
62-year-old female presents with acute dyspnea and chest pain
“White Out” Left Chest
62-year-old female presents with acute dyspnea and chest pain
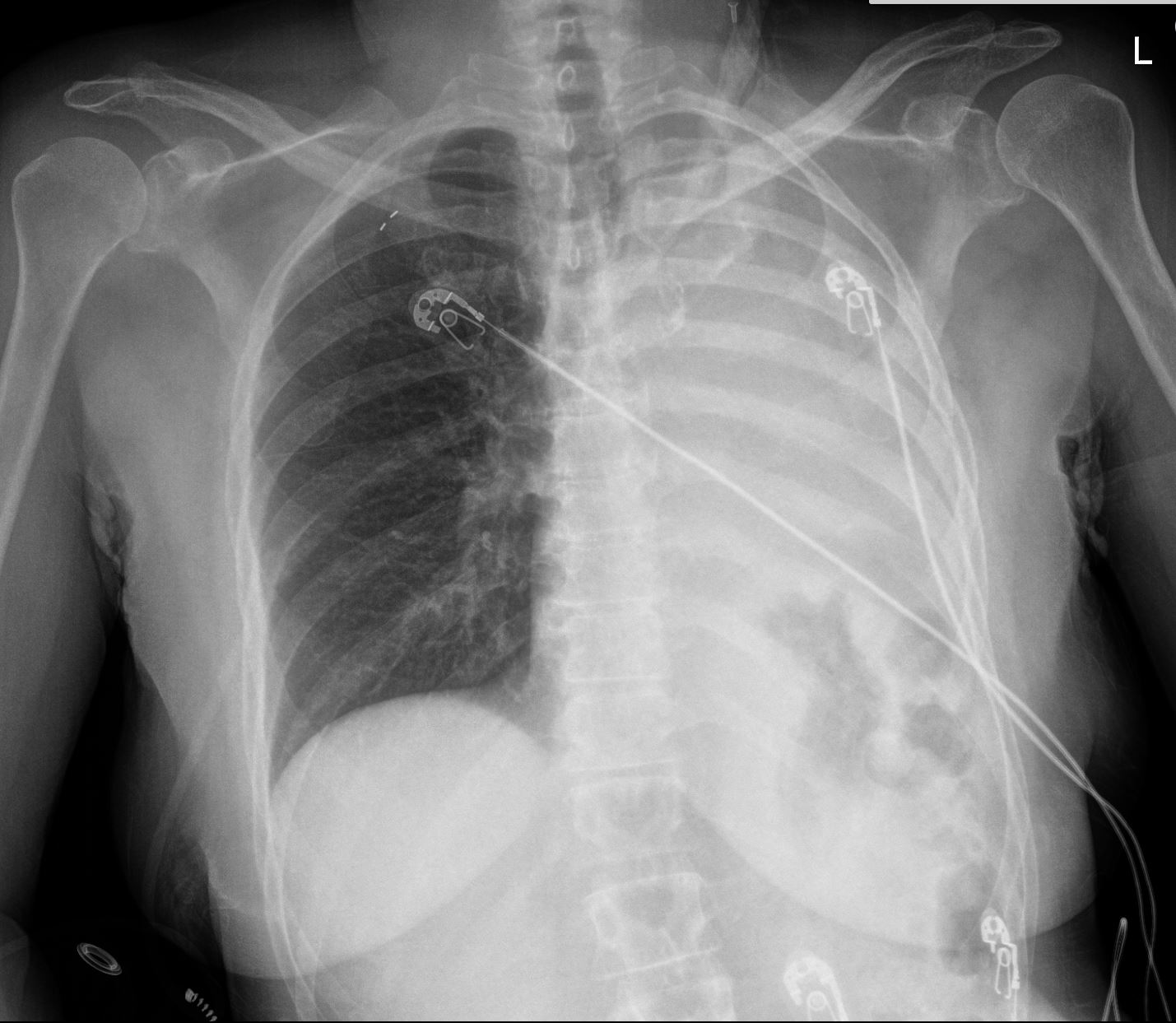
Frontal CXR shows a “white out” of the left hemithorax. The left hemidiaphragm is elevated and there is leftward mediastinal shift indicating volume loss
She was subsequently diagnosed with a small cell lung carcinoma that was obstructing the left main stem bronchus
Ashley Davidoff MD TheCommonVein.net 298Lu 136700
62-year-old female presents with acute dyspnea and chest pain
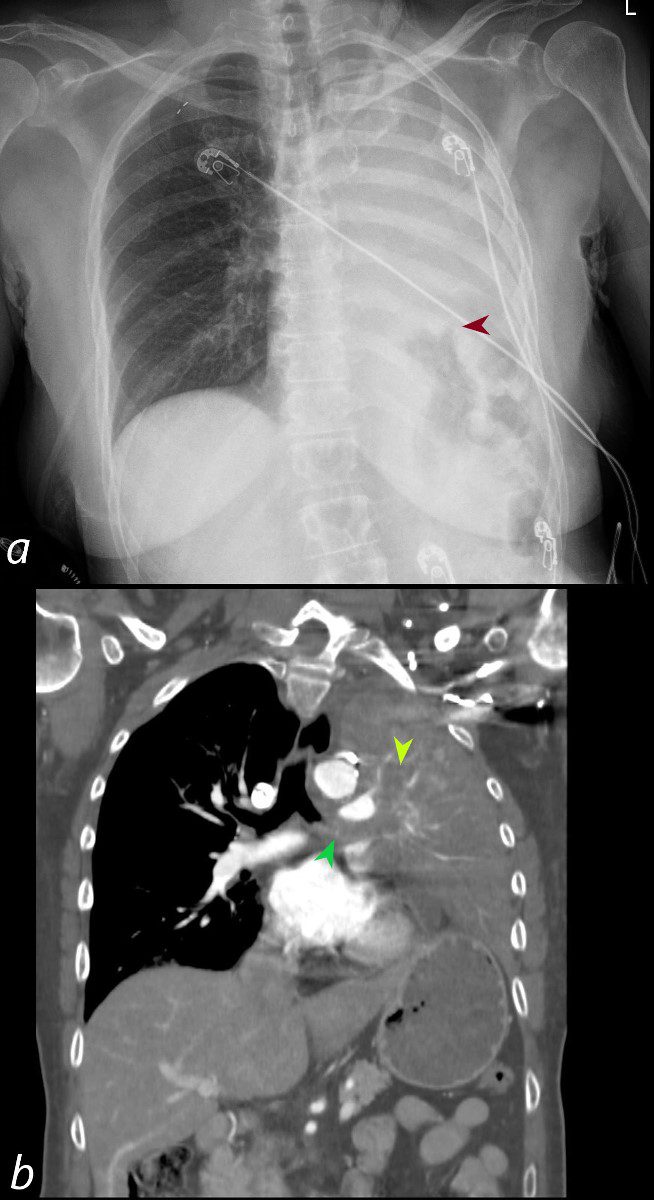
Frontal CXR shows a “white out” of the left hemithorax. The left hemidiaphragm is elevated (maroon arrowhead) and there is leftward mediastinal shift indicating volume loss.
Coronal CT confirms the presence of an obstructing lesion in the left mainstem bronchus,(b, dark green arrowhead), with extension of the soft tissue into an upper lobe bronchus (b light green arrowhead). There is total collapse of the left lung and an elevated left hemidiaphragm
Subsequent pathological diagnosis of small cell lung carcinoma was established
Ashley Davidoff MD TheCommonVein.net 298Lu 136702
62-year-old female presents with acute dyspnea and chest pain
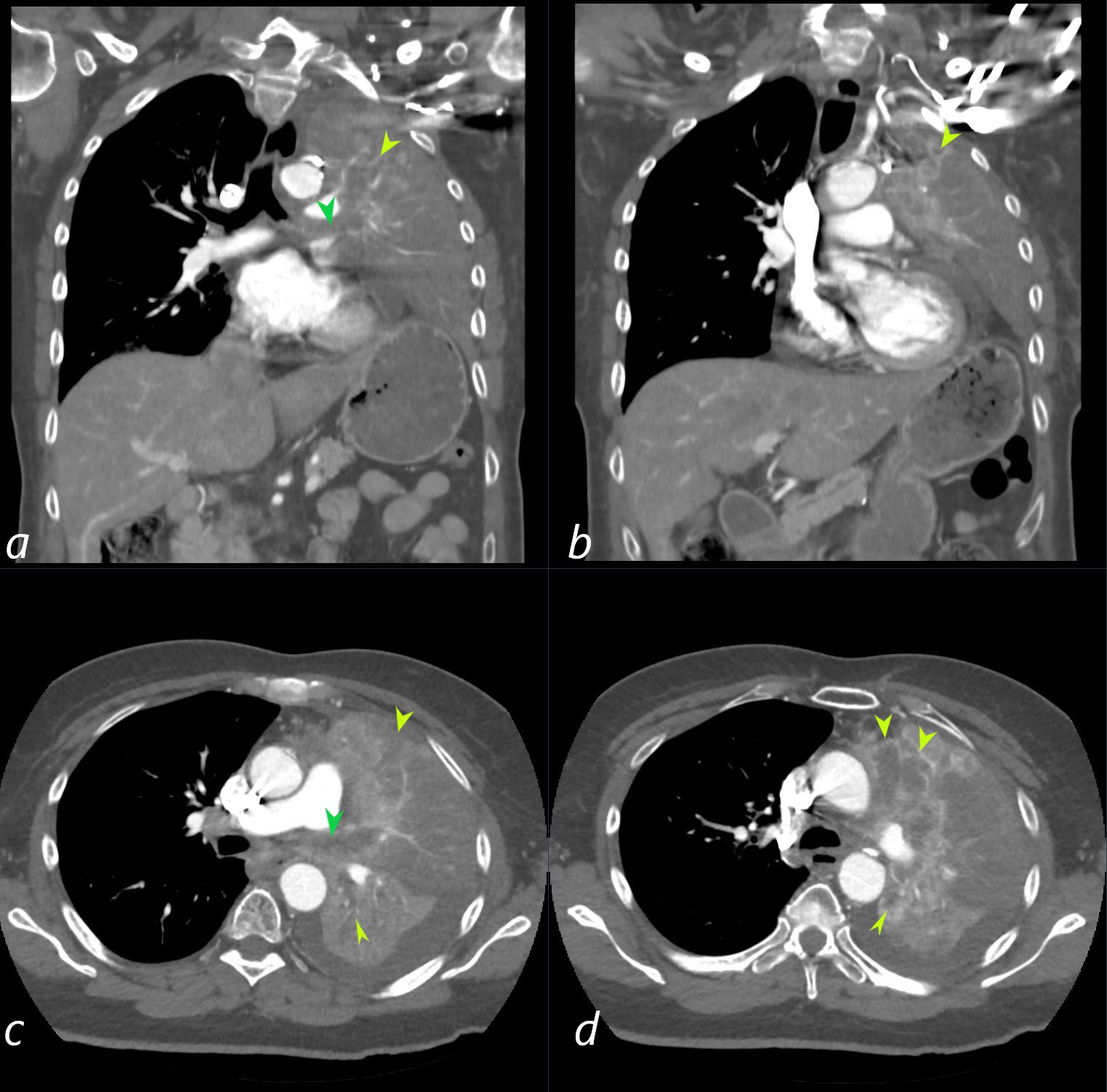
Coronal CT confirms the presence of an obstructing lesion in the left mainstem bronchus, (dark green arrowhead, a), with extension of the soft tissue into bronchiectatic upper lobe bronchi (light green arrowheads b, c, d) There is total collapse of the left lung.
Subsequent pathological diagnosis of small cell lung carcinoma was established
Ashley Davidoff MD TheCommonVein.net 298Lu 136704
62-year-old female presents with acute dyspnea and chest pain
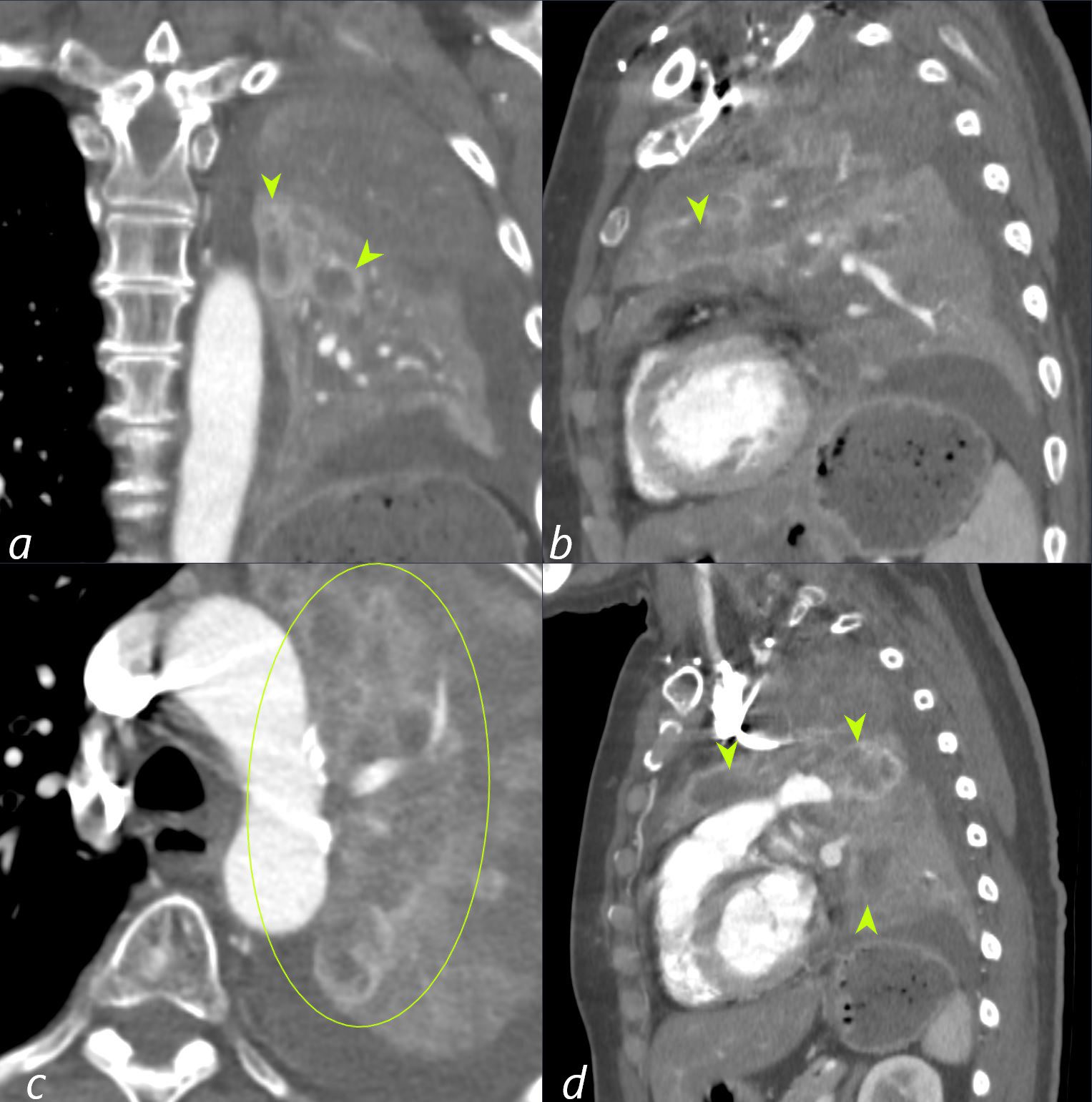
Coronal CT shows inspissation and bronchiectasis of the left upper lobe segmental an subsegmental airways (green arrowheads and ringed in green) likely due to extension of the the central small cell cancer. There is total collapse of the left lung.
Subsequent pathological diagnosis of small cell lung carcinoma was established
Ashley Davidoff MD TheCommonVein.net 298Lu 136706
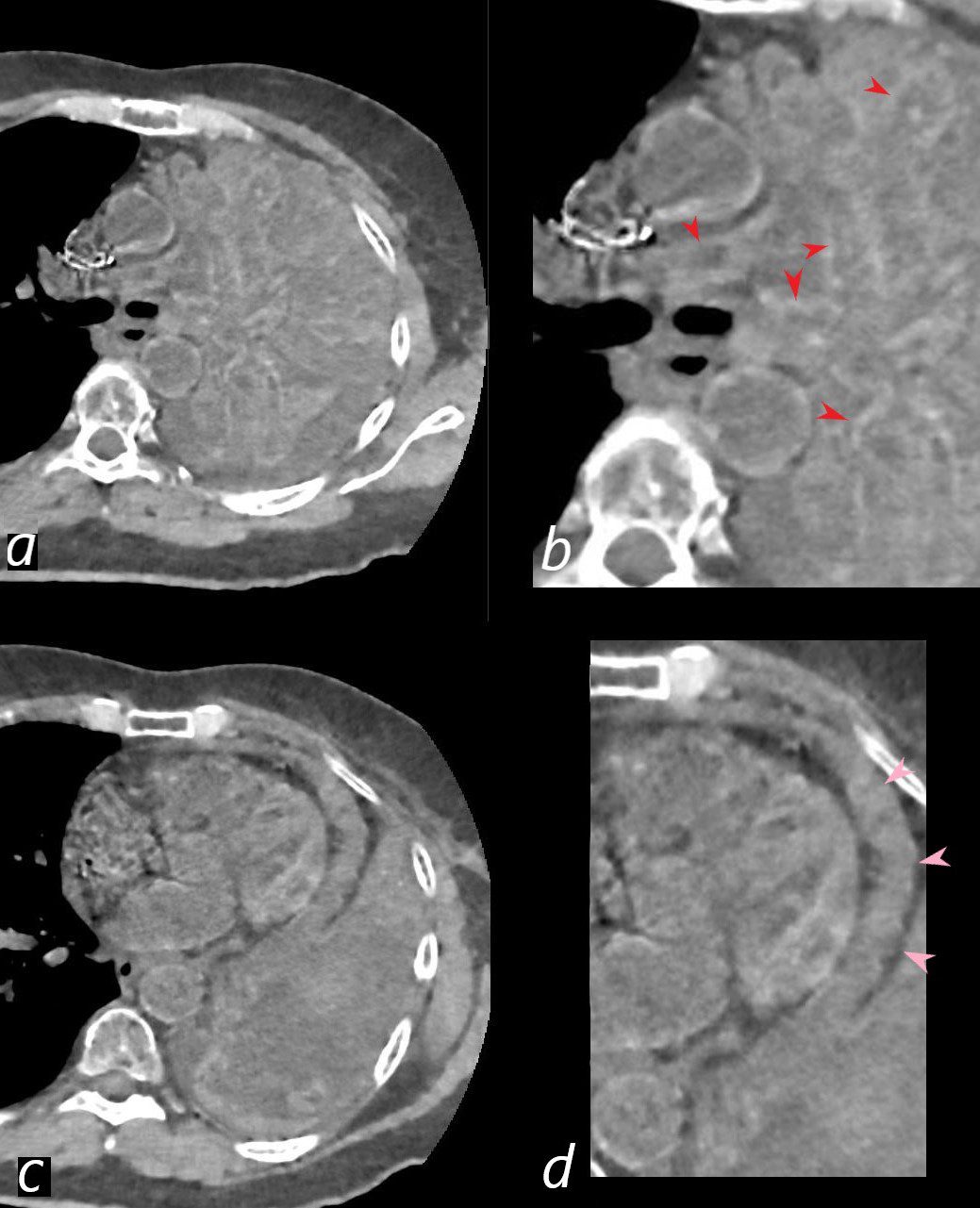
62-year-old female presents with acute dyspnea and chest pain
Dual energy CT shows enhancement of the walls of the impacted bronchiectatic walls (red arrowheads b) but without enhancement of the pericardium with known malignant effusion.
Ashley Davidoff MD TheCommonVein.net 298Lu 136709
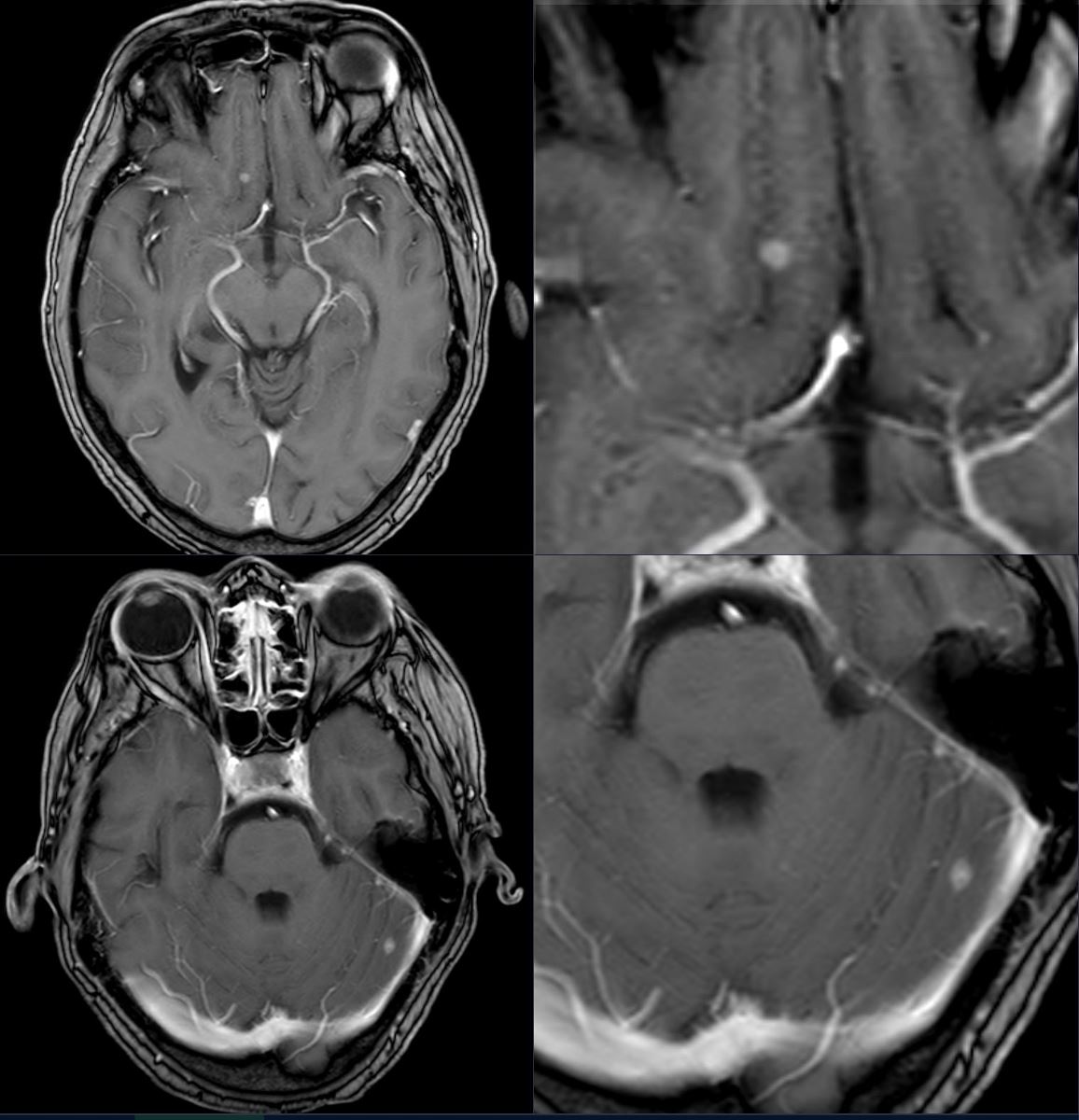
T1 weighted MRI images of the brain following contrast administration show small enhancing lesions in the right frontal lobe and the left cerebellar hemisphere
Ashley Davidoff MD TheCommonVein.net 298Lu 136711
1 Month Later Presents with Ongoing Dyspnea
62-year-old female presents with acute dyspnea and chest pain
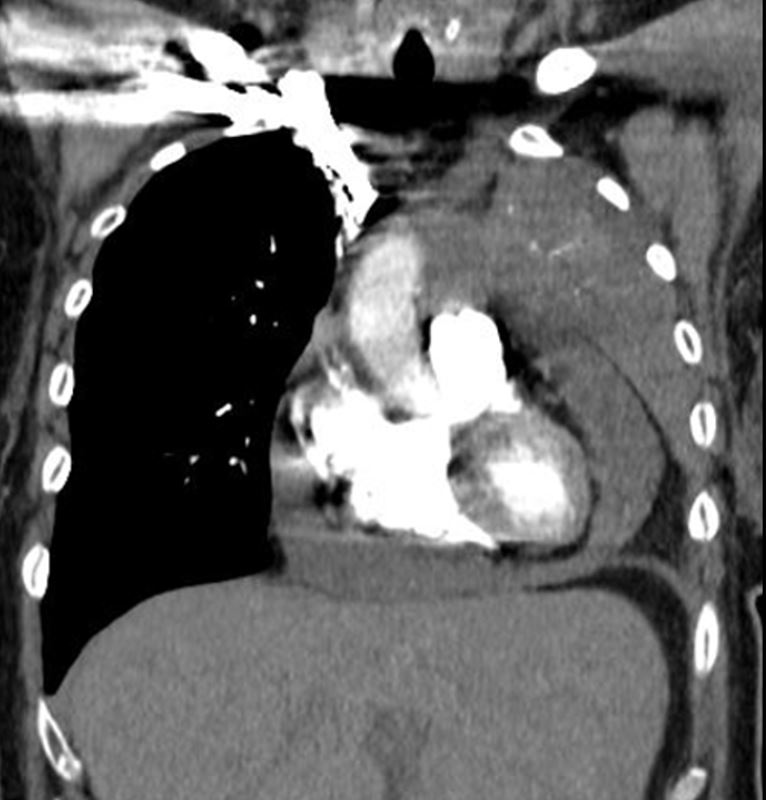
CT in the coronal plane shows a small to moderate pericardial effusion and left lung collapse
Echocardiogram revealed increased right sided pressures but no “frank” tamponade, and was subsequently drained
Ashley Davidoff MD TheCommonVein.net 298Lu 136724
62-year-old female presents with acute dyspnea and chest pain
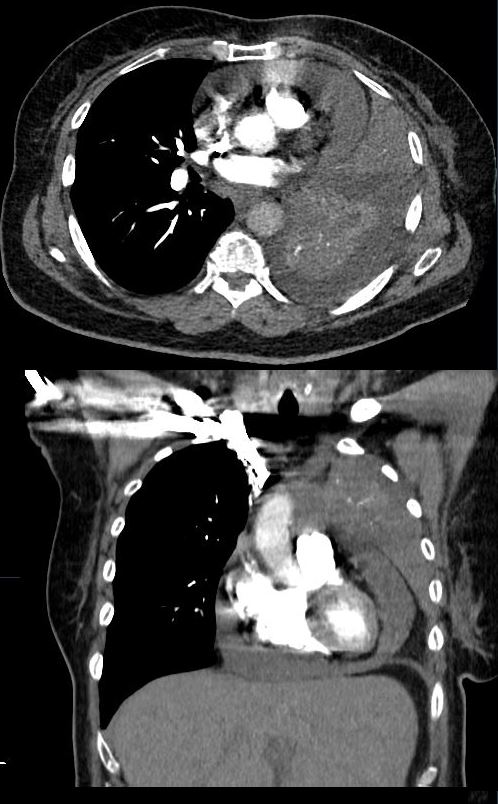
CT in the axial and coronal plane shows a small to moderate pericardial effusion, left lung collapse and small pleural effusion.
Echocardiogram revealed increased right sided pressures but no “frank” tamponade, and was subsequently drained
Ashley Davidoff MD TheCommonVein.net 298Lu 136725
62-year-old female presents with acute dyspnea and chest pain
CT in the axial and coronal plane shows a small to moderate pericardial effusion, left lung collapse and small pleural effusion.
Echocardiogram revealed increased right sided pressures but no “frank” tamponade, and was subsequently drained
Ashley Davidoff MD TheCommonVein.net 298Lu 136728
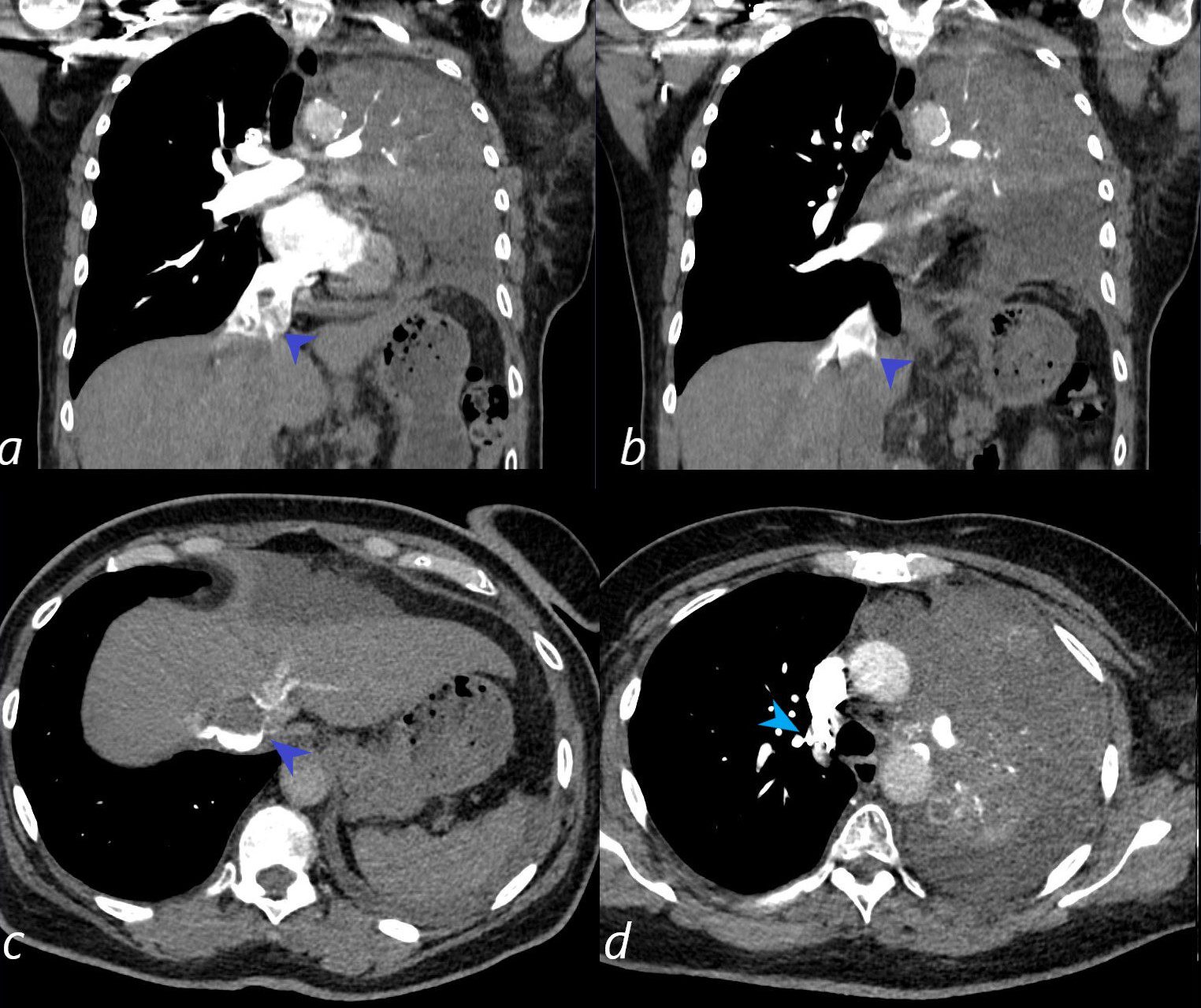
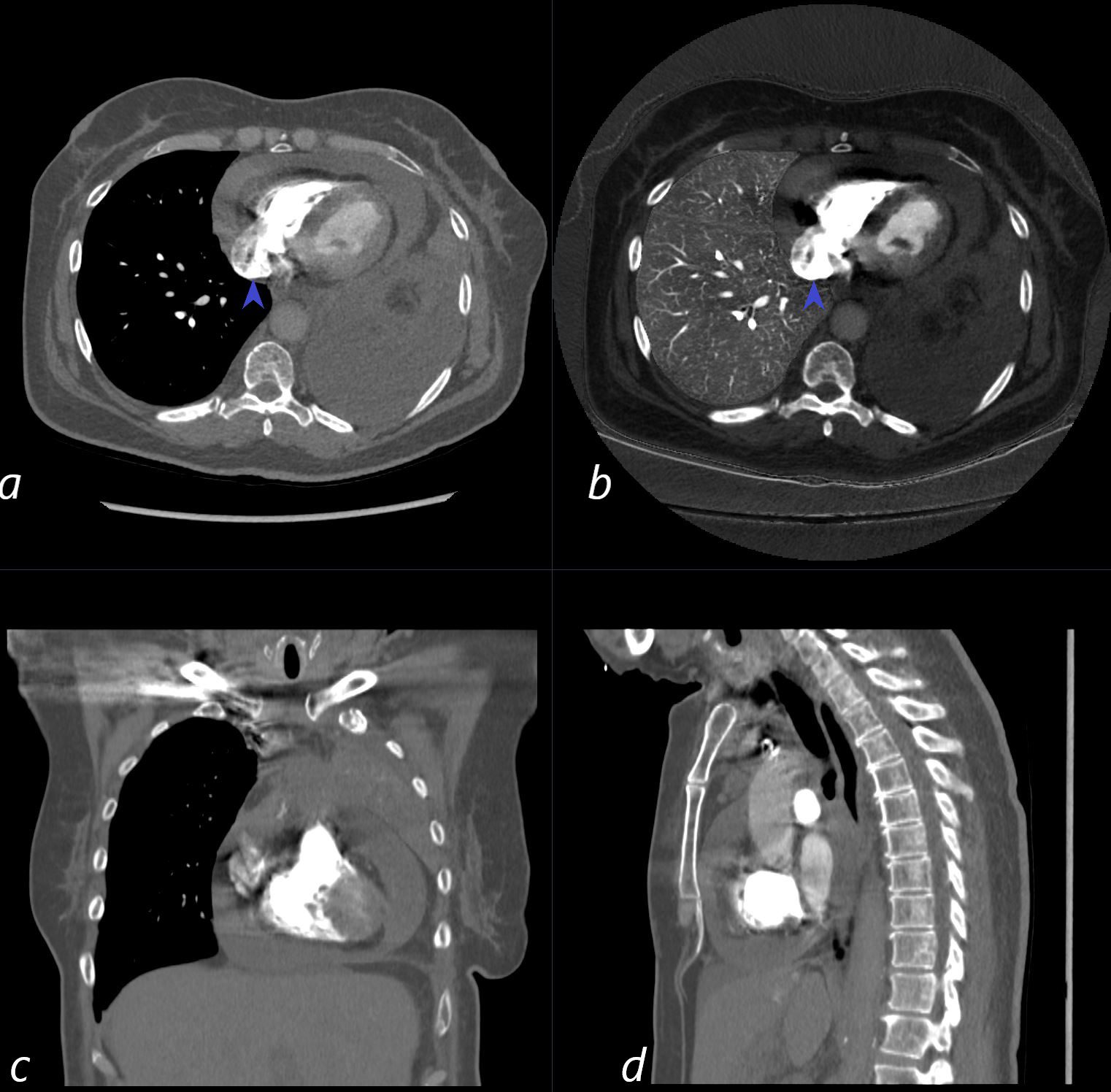
62-year-old female presents with acute dyspnea and chest pain
CT in the coronal and axial planes shows a small to moderate pericardial effusion, left lung collapse and small left pleural effusion.
There is evidence of elevated pressures in the right side of the heart, characterized by an enlarged IVC (3.1cms) with reflux into the hepatic veins (dark blue arrowheads , a, b, c) and reflux of contrast into the azygous vein (light blue arrowhead (d) A contrast blood level in the IVC in image c, further indicates slow flow in the IVC. tamponade would be on the differential diagnosis in this case and an echo is warranted for evaluation.
Echocardiogram revealed increased right sided pressures but no “frank” tamponade. The pericardial fluid was subsequently drained and was positive for malignant cells
Ashley Davidoff MD TheCommonVein.net 298Lu 136730

62-year-old female presents with acute dyspnea and chest pain
Frontal CXR shows a “white out” of the left hemithorax
She was subsequently diagnosed with a small cell lung carcinoma that was obstructing the left main stem bronchus
Ashley Davidoff MD TheCommonVein.net 298Lu 136714
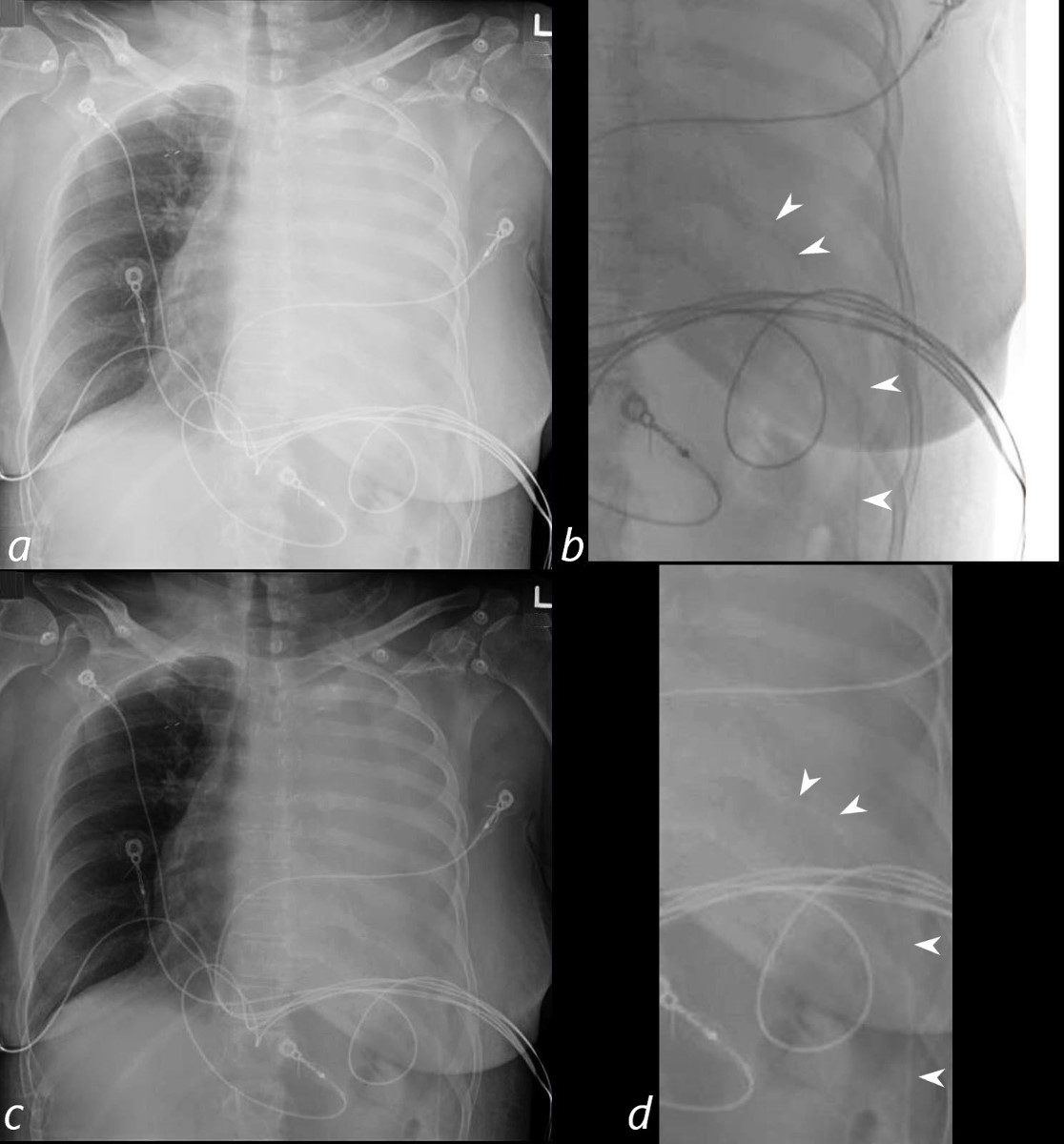
Frontal CXR shows a “white out” of the left hemithorax
Echocardiogram revealed a moderate effusion with elevated right sided pressures, but without “frank” tamponade. It was elected to perform a pericardiocentesis. The frontal CXR faintly reveals the pericardial catheter entering from the LUQ and overlies the expected location of the cardiac shadow.
Ashley Davidoff MD TheCommonVein.net 298Lu 136715cL
62-year-old female presents with acute dyspnea and chest pain
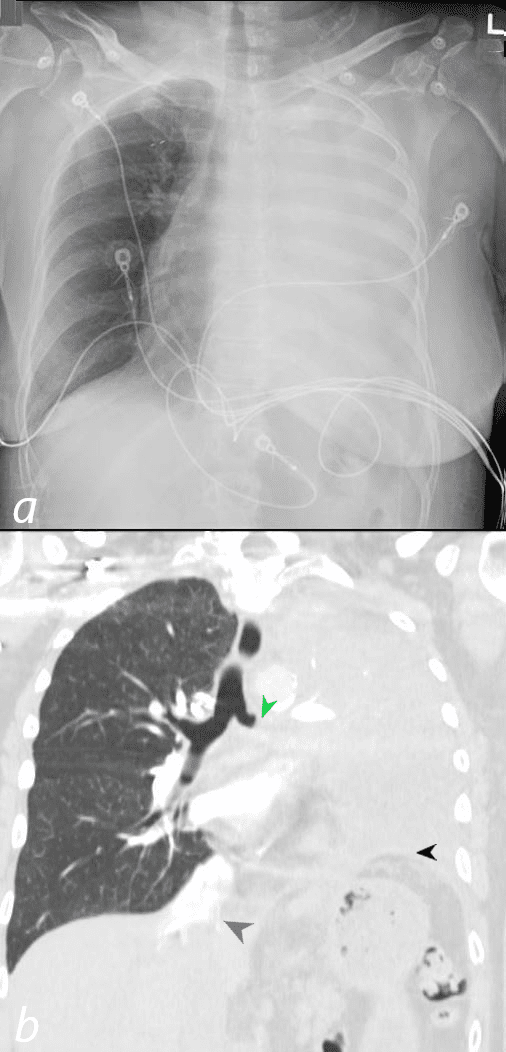
Frontal CXR shows a “white out” of the left hemithorax
The corresponding coronal CT shows an abrupt occlusion of the left mainstem bronchus (green arrowhead, b), total collapse of the left lung with an elevated left hemidiaphragm (black arrowhead) and a dilated IVC with reflux into the hepatic veins (blue arrowhead)
She was subsequently diagnosed with a small cell lung carcinoma that was obstructing the left main stem bronchus, and a presumed malignant pericardial effusion with suggestion of tamponade based on the findings of a dilated IVC with reflux
Ashley Davidoff MD TheCommonVein.net 298Lu 136721
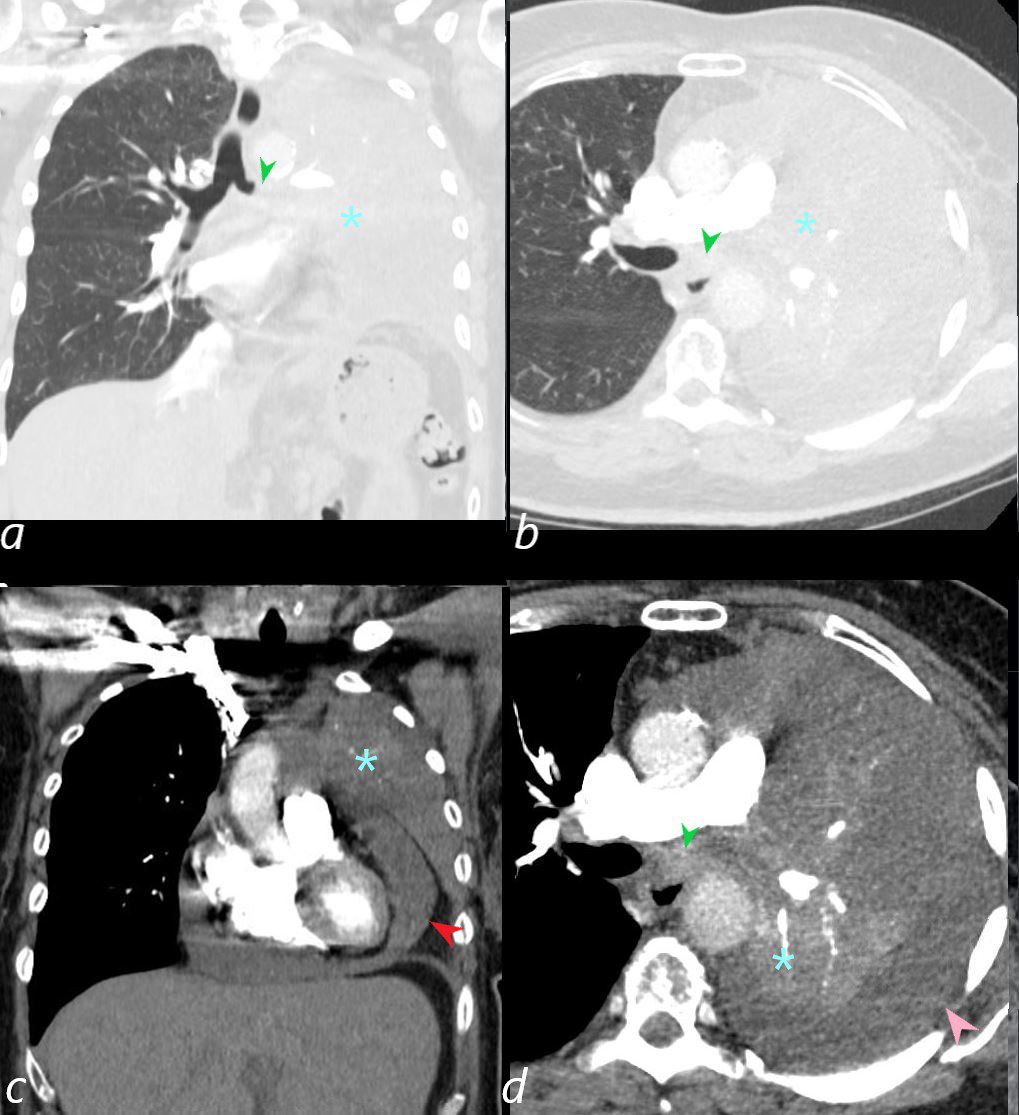
62-year-old female presents with acute dyspnea and chest pain
CT in the coronal plane (a,c) and axial plane (b,d) show an abrubt occlusion of the left mainstem bronchus (green arrowhead, a, b), total collapse of the left lung (teal asterisks), a small to moderate malignant pericardial effusion (red arrowhead, c), and a small left effusion (pink arrowhead, d)
Echocardiogram revealed increased right sided pressures but no “frank” tamponade, and was subsequently drained
Ashley Davidoff MD TheCommonVein.net 298Lu 136723
The IVC is dilated with blunted respirophasic variation c/w elevated RA
pressure. Unable to estimate PA systolic pressure owing to inadequate TR jet.
5. There is a circumferential pericardial effusion that is moderate overlying
the RV free wall (14 mm), the anterior wall (18 mm) and the apex (19 mm) and
small inferolaterally (4 mm). There is echodense material measuring up to 10
mm that is adherent to the RV and LV free walls and apex, c/w thrombus or
organized fibrinous material. Variation in transvalvular flow velocities could
not be accurately assessed owing to fusion of E and A waves during
tachycardia. There is late diastolic RV inversion noted without overt chamber
collapse. These findings are c/w elevated intrapericardial pressures without
overt tamponade – clinical correlation is warranted.
3 mm enhancing nodule within the medial aspect of the right frontal lobe (series 803, image 148) previously measuring 2 mm on
-6 mm enhancing nodule within the left cerebellar hemisphere
Post procedure there is a residual minimal pericardial effusion (trace) with
decreased HR to 81 and resolution of RA inversion.
PERICARDIAL FLUID:
POSITIVE FOR MALIGNANCY, CONSISTENT WITH METASTATIC SMALL CELL CARCINOMA FROM KNOWN LUNG PRIMARY.
A CELL BLOCK WAS USED FOR THE FINAL INTERPRETATION OF THIS CASE.
NOTE: Immunostains for calretinin and INSM1 reviewed and support the above diagnosis.