

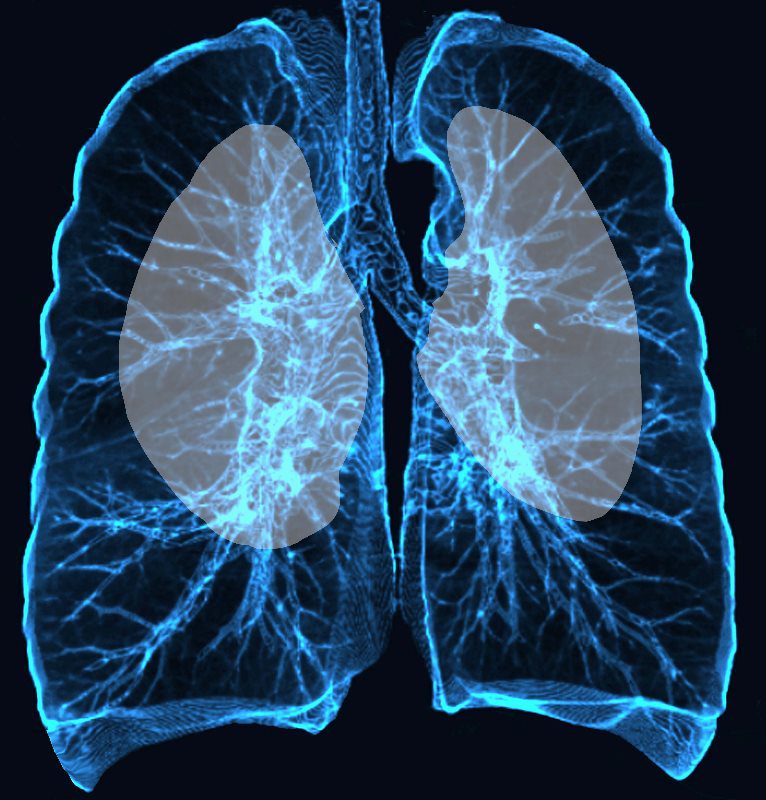
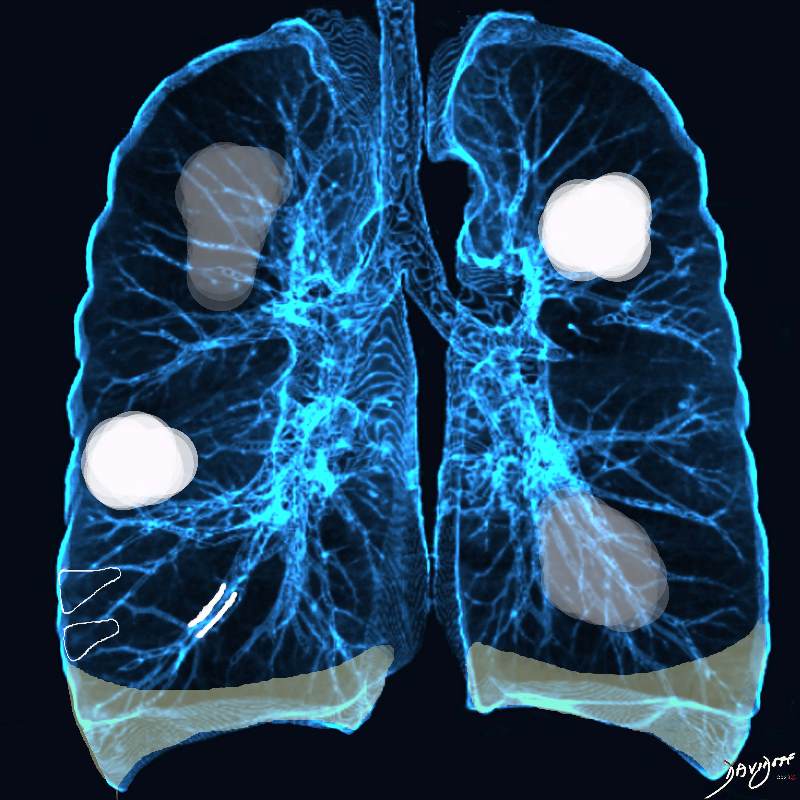
Upper lung field distribution
Ashley Davidoff MD TheCommonvein.net lungs-0774

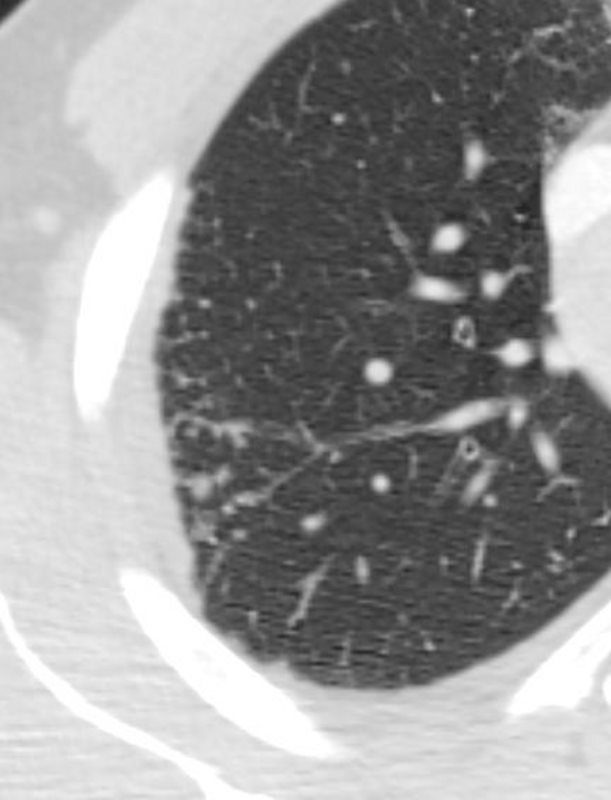
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows bilateral peripheral consolidations in the upper lobes
Ashley Davidoff MD The CommonVein.net lungs-0775e
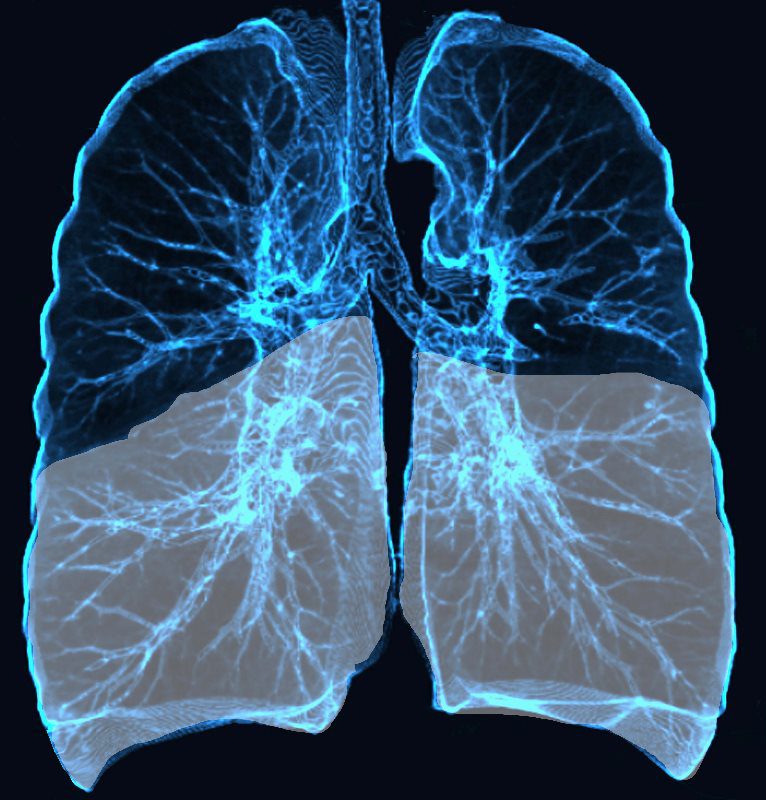
Lower Lobe distribution
Ashley Davidoff MD TheCommonvein.net lungs-0771
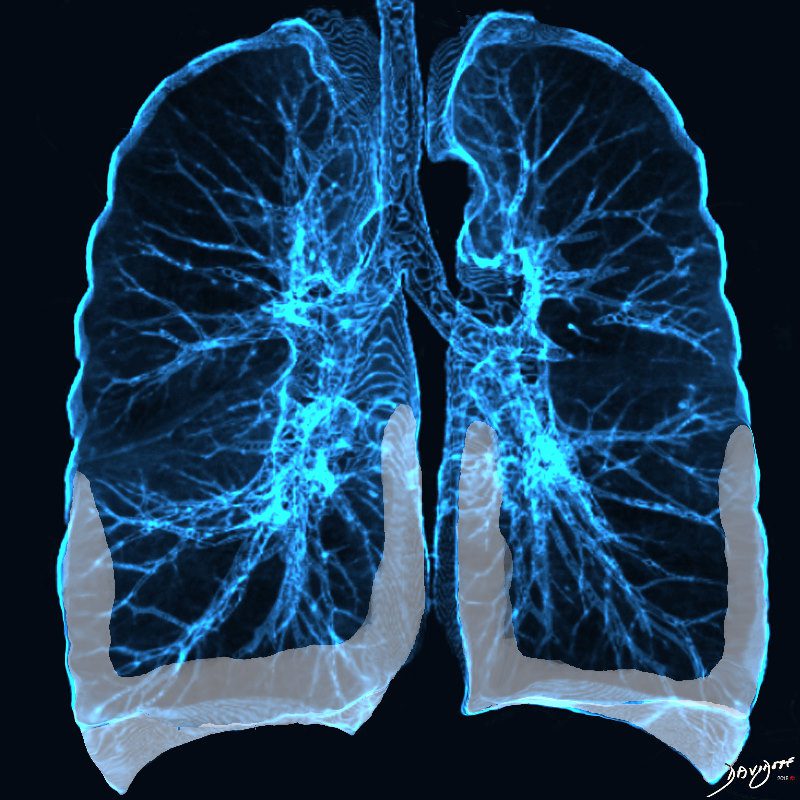
Basilar and peripheral distribution
Ashley Davidoff MD TheCommonvein.net lungs-0769b
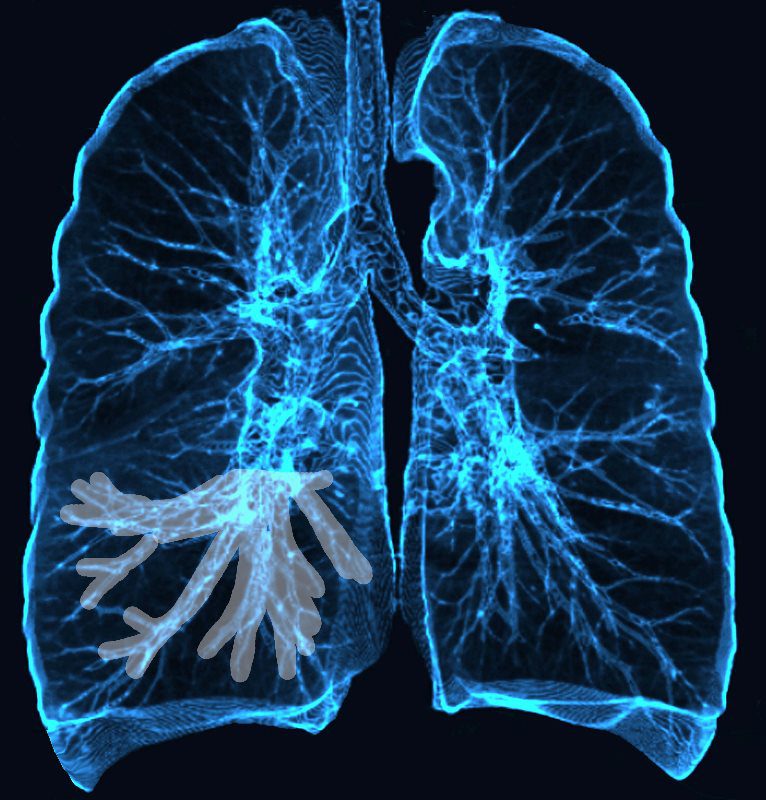
Broncho vascular distribution
Ashley Davidoff MD TheCommonvein.net lungs-0769
Perihilar distribution
Ashley Davidoff MD TheCommonvein.net lungs-0770
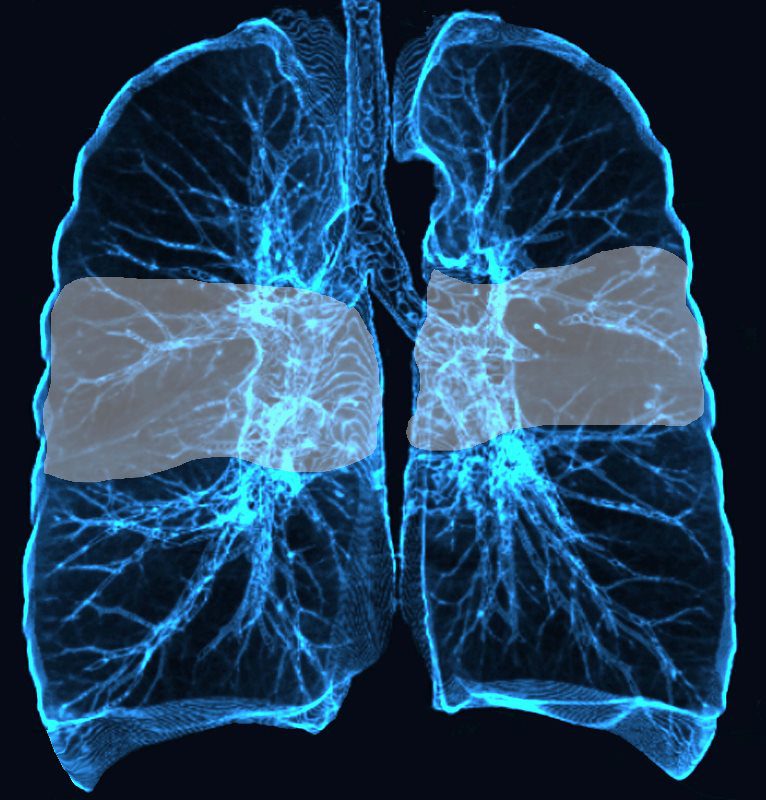
Mid lung field distribution
Ashley Davidoff MD TheCommonvein.net lungs-0773
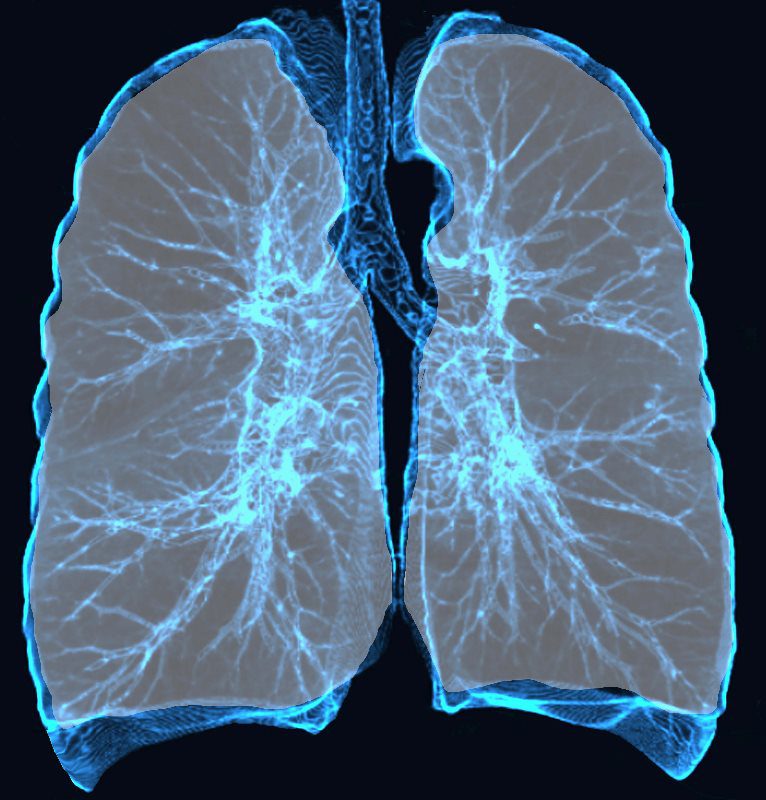
Diffuse Lung Disease
Ashley Davidoff MD TheCommonvein.net lungs-0775

Subpleural Sparing
Ashley Davidoff MD TheCommonvein.net lungs-0775 0775-lo res subpleural sparing
Acute Eosinophilic pneumonia is characterised by ground glass opacities (100%) and sometimes consolidation (55%) most commonly with a random distribution 60%. Septal lines (90%) and thickening of the bronchovascular bundles (66%) and bilateral pleural effusions (75%) were common.
Ashley Davidoff MD TheCommonvein.net lungs-0775-b (Reference De Giacomi F et al)
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
48-year-old previously well presented with dyspnea and initial CXR showed an infiltrate at the right base, and clinically resolved. He presented a year later with right chest pain and low grade ever and the CXR showed patchy opacities in the LUL and in the RLL
A subsequent CT showed LUL nodular opacities and subpleural rim of consolidation in the LUL and more prominently at both lung bases, associated with significant mediastinal adenopathy. Lymphovacscular nodularity was noted in the bronchovascular bundles as well as in the interlobular septa, consistent with sarcoidosis
CXR and CT 4 years later showed almost complete resolution of the parenchymal findings and the CT findings except for minimal reticulation and scarring in the subpleural regions
Ashley Davidoff MD