
Normally the
Central Arteriole
1mm in diameter
(at the resolution of current CT scanners}
The Interlobular Septum is
.1mm and
should not be visualised normally
Normal Variations
Secondary Lobule in CHF
Varied Sizes and Shapes
Periphery vs Centrally
Tend to be a Paucity Posteriorly
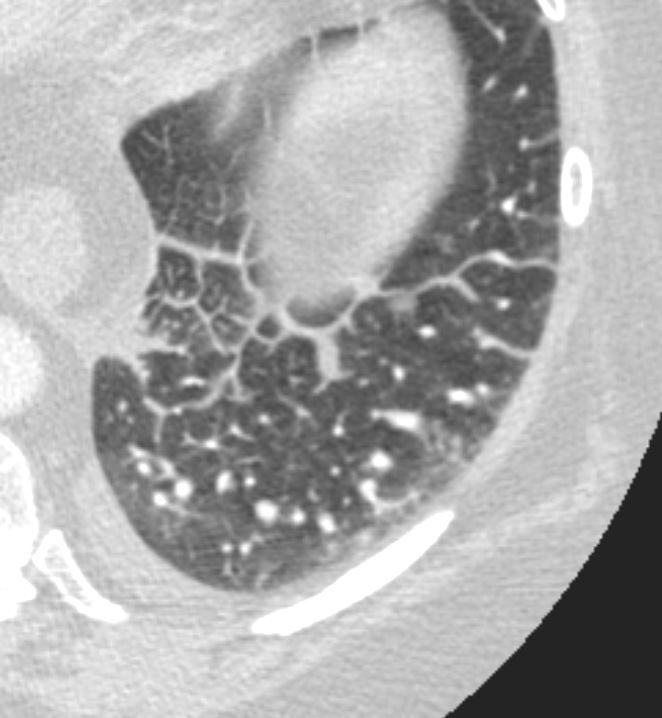
Axial CT in a patient with CHF demonstrates the heterogeneous morphology of the secondary lobule. In this patient the lobules in the periphery are larger than the centrally placed secondary lobules. In addition the peripheral lobules are more rectangular and those centrally are more of a polyhedral shape.
Ashley Davidoff MD TheCommonVein.net 135831
Small Peripheral Secondary Lobules and Varying Shapes Centrally
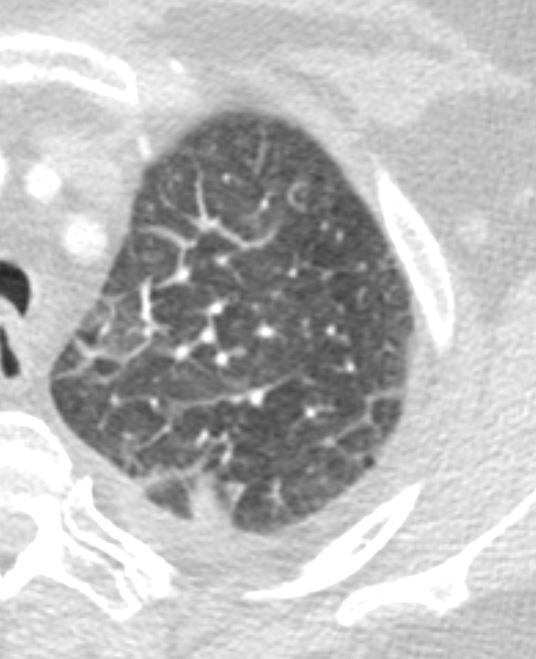
Axial CT in a patient with CHF demonstrates the heterogeneous morphology of the secondary lobule. In this patient the lobules in the periphery are smaller than the centrally placed secondary lobules. In addition the central lobules are more irregular in shape and are hexagonal or polygonal.. There is a small effusion.
Ashley Davidoff MD TheCommonVein.net 135834
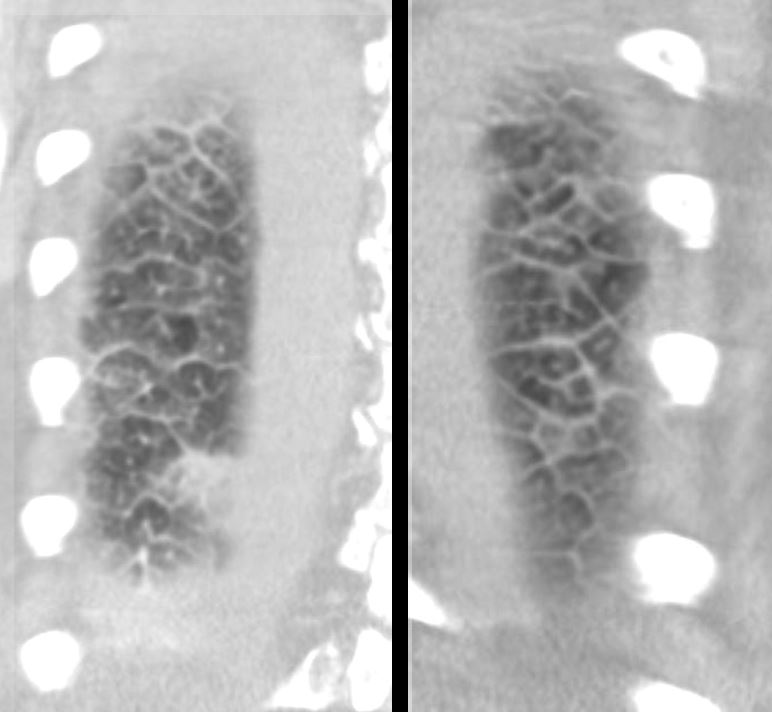
Coronal CT through the posterior chest in a patient with CHF demonstrates the heterogeneous morphology of the secondary lobule. There is a wide range of sizes and shapes, with wide variations of hexagonal and polygonal morphology. Some of the shapes are innate but consideration must be given to the orientation of the lobule and the varying angles we may catch them in a single plane of this technique.
Ashley Davidoff MD TheCommonVein.net 135832c
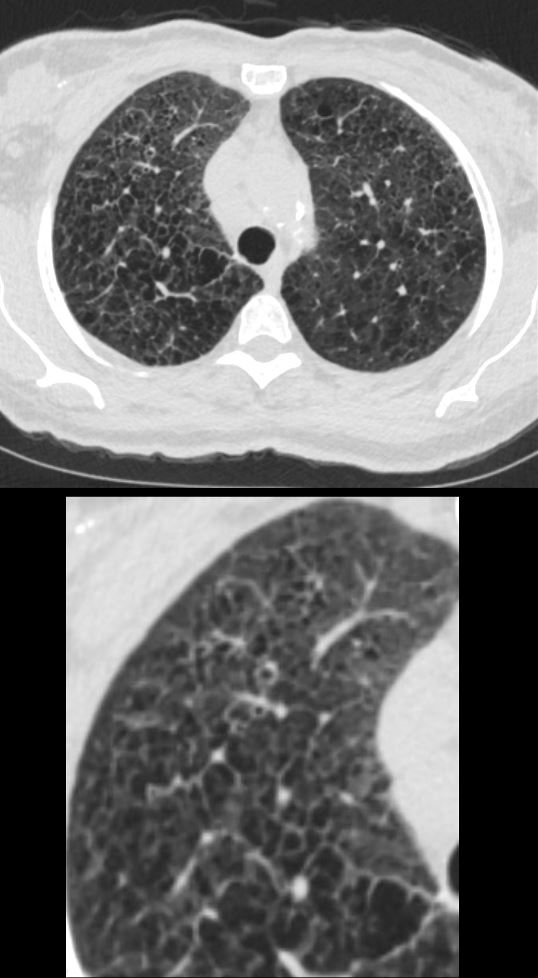
Expansion Due to Traction in Fibrotic NSIP
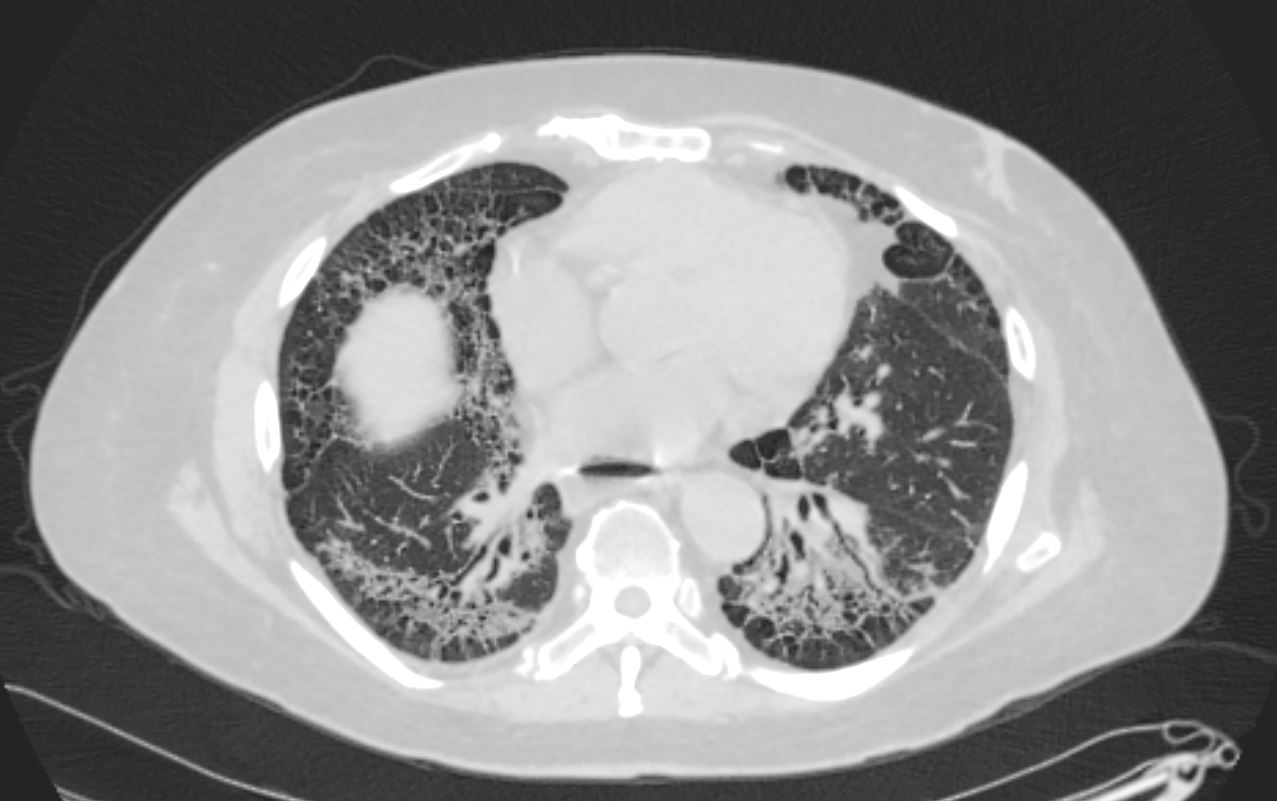
Axial CT shows peripheral reticular changes, ground glass, bronchiolectasis at both lung bases, volume loss with crowding of the bronchovascular bundles posteriorly and subpleural sparing posteriorly. Note air-fluid level in the distended esophagus.
Ashley Davidoff MD TheCommonVein.net 110Lu 136598
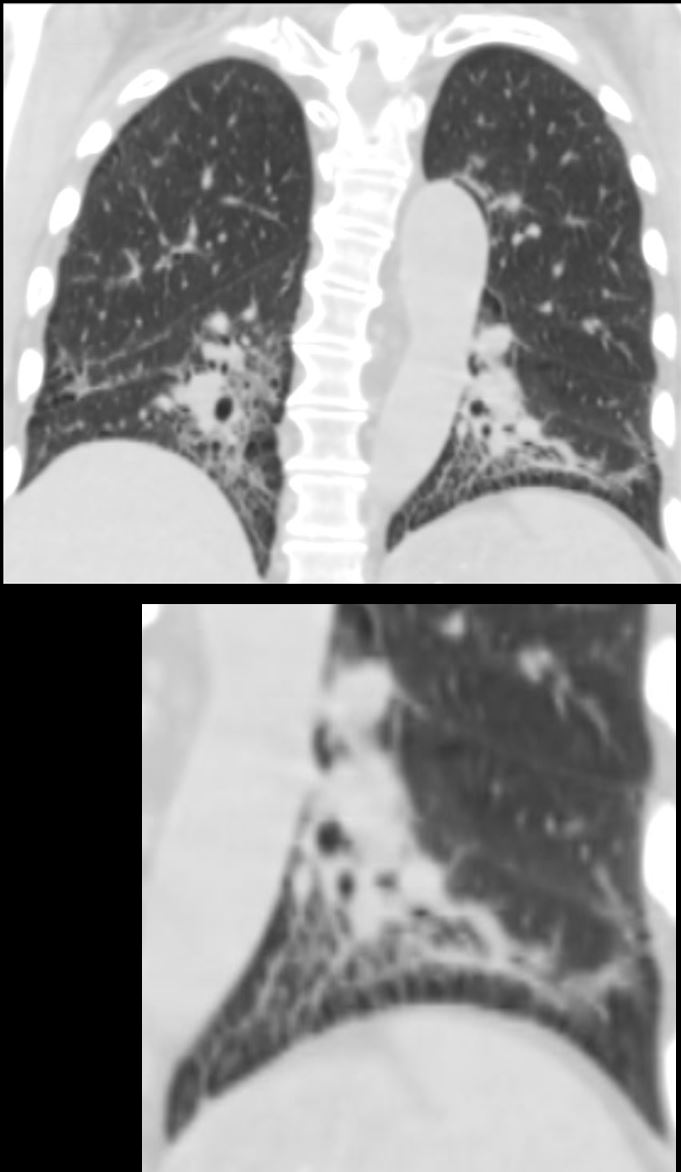
59-year-old male presents with history of scleroderma, Raynaud’s disease, and ILD
Coronal CT shows bibasilar volume loss, reticular change, ground glass changes, bronchovascular thickening , bronchiectasis, and subpleural sparing, all features characteristic of NSIP
.
The lower image highlights the bronchovascular thickening volume loss bronchiectasis and subpleural sparing. The fibrotic process has resulted in traction of the secondary lobules in the region of subpleural sparing
Ashley Davidoff MD TheCommonVein.net 110Lu 136592c01
Pulmonary Hemorrhage and Heterogeneous
Changes in the Secondary Lobules
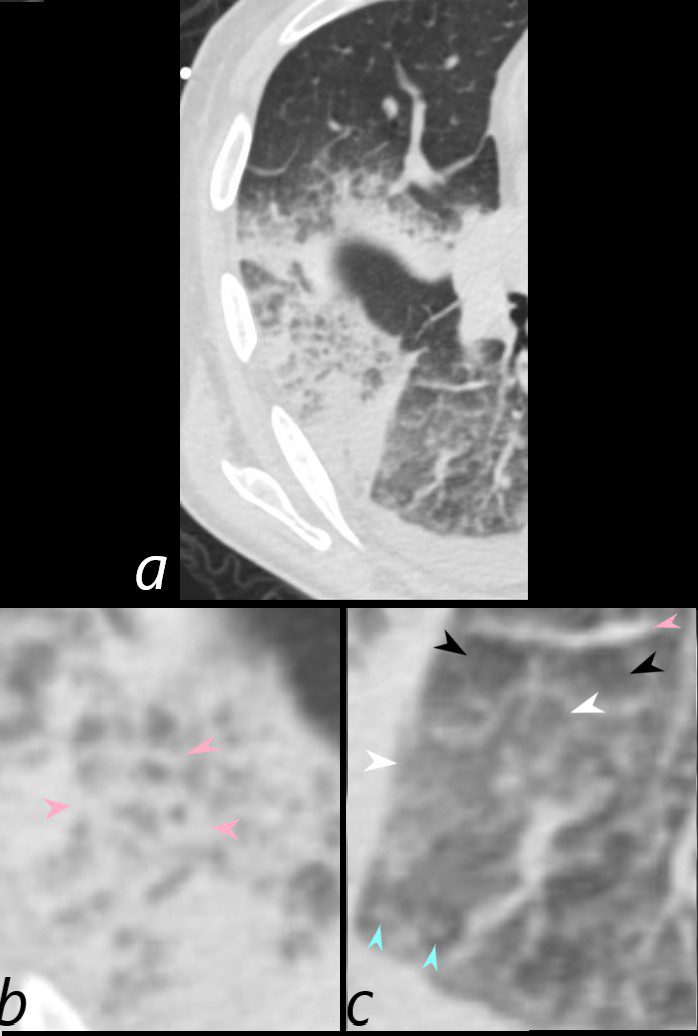
75-year-old man on blood thinners s/p aortic valve replacement, s/p trauma, presents with hemoptysis. He was afebrile and without an elevated white count
Axial CT at the level below the carina at the inferior aspect of the hematoma shows heterogenous changes of the secondary lobules. The changes in the post segment of the right upper lobe (b) show significantly thickened interlobular septa (pink arrowheads) and relatively small secondary lobules caused by the compression of the hematoma. The changes in the apical segment of the lower lobe (c) show a combination of secondary lobules with ground glass changes (white arrowheads) some normal or with mosaic attenuation (black arrowheads), some showing mildly thickened smooth interlobular septa (pink arrowheads), and others revealing centrilobular nodules (teal arrowheads).
There is a right sided effusion
Ashley Davidoff MD TheCommonVein.net 165Lu 135853cL
Desquamative Interstitial Pneumonia
Diffuse Ground Glass Changes in the Upper Lobes
Small Secondary Lobules and Some Centrilobular Nodules
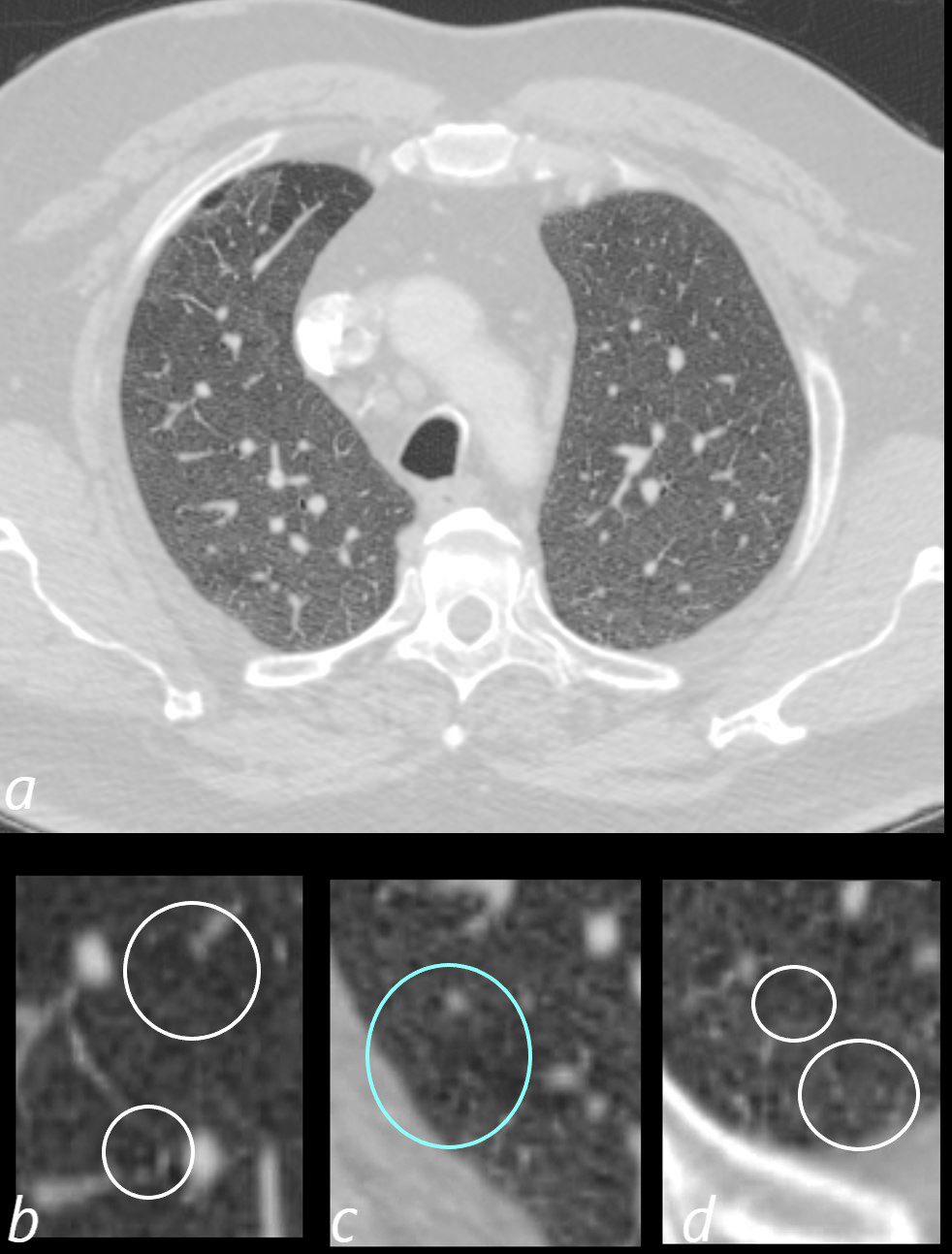
60-year-old male smoker with a history of progressive dyspnea. Axial CT through the upper lung fields shows diffuse ground glass changes with minimal heterogeneity. The secondary lobules appear relatively small with slightly thickened septa and some have prominent centrilobular nodules (b and c within the white rings) suggesting small airway disease Part of the anterior segment of the right upper lobe is spared.
Pathology confirmed a diagnosis of DIP
Ashley Davidoff MD TheCommonVein.net 253Lu 136004cL
Small
Large Cancer
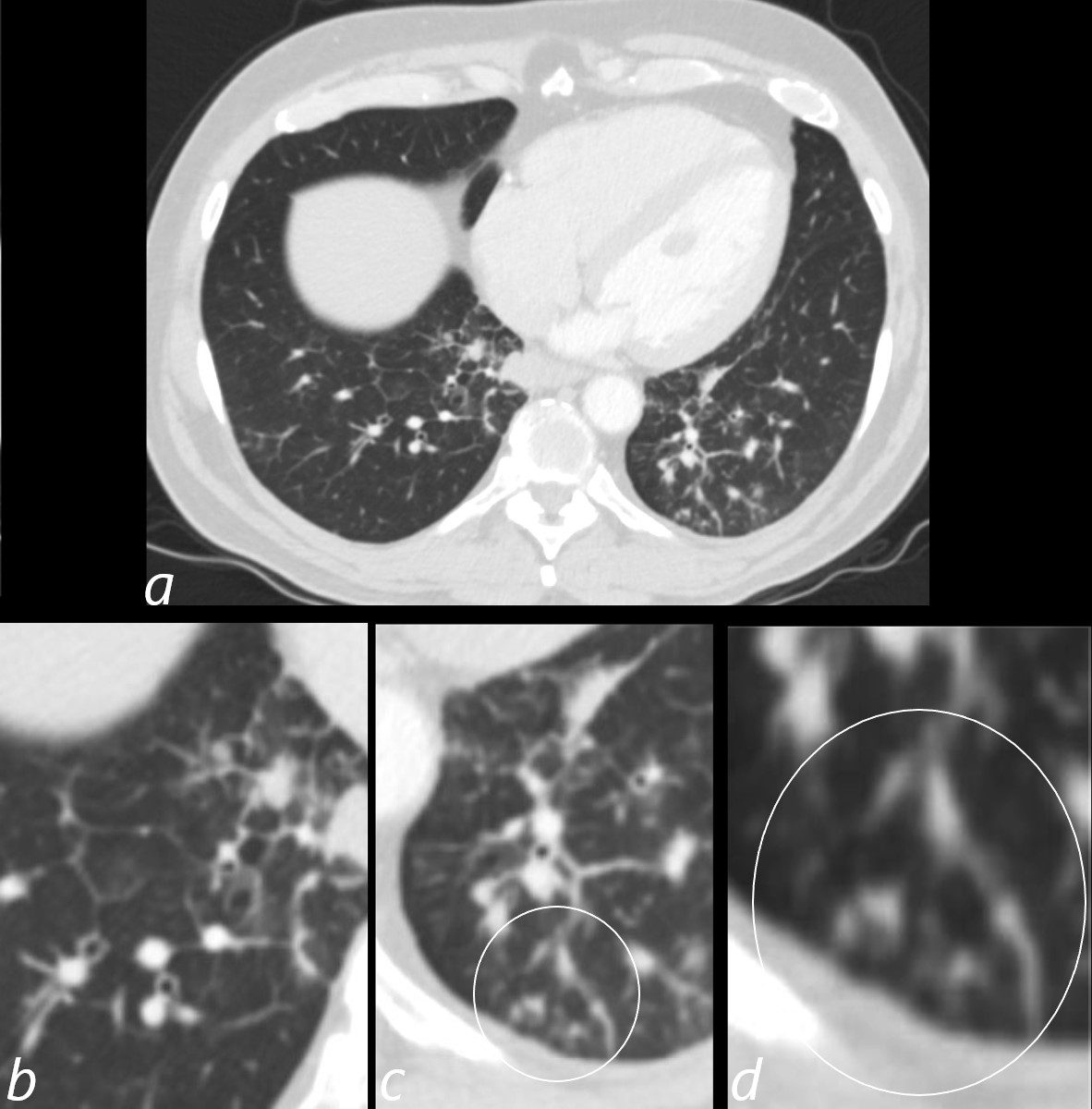
3 months later the patient presented with chest pain and a cough. CT of the chest in the axial plane shows new bilateral lower lobar regions of irregular interlobular septal thickening noted in the right lower lobe a, magnified in b). Ringed in image c and d are 2 side by side secondary lobules with irregular septal thickening centrilobular nodules and other intralobular nodules likely reflecting lymphatic involvement.
Given the changes in the right upper lobe these findings likely reflect lymphangitis carcinomatosa
Ashley Davidoff MD TheCommonVein.net 013Lu 136062cL
51-year-old female smoker with a history of COPD asthma and pulmonary hypertension presents with progressive dyspnea. Axial CT through the upper lung fields shows extensive changes of centrilobular emphysema associated with peribronchial thickening noted in the right upper lobe Path confirmed diagnosis of DIP
Ashley Davidoff MD TheCommonVein.net 252Lu 135961c