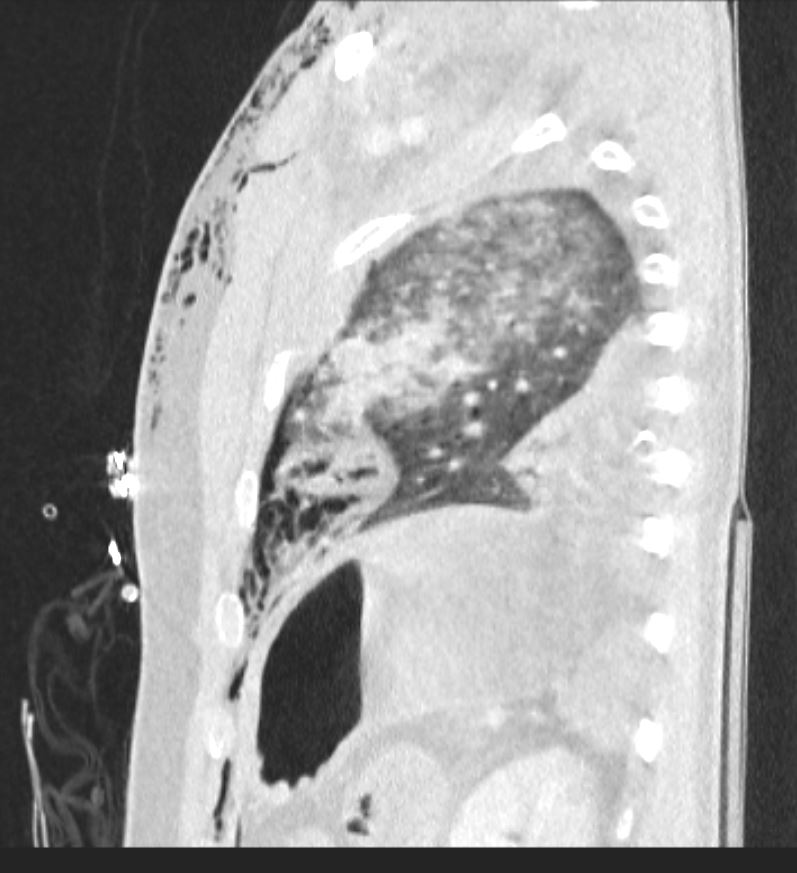
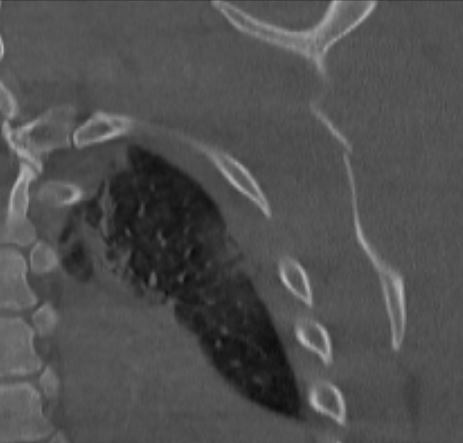
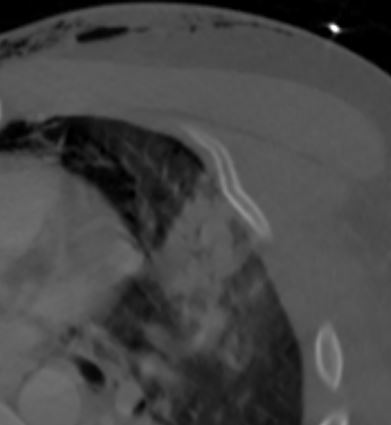
CT Pneumomediastinum
Air Along the Left and Right Heart Border
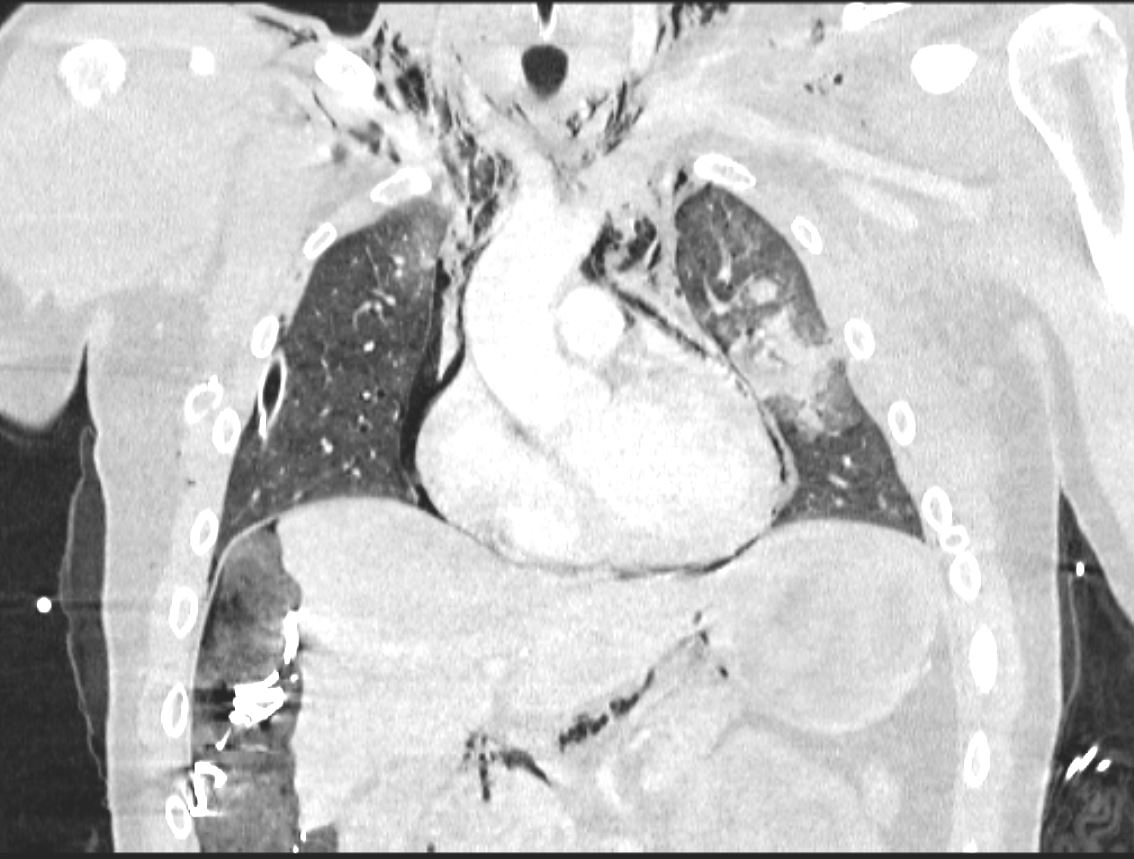
Air Along the Left and Right Heart Border
Coronal CT scan shows air surrounding the heart, but also in the gastrohepatic ligament and extensive accumulation in the soft tissues of the neck. The lung contusion is notes in the left mid chest. The patient has been to the OR and the changes alongside the liver are due to surgical packing
Ashley Davidoff MD TheCommonvein.net
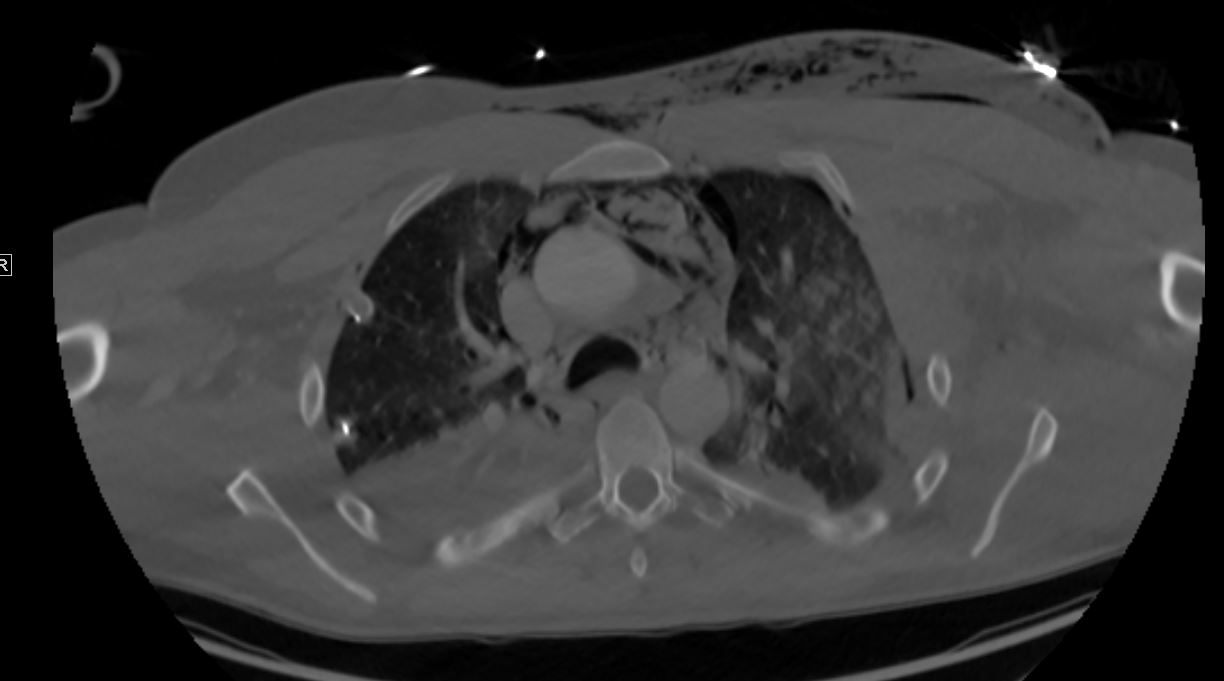
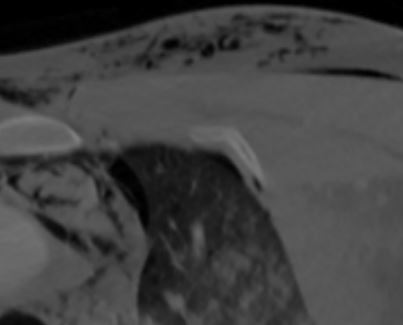
CT Pneumomediastinum
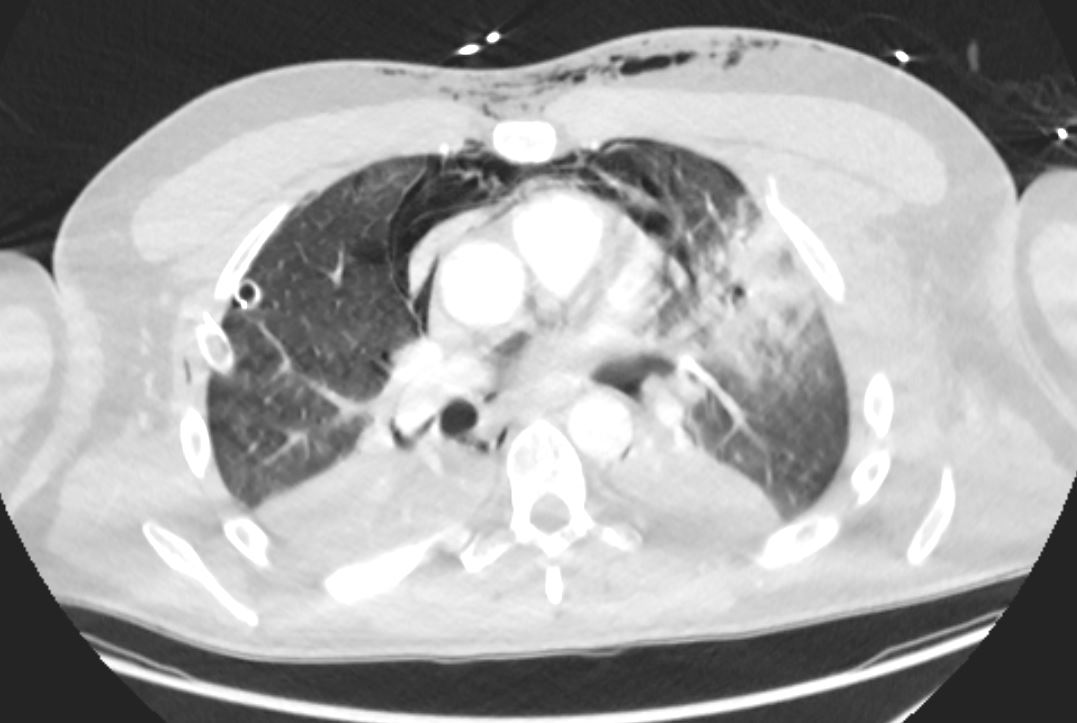
Air Around the Great vessels
Axial CT scan shows air surrounding the great vessels, and in the anterior mediastinal fat. The left upper lung contusion is associated with bibasilar atelectasis. A small amount of subcutaneous air is noted. The lung contusion is noted in the left upper lobe.
Ashley Davidoff MD TheCommonvein.net
1. Bilateral consolidative and groundglass pulmonary opacities, likely representing a combination of contusions and airspace disease, possibly due to aspiration. There is occlusion of the right lower lobe bronchus which may be due to intraluminal debris versus compression from adjacent consolidation.
2. Bilateral chest tubes with trace bilateral pneumothoraces.
3. Extensive diffuse mediastinal and subcutaneous emphysema in the anterior chest wall.
4. Postsurgical changes in the abdomen and pelvis with wound VAC in place. Small volume pneumoperitoneum is expected from recent surgery. No traumatic definite solid organ injury.
5. Substantial enhancement thickening of multiple loops of small bowel which may reflect shock bowel. Clinical correlation is recommended.
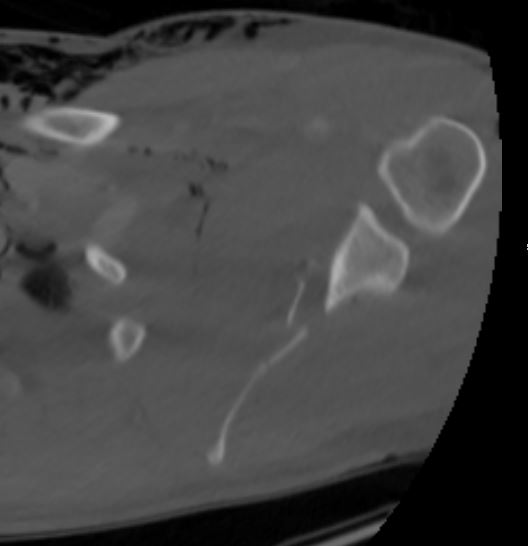
6. Acute fractures of the left scapula and left ribs 2 and 3.