
Parts and Bonds
Ashley Davidoff MD TheCommonVein.net lungs-0060

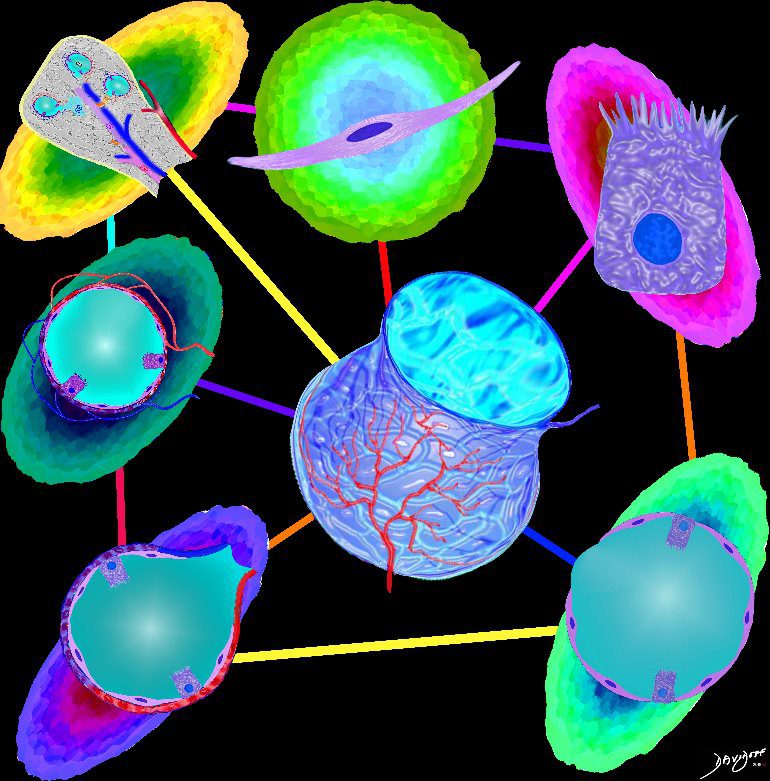
The five major layers that keep the air moving include the outer bony cage, the muscular layer represented in maroon, the pleural complex (orange yellow orange) the lung (blue) and surfactant within the alveolus. (pink) by Ashley Davidoff MD TheCommonVein.net lungs-0014 aka 42530b05b09b01a08
The diagram shows an alveolus, lined by a single layer of squamous cells,
Ashley Davidoff MD TheCommonVein.net lungs-0705-lo res
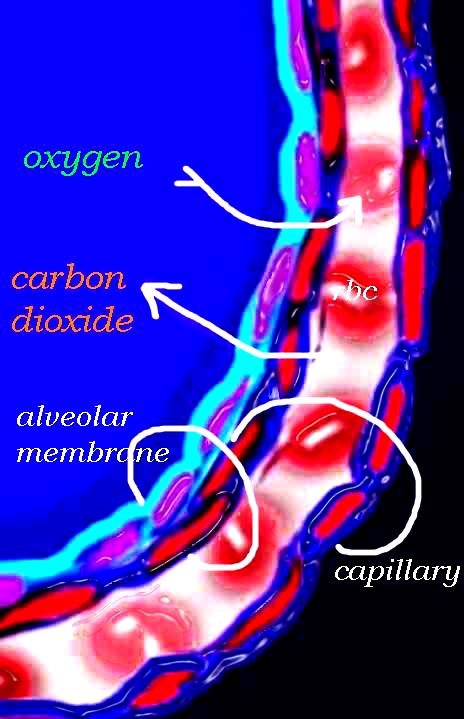
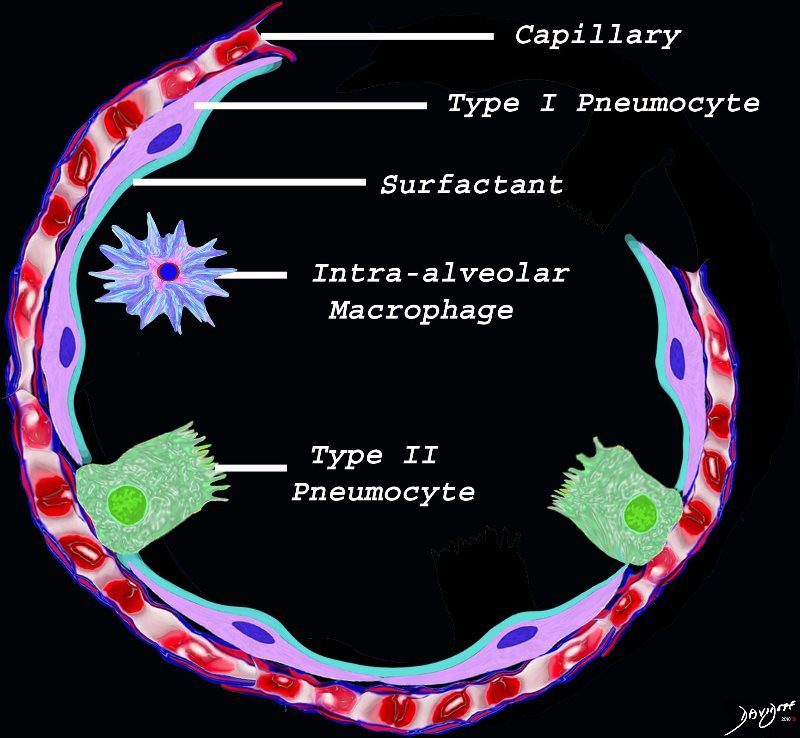
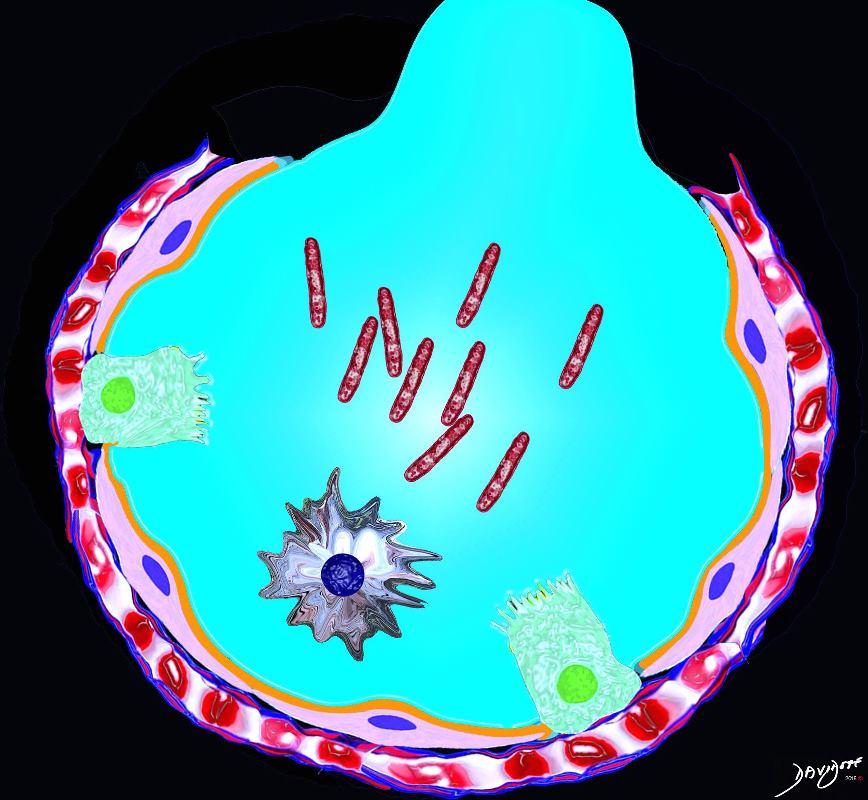
The diagram shows an alveolus, lined by a single layer of squamous cells, surrounded by a capillary with red cells which is also lined by a single layer of squamous endothelial cells . The images show exchanges of oxygen and carbon dioxide through the alveolar membrane .
Ashley Davidoff MD TheCommonVein.net lungs-0028b-low res
Ashley Davidoff MD TheCommonvein.net lungs-0056
key words
key words RS lung alveolus respiratory bronchiole artery vein pulmonary capillary normal anatomy histology drawing
Ashley Davidoff MD TheCommonVein.net 32164
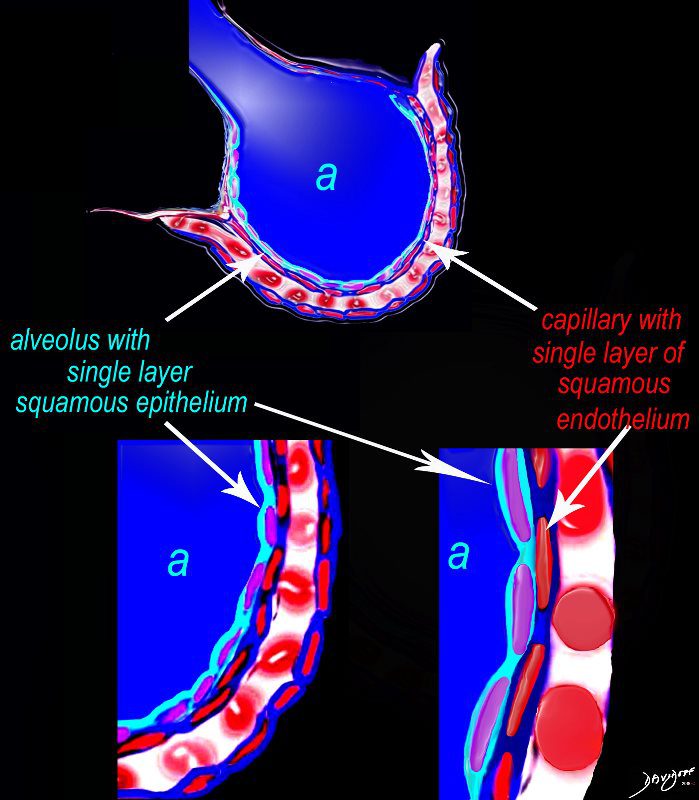
The diagram shows an alveolus (a) above, lined by a single layer of squamous cells, surrounded by a capillary with red cells which is also lined by a single layer of squamous endothelial cells . The images below show progressive magnification of the alveolar wall demonstrating the two thin layer of the alveolar membrane .
Ashley Davidoff MD TheCommonVein.net lungs-0028-low res

Ashley Davidoff MD TheCommonVein.net lungs-0026
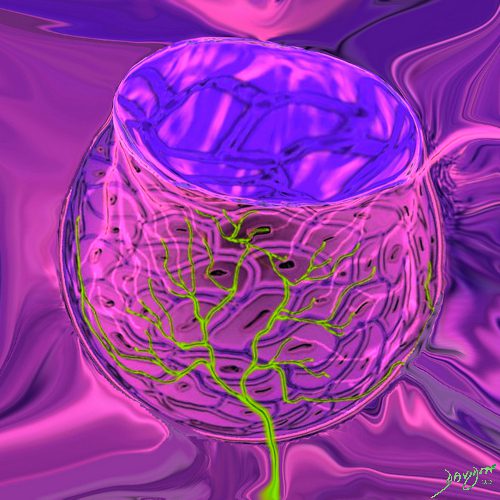
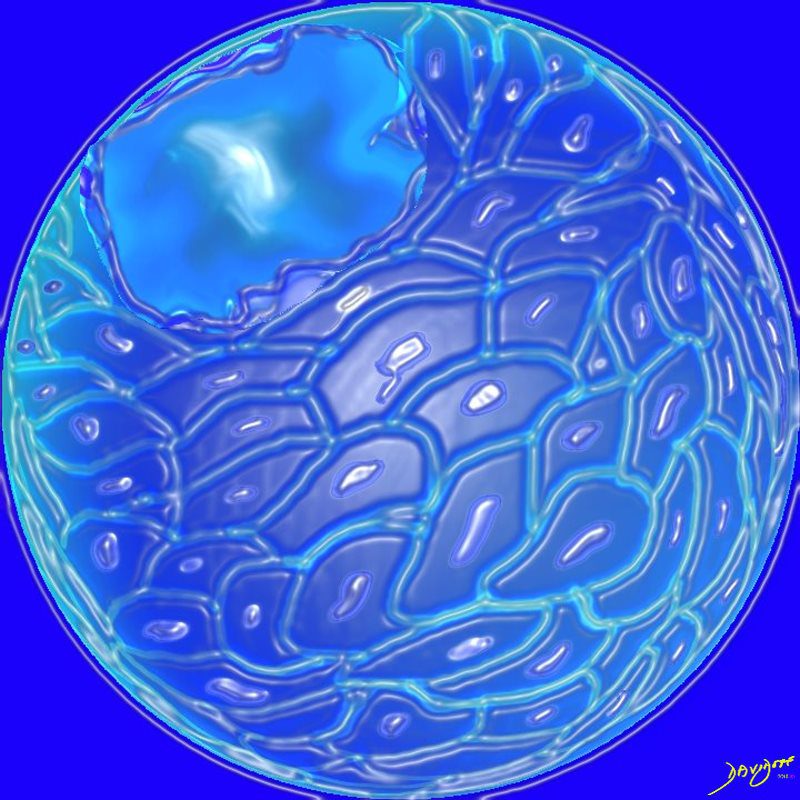
This drawing demonstrates the open mouth view of the alveolus, which is surrounded by its tree like capillary network. The lining single layer of squamous cells (pneumocytes) can be seen peaking through the vessels.
Ashley Davidoff MD. TheCommonVein.net lungs-0022

Ashley Davidoff MD TheCommonvein.net
Ashley Davidoff MD. TheCommonVein.net 32166
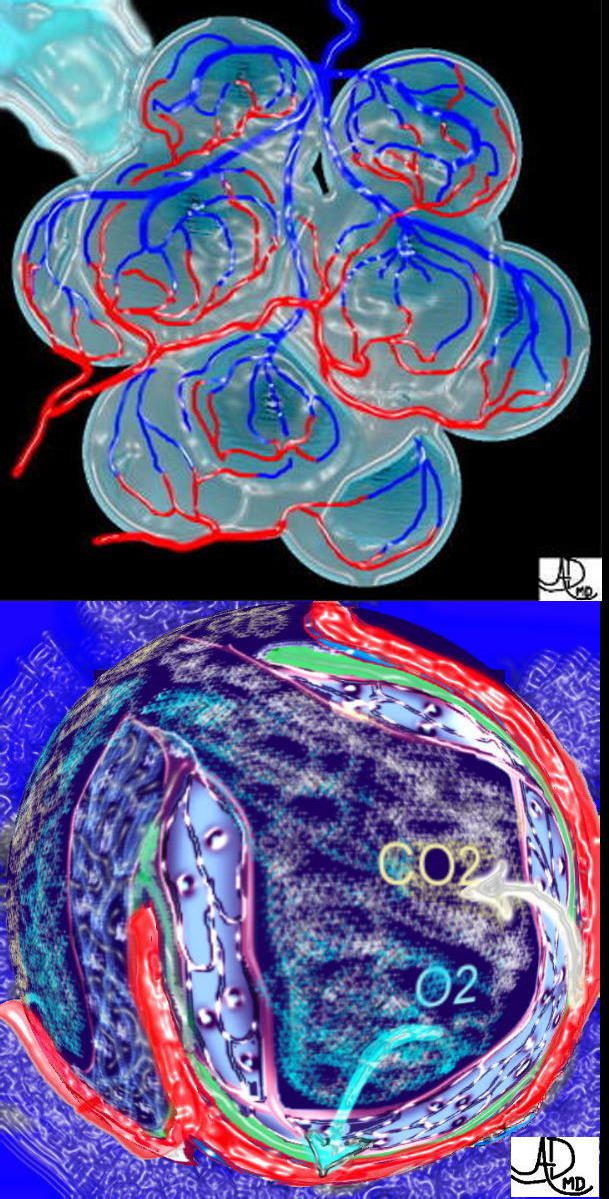
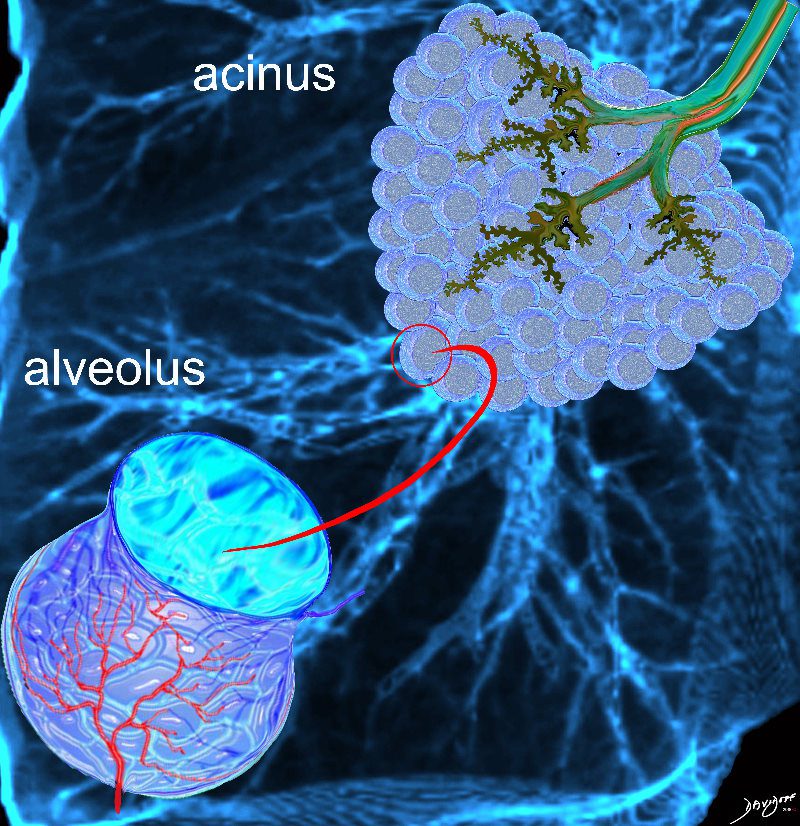
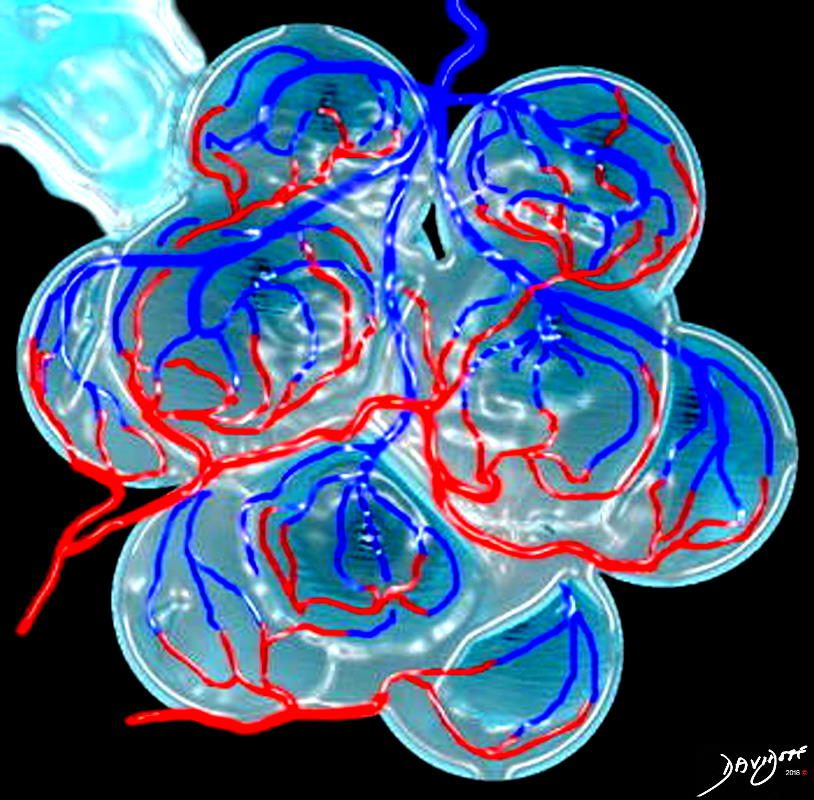
This is a drawing of a cluster of alveoli surrounded by the capillary network, fed by an arteriole in blue, and drained by a venule in red. The second image shows the exchange of life giving oxygen for the by product of metabolic activity – carbon dioxide
Ashley Davidoff MD
TheCommonVein.net
32165c
Courtesy Ashley Davidoff MD The CommonVein.net lungs-0735
Ashley Davidoff TheCommonVein.net lungs-0689

Ashley Davidoff TheCommonVein.net lungs-00679
Ashley Davidoff MD TheCommonVein.net lungs-0008
Courtesy Ashley Davidoff MD The CommonVein.net lungs-0735
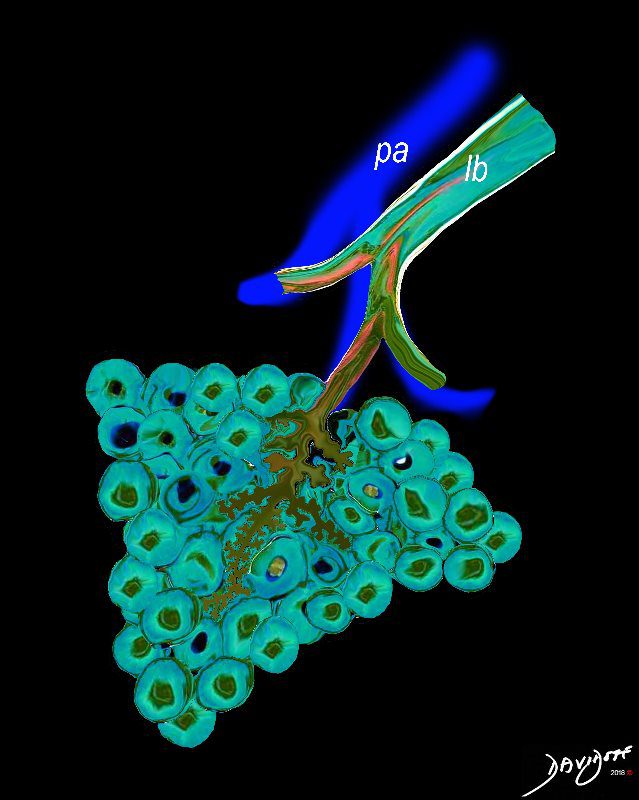
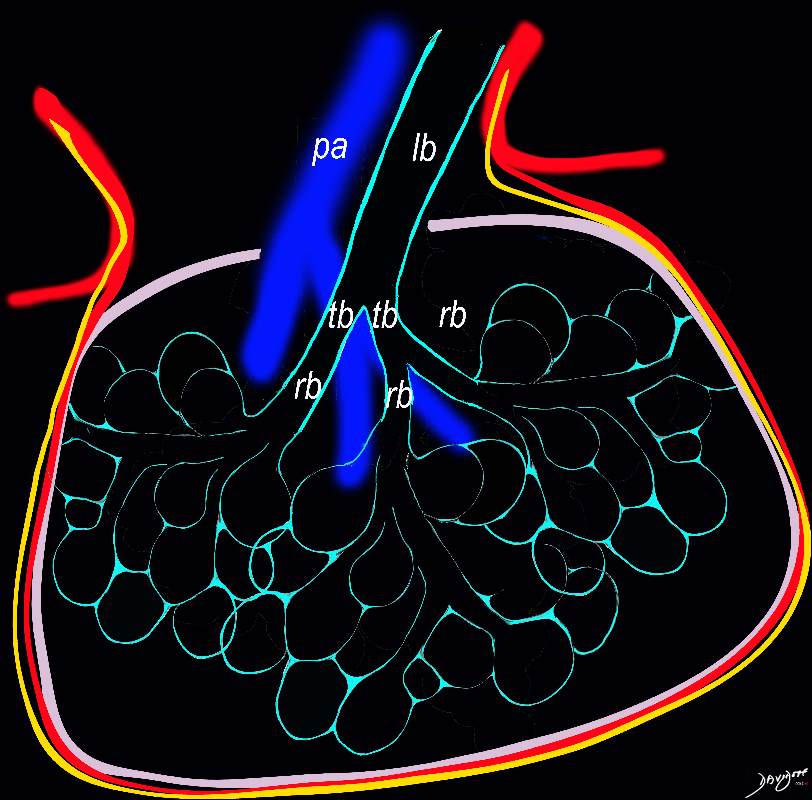
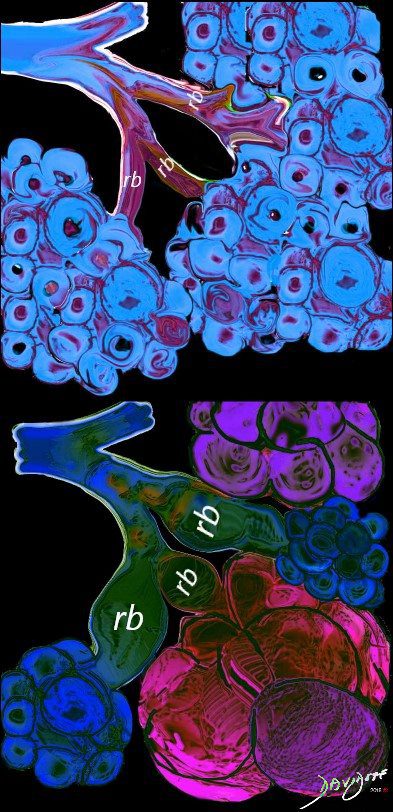
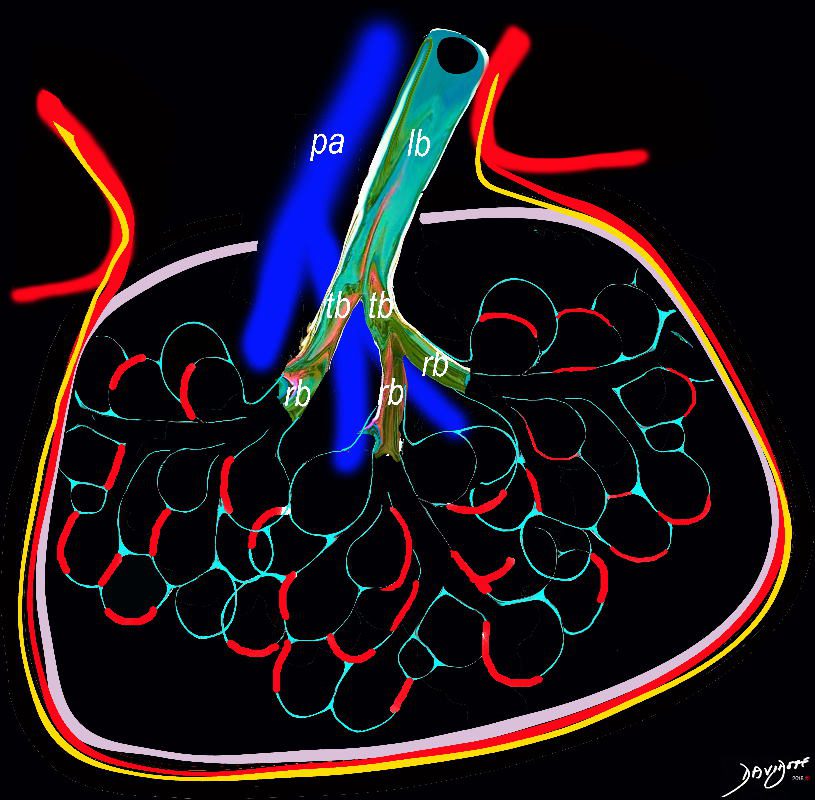
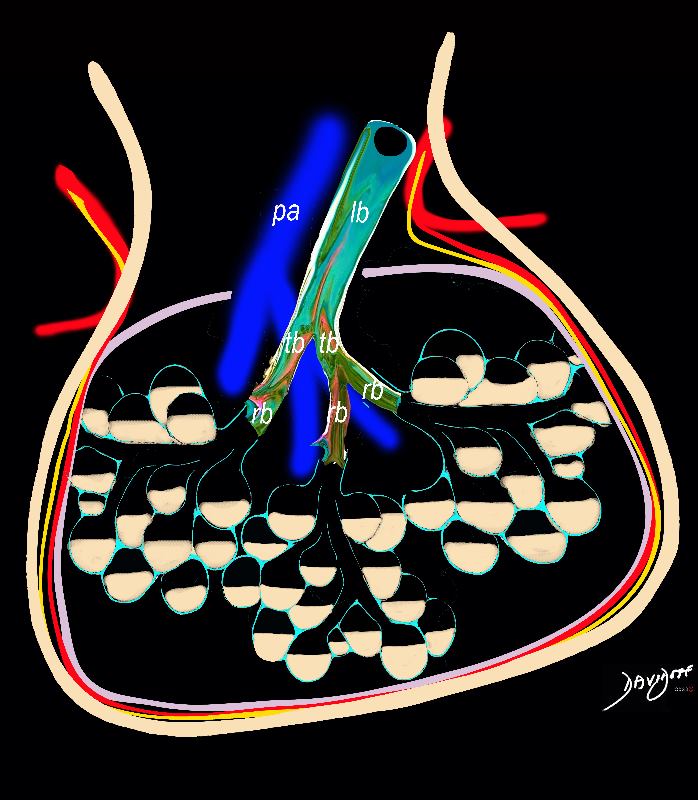
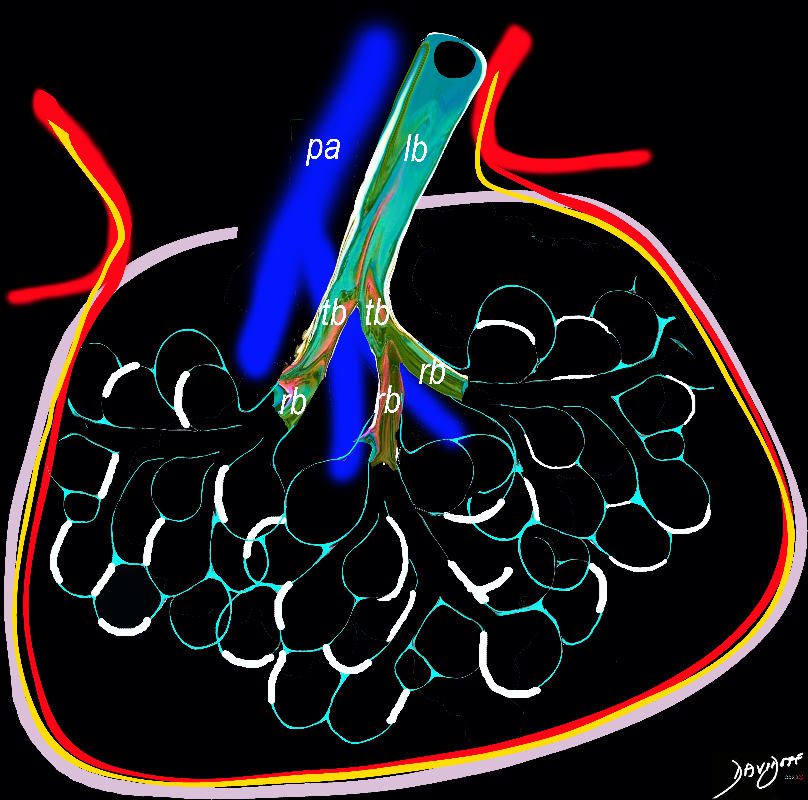
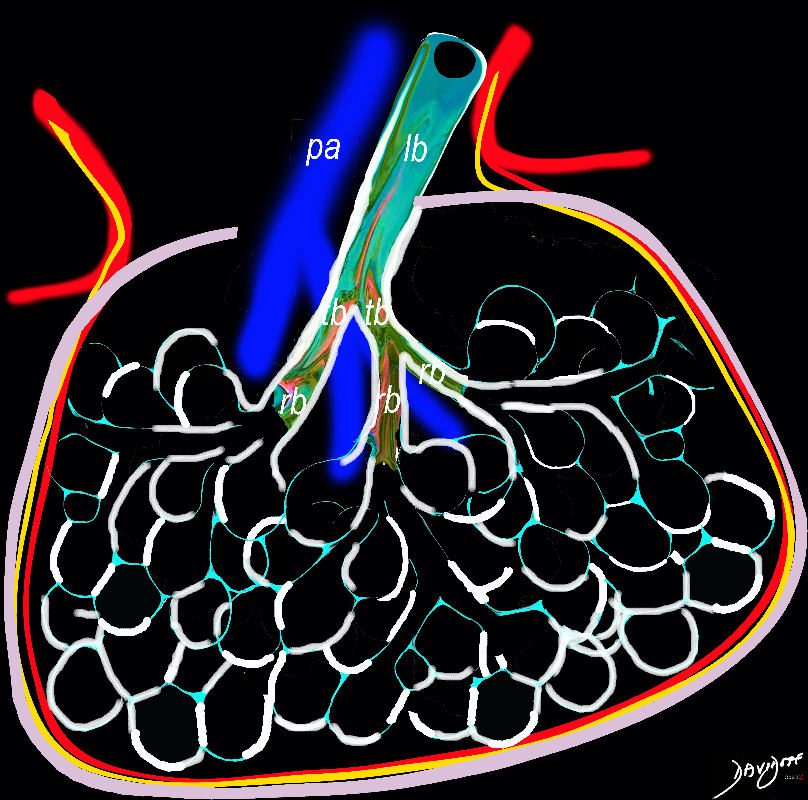
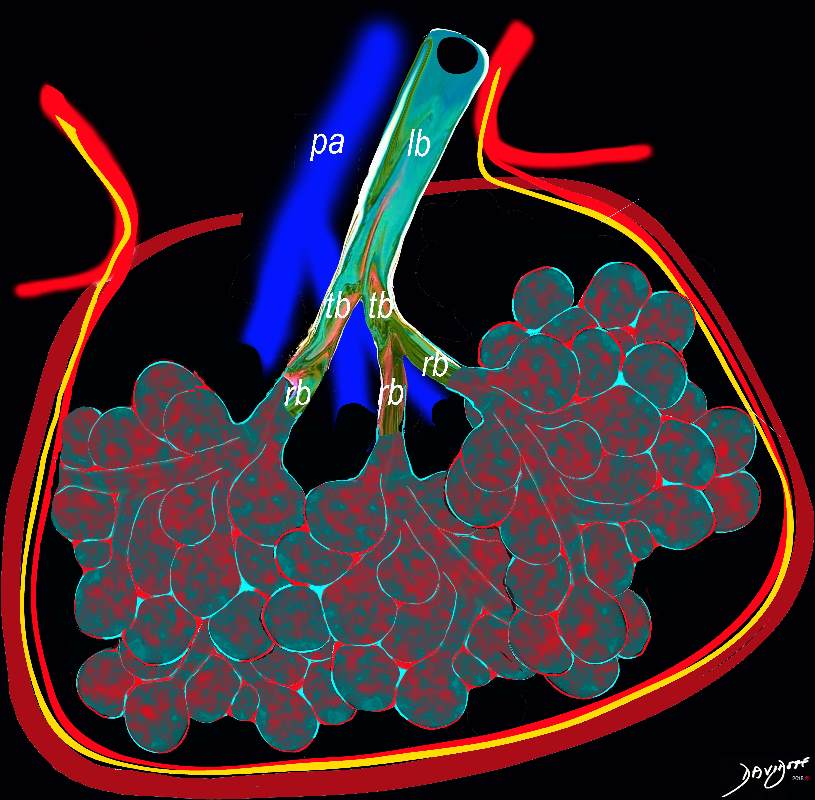
The pulmonary arteriole (pa) accompanies the lobular bronchiole (lb). The arteriole transports deoxygenated blood and the bronchiole carries oxygen from the trachea to the alveoli.
They part ways at the alveoli
Ashley Davidoff MD TheCommonVein.net lungs-0034
Disease

Ashley Davidoff MD TheCommonvein.net lungs-0021

A hyaline membrane evolves covering the damaged surface of the alveolus. This impedes gas exchange
Ashley Davidoff
TheCommonVein.net lungs-0694
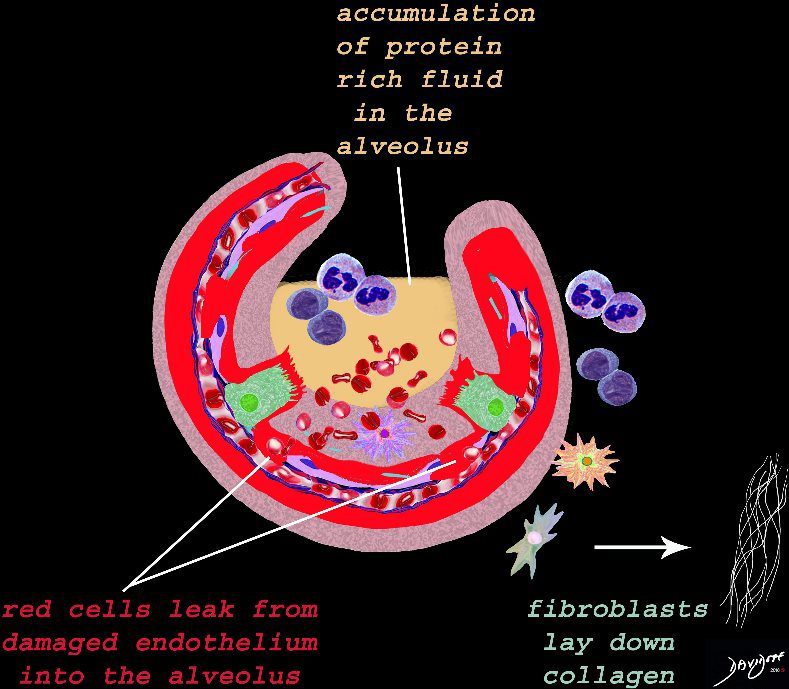
The damage to the endothelium of the capillary results in bleeding into the alveoli. The severe tissue damage and fluid exudation results in protein rich intra-alveolar fluid . The fibroblasts start to lay down collagen as part of the early repair process
Ashley Davidoff
TheCommonVein.net lungs-0693
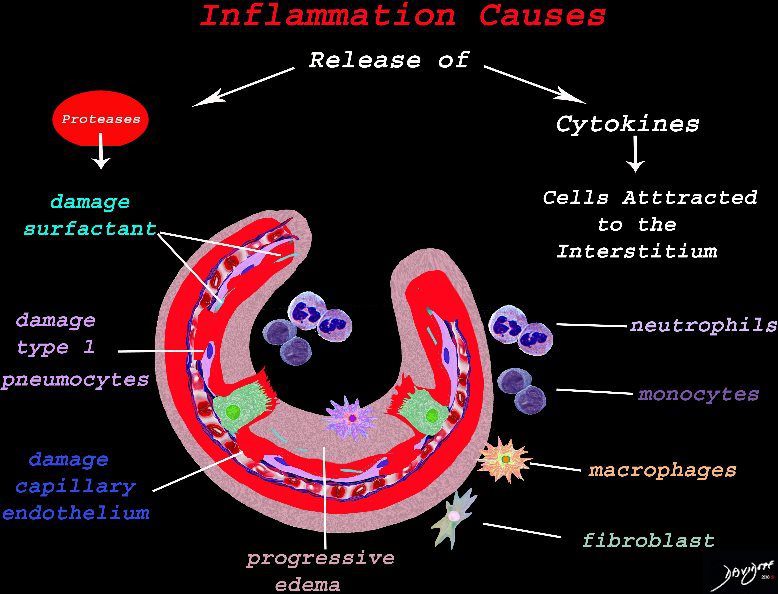
The cells of the immune system release cytokines, chemotactic agents and proteases. Immune cells , macrophages and fibroblasts are attracted to the interstitium. Some of proinflammatory agents are toxic to the cell lining causing damage to the surfactant, type 1 pneumocytes and the capillary endothelium. There is progressive edema.
Ashley Davidoff
TheCommonVein.net lungs-0692
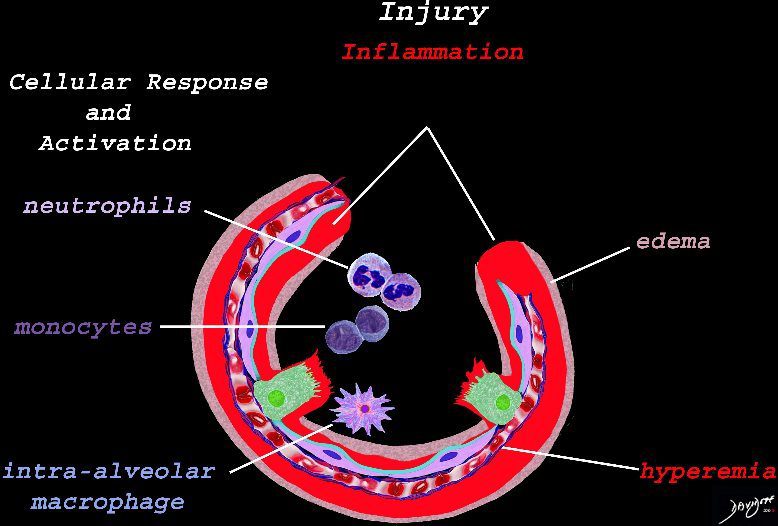
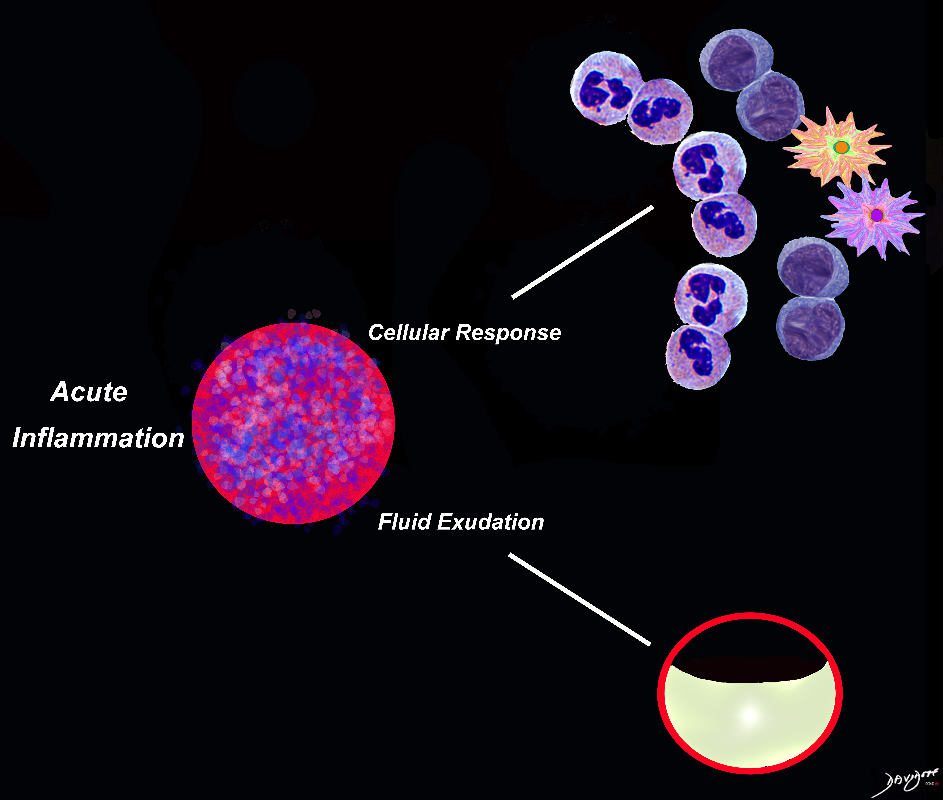
The initial injury results in an acute severe inflammatory response consisting hyperemia , edema with migration initially of neutrophils in the first 6-24 hours followed by monocytes (24-48hours). The intra -alveolar macrophages are activated.
Ashley Davidoff
TheCommonVein.net lungs-0691
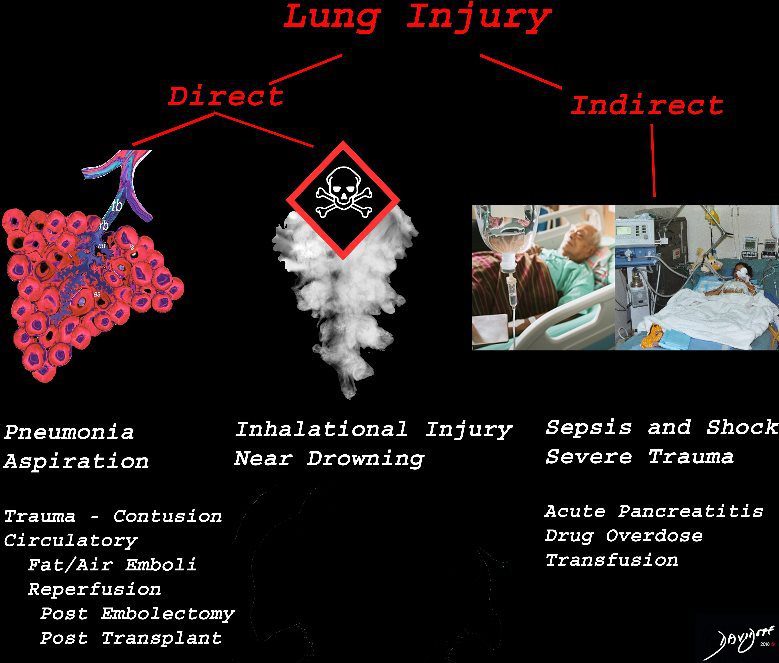
The lung is injured either by direst causes most commonly pneumonia, aspiration or from inhalation of toxic substances. Severe systemic illnesses, most commonly sepsis with shock, and severe trauma are considered indirect causes.
Ashley Davidoff
TheCommonVein.net lungs-0690
Ashley Davidoff TheCommonVein.net lungs-00683
Ashley Davidoff MD TheCommonVein.net lungs-0038
Ashley Davidoff MD TheCommonVein.net lungs-0752
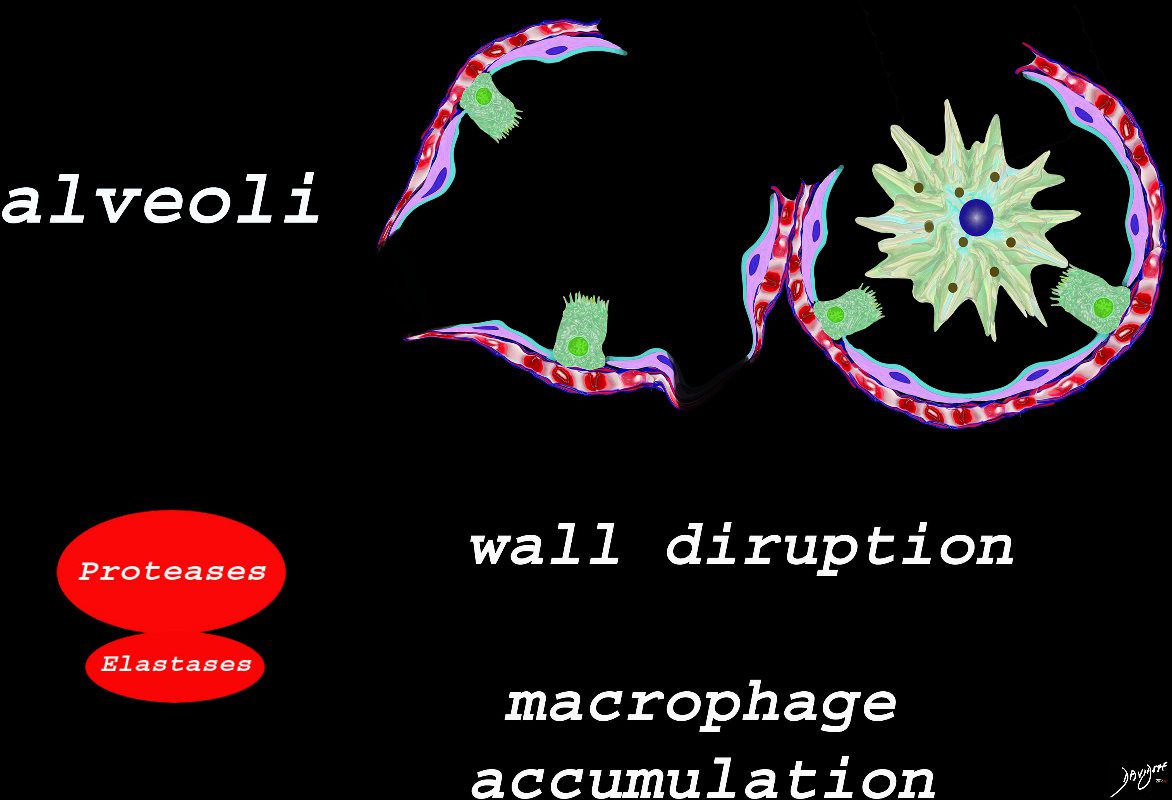
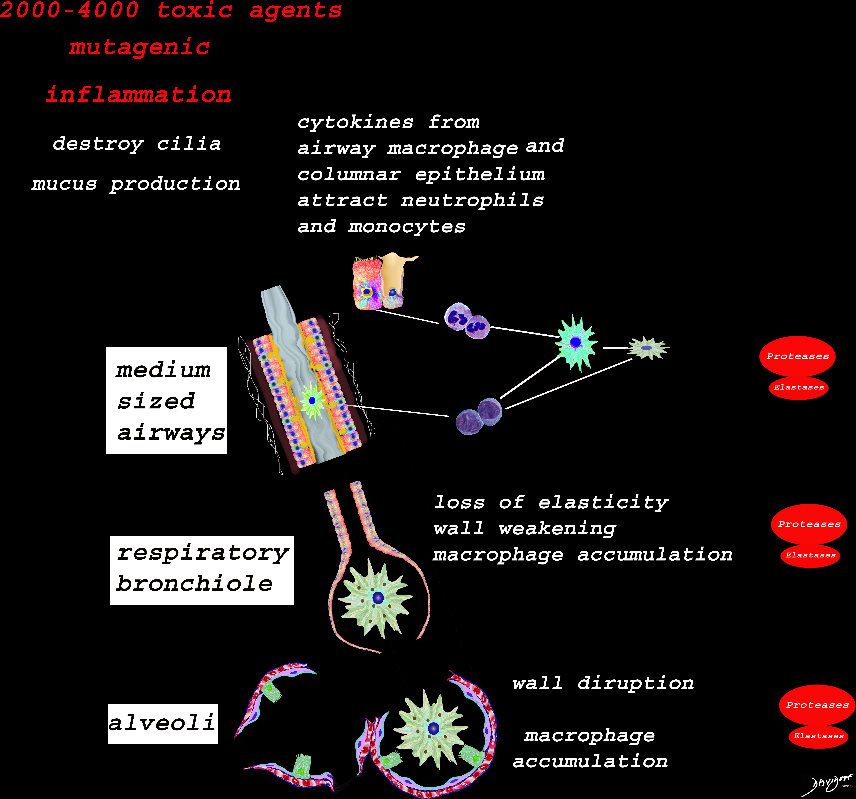
The effect of the proteases and and elastases cause destruction of the alveoli and loss of elasticity, and therefore overall function. The destruction leads to bullous disease
The accumulation of smokers macrophage, and in the case of Langerhans cell histiocytosis leads to space occupation of the alveoli also reducing function
Ashley Davidoff
TheCommonVein.net
lungs-00687
Understanding Radiology and the Alveoli

When the alveoli are fully filled with fluid, tumor, or pus for example, the overall net density will be white, and when adjacent to air filled airways, air bronchograms are visible (left side of image)
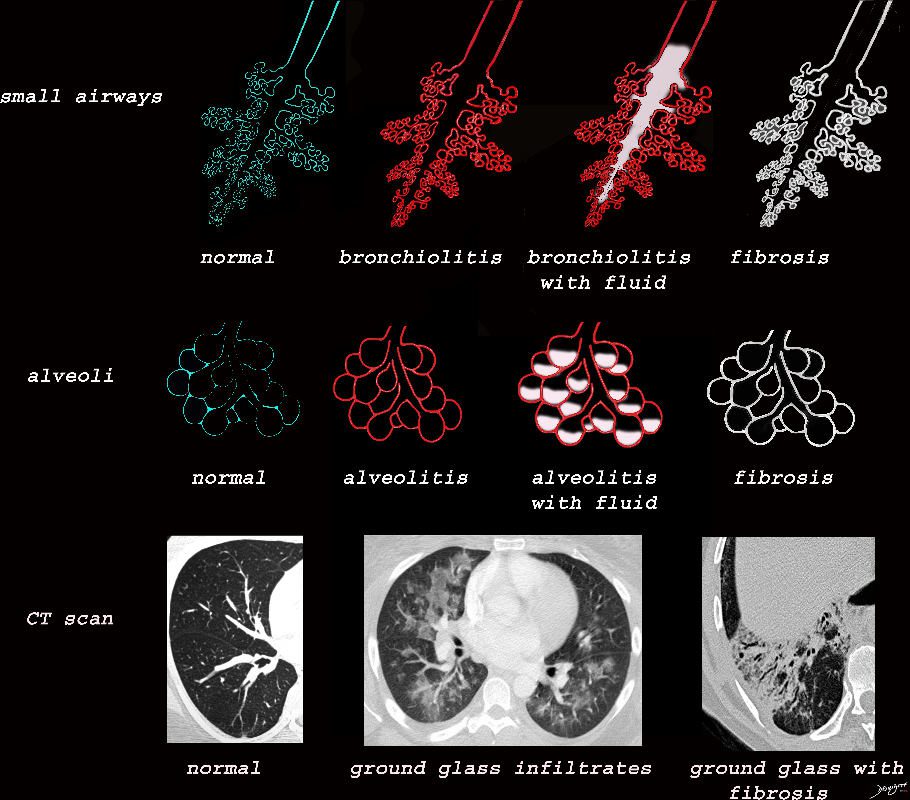
When the alveoli are only partially filled, the density of the fluid added to the density of the air results in an overall gray density, and when positioned next to air filled bronchi, there is insufficient contrast to create an air bronchogram and sufficient to enable visualization of the blood vessels. This is called ground glass opacification
Ashley Davidoff
TheCommonVein.net lungs-00681
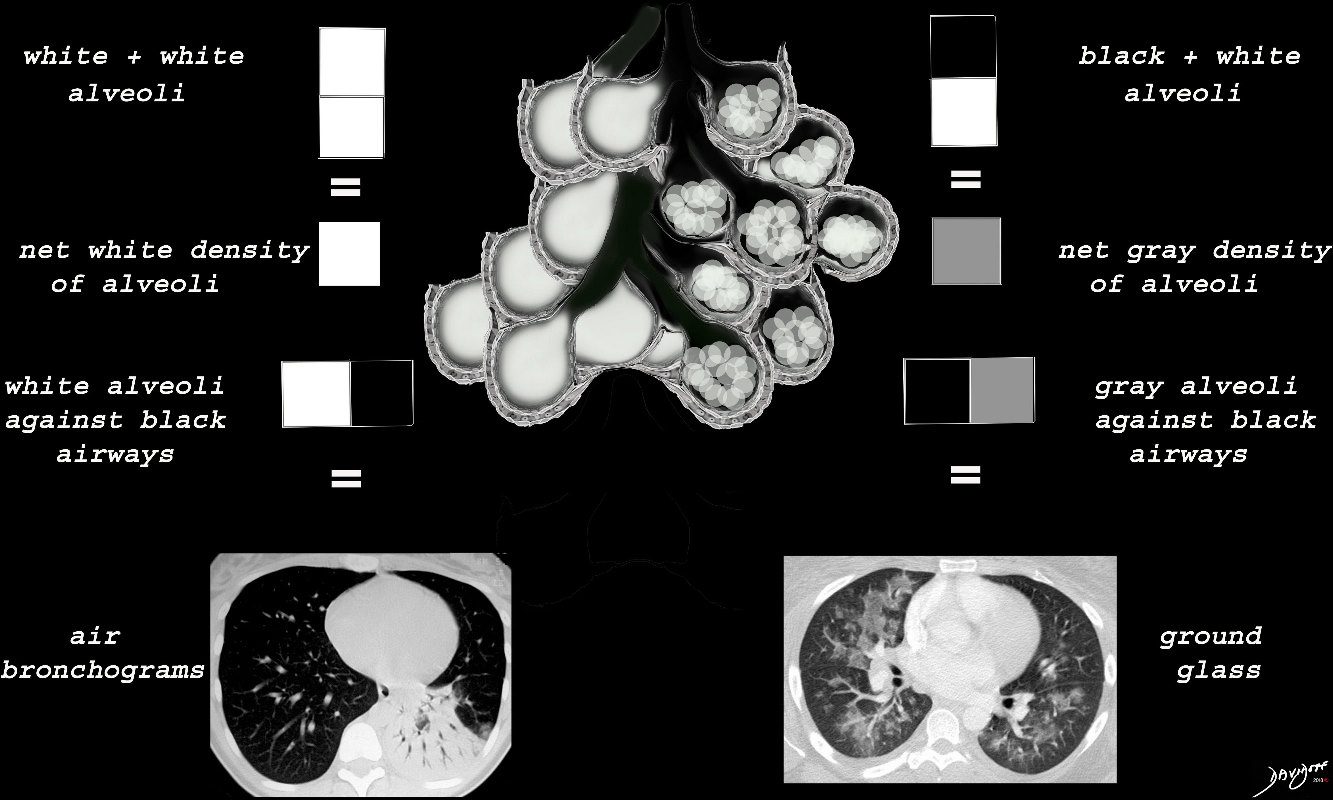
When there are extensive ceelular accumulations in the alveoli, such as adenocarcinoma with lepidic growth, Langerhans cells or other macrophages, the overall net density of the region of involvement will be gray, and when adjacent to the black air filled airways, a ground glass appearance will be apparent
Ashley Davidoff
TheCommonVein.net
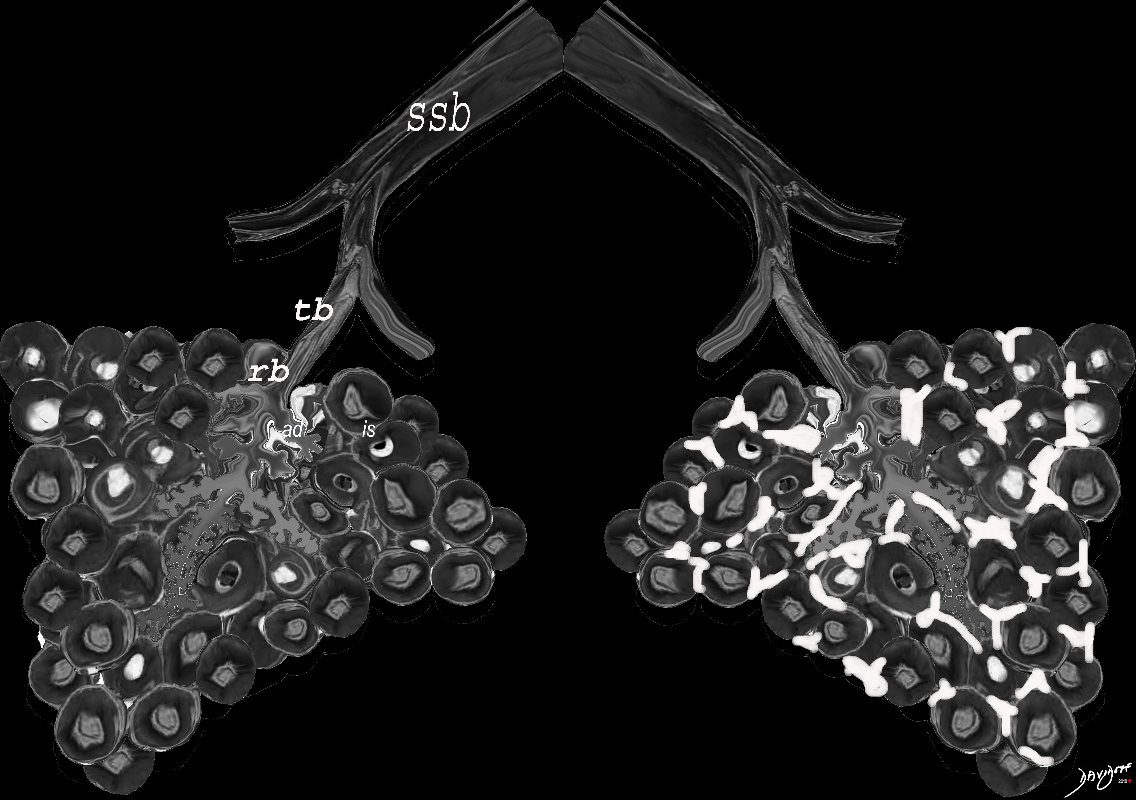
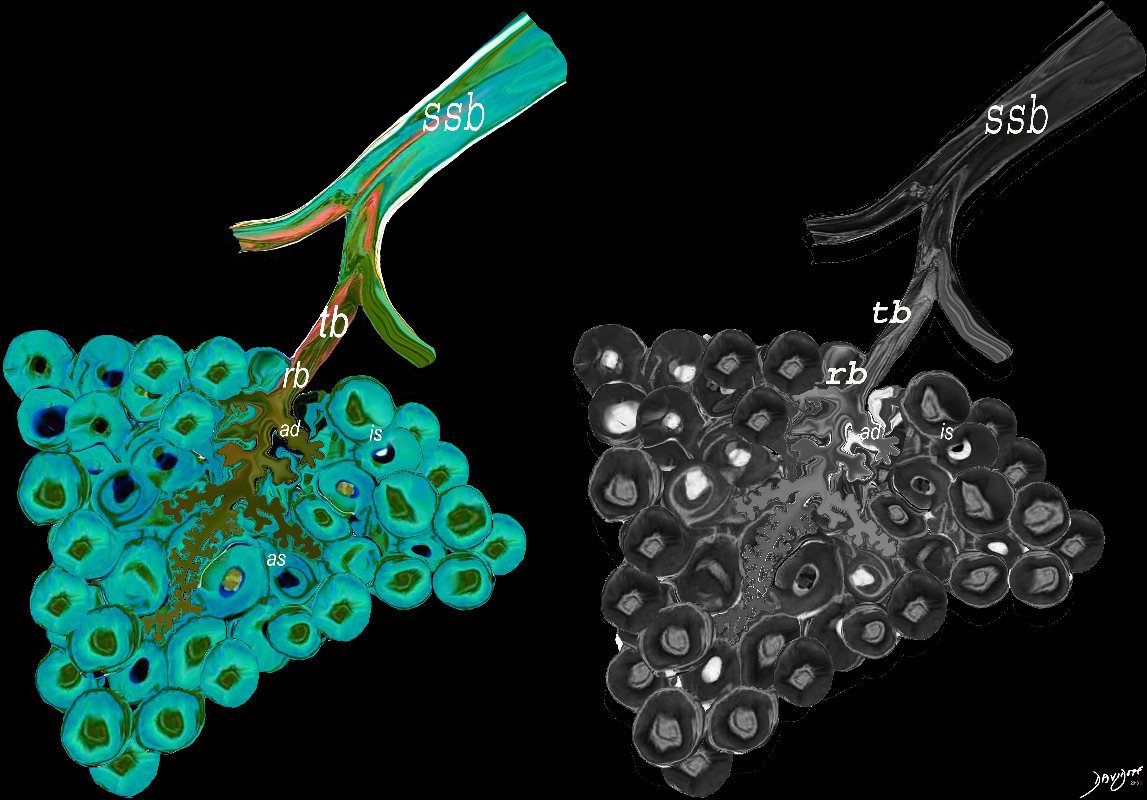
ssb = subsegmental bronchiole
tb = terminal bronchiole
rb = respiratory bronchiole
as = alveolar duct
as = alvelar sac
is = anteralveolar septum
lungs-00688
Ashley Davidoff TheCommonVein.net lungs-00682
Black White and Gray Densities
The filling of alveoli with fluids or cells results in a density that is “white” on X-ray and CT scan and is in distinct contrast to the black of the air filled airways. This contrast results in an air bronchogram. The smaller airways in a normal patient are not usually visualized because the “black” of the of the airways and the black of the air filled alveoli does not create a contrast.
Ashley Davidoff MD TheCommonvein.net
lungs-0708d
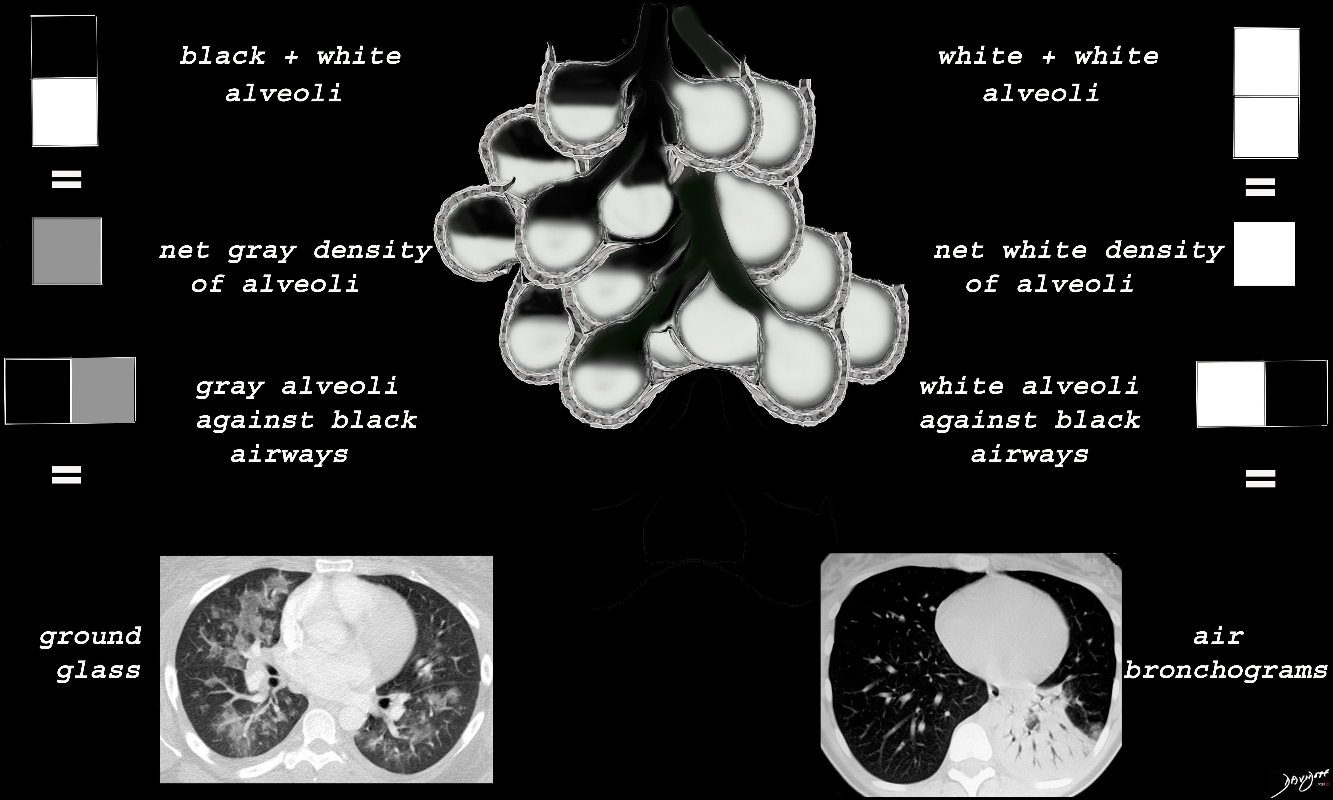
Black White and Gray Densities
An air filled alveolus appears as black, a fluid filled alveolus appears as white and a a half filled alveolus appears as gray
Ashley Davidoff MD TheCommonvein.net lungs-00688b
Ashley Davidoff TheCommonvein.net lungs-00680
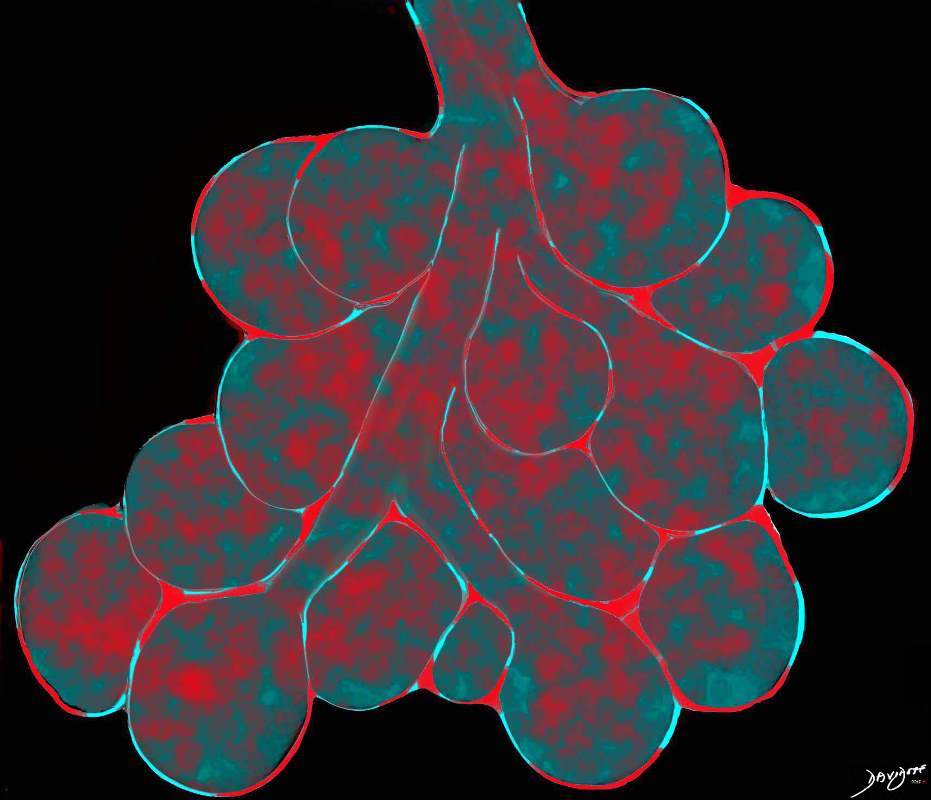
Interstitial changes (red parts of alveoli ) representing either infiltration into the interstitium or inflammatory changes in the interalveolar interstitium
Ashley Davidoff TheCommonVein.net lungs-0736a01
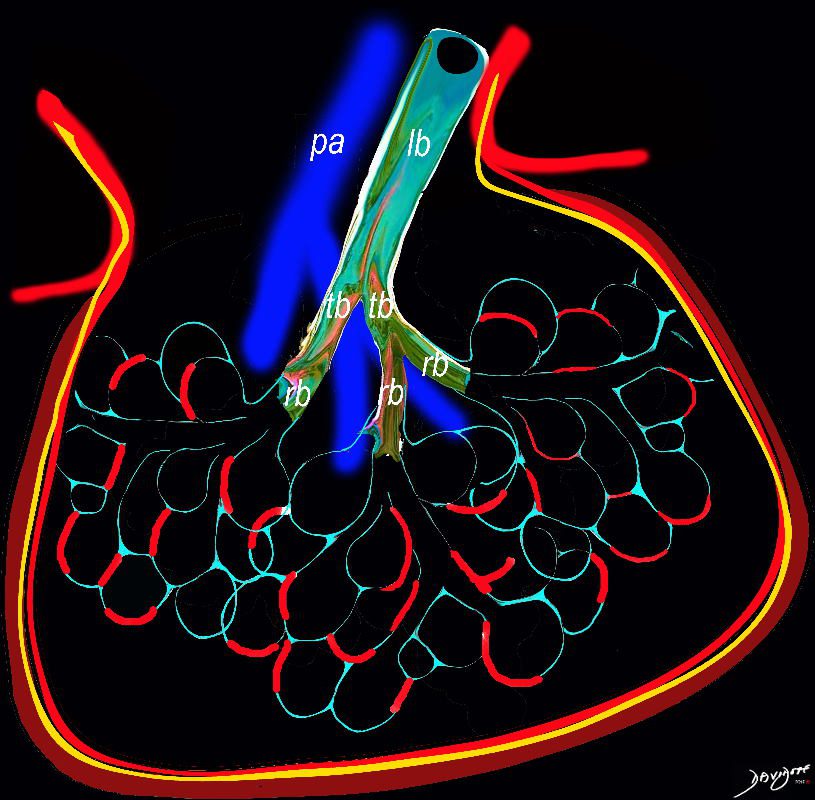
Diagram shows inflammation (red ) in the walls of the alveoli with thickening of the interlobular septa (maroon) . The increased density in the interalveolar septa and interlobular septa results in a ground glass opacity with and crazy paving appearance on CT scan
Ashley Davidoff TheCommonVein.net
lungs-0736a
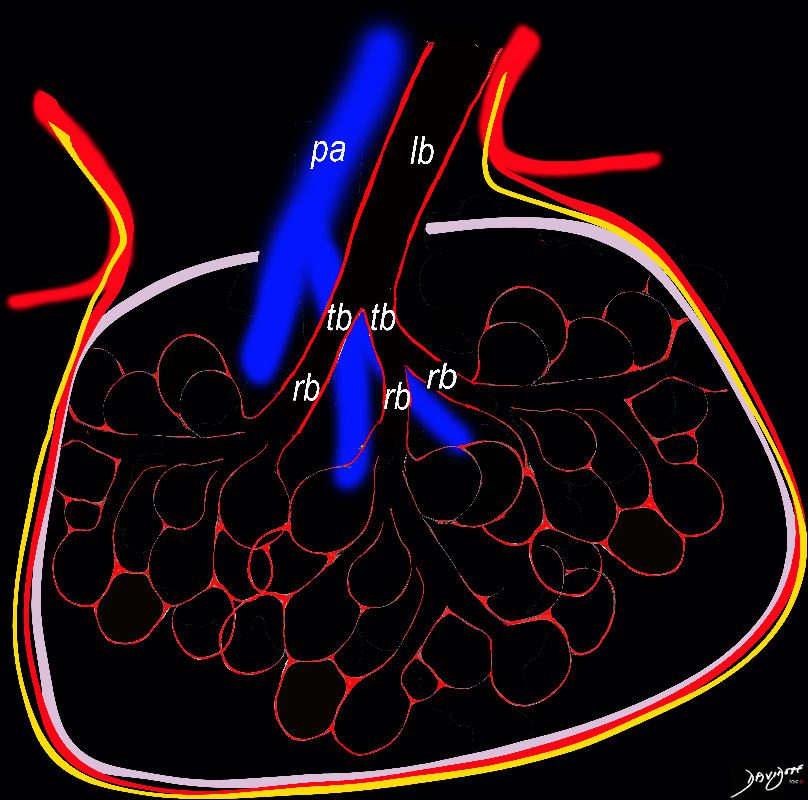
Diagram shows inflammation (red ) in the walls of the alveoli. The increased density in the interalveolar septa results in a ground glass opacity on T scan
Ashley Davidoff TheCommonVein.net
lungs-0736
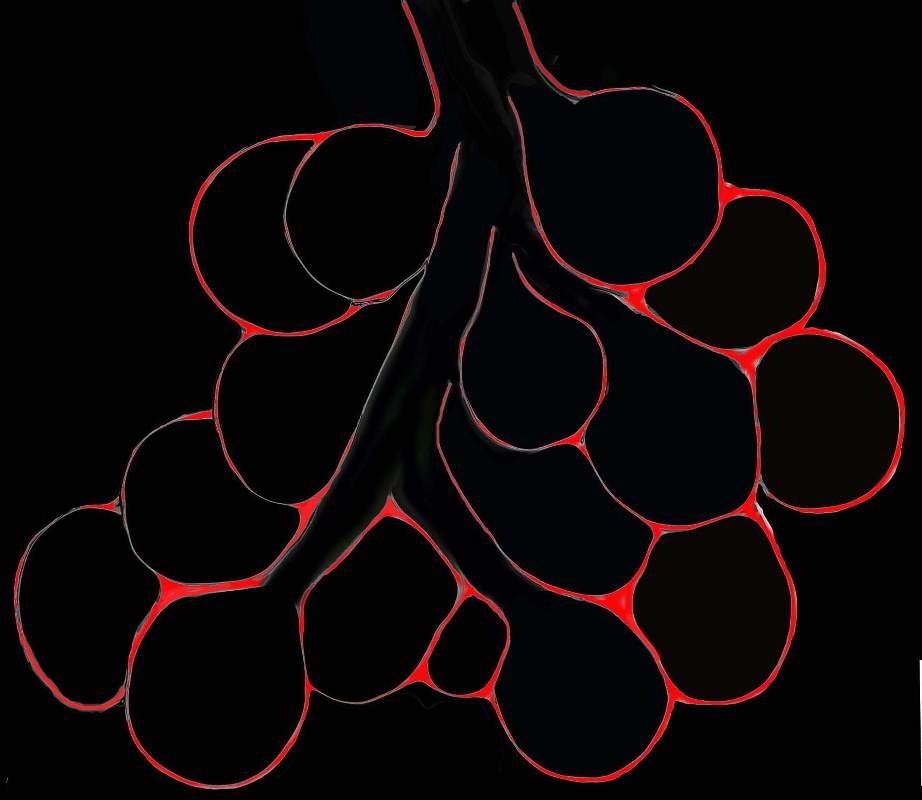
Diagram shows inflammation (red ) in the walls of the alveoli. The increased density in the interalveolar septa results in a ground glass opacity on T scan
Ashley Davidoff TheCommonVein.net
lungs-0736b
Ashley Davidoff MD TheCommonVein.net lungs-0698d
Ashley Davidoff MD TheCommonvein.net lungs-0732b01
Ashley Davidoff MD TheCommonVein.net lungs-0702d- lo res
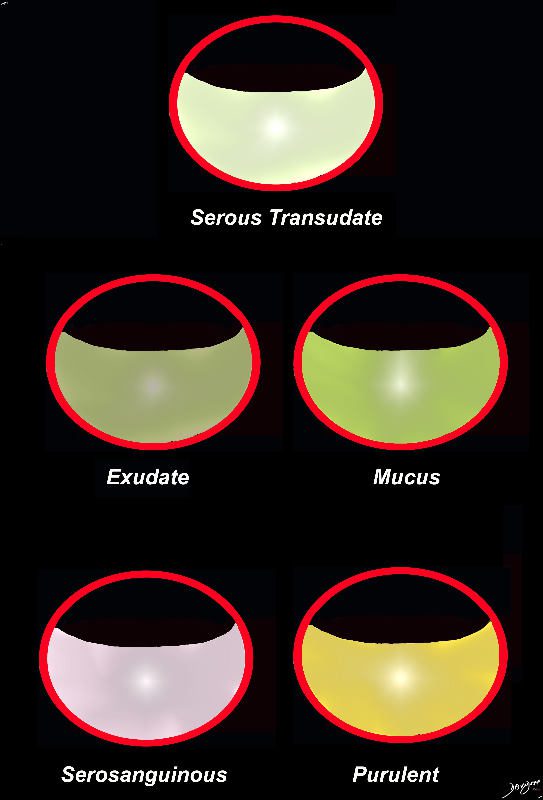
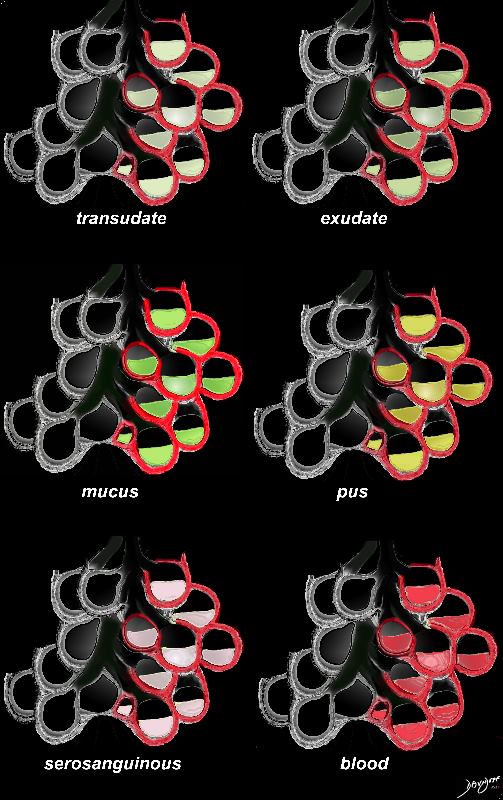
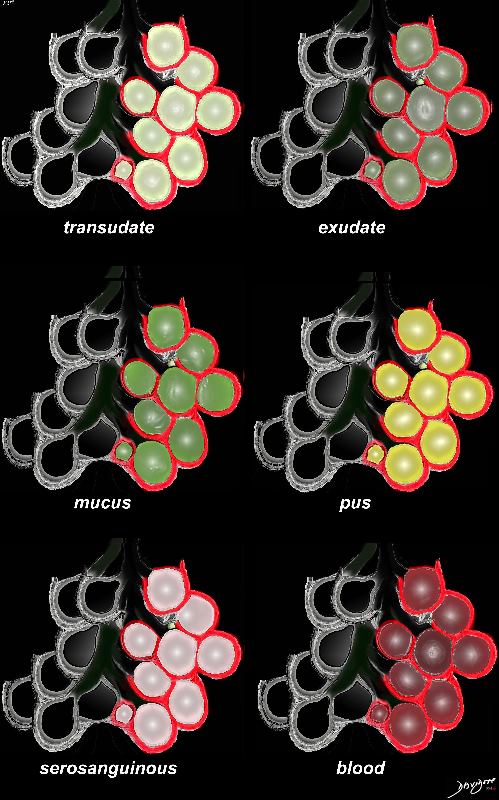
The acute inflammatory process results in fluid exudation into the alveoli which can take the form of a serous transudate, and exudate or in the form of mucus, and when severe (eg ARDS) can result in tissue and vessel destruction and could be be blood tinged. Infected fluid could be mucoid or purulent. The extent of filling the alveoli results either in a ground glass appearance when partially filled or a consolidation when filled.
Ashley Davidoff MD TheCommonVein.net
lungs-0701d- lo res
Ashley Davidoff MD TheCommonVein.net lungs-0704
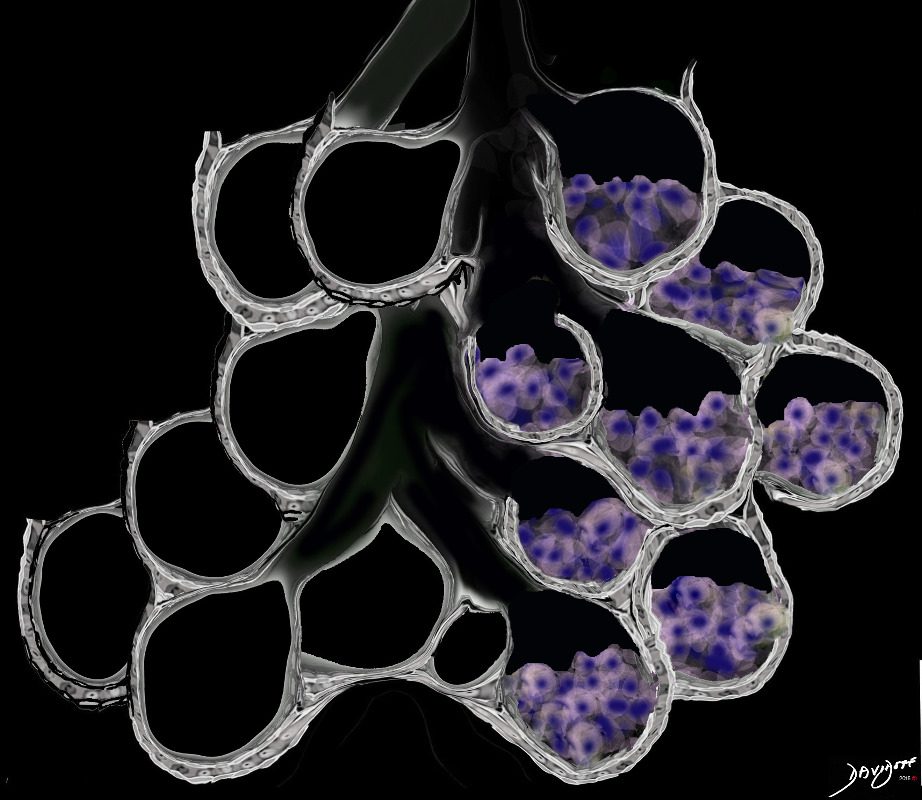
Ground Glass Opacity (GGO) Caused by Cellular Accumulation with Partial Filling of the Alveolus Ground glass opacification may be caused by partial filling of the alveolus with cellular material with partial replacement of air with solid material with the net density being gray rather than white if the alveolus were fully filled. The black of the airway nor the white of the vessels may blend with the gray density and hence they are not visualized in ground glass opacities.
Ashley Davidoff MD TheCommonVein.net lungs-0707a
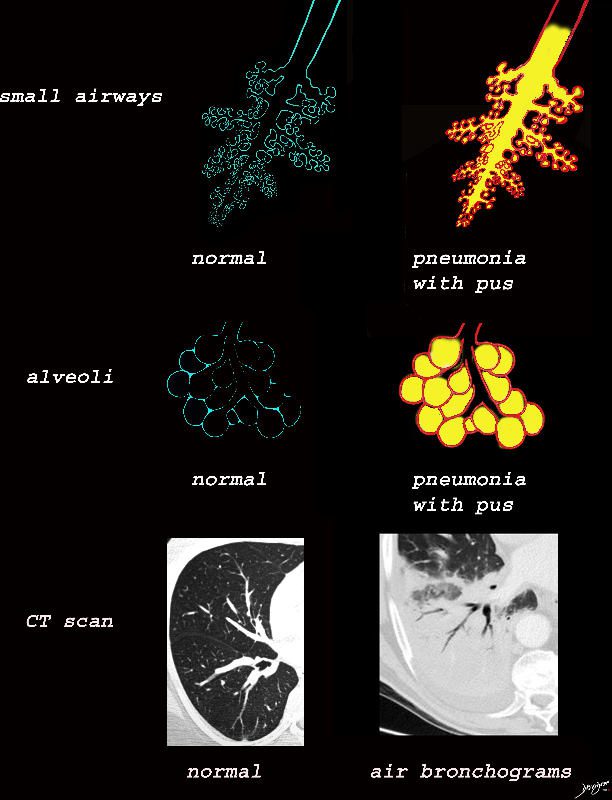
The collage provides a perspective of purulent accumulation in the small airways and the alveoli that results in consolidation. A process that increases the density of the lungs to a net “white” regional density will result in a consolidation and in this case when the fluid is infected it is labelled “pneumonia” The net result on CT is air bronchograms within the non aerated dense lung tissue.
Ashley Davidoff MD TheCommonVein.net lungs-0734
Alveolar Proteinosis
Ashley Davidoff TheCommonVein.net lungs-0738b
Ashley Davidoff MD TheCommonVein.net lungs-0733
Fibrotic Diseases
Ashley Davidoff TheCommonVein.net
lungs-0738b
Ashley Davidoff TheCommonVein.net lungs-0738b01
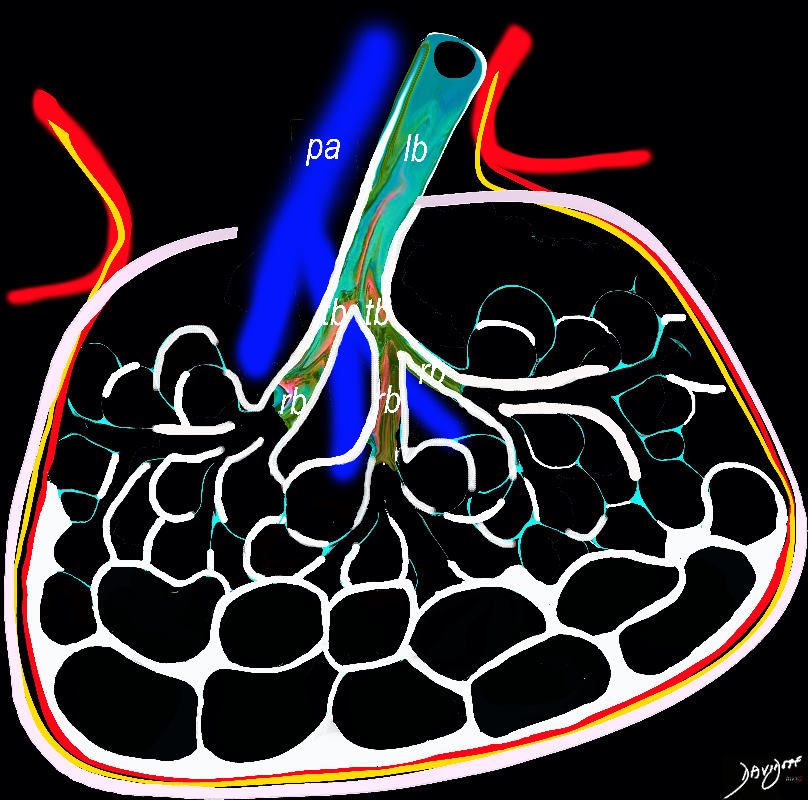
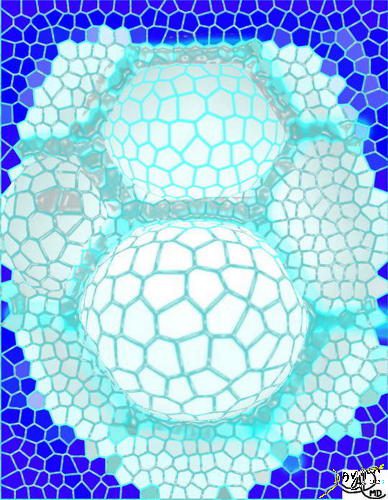
In patients with interstitial lung disease, the inflammatory process and interstitial fibrotic disease progresses and the walls between the alveoli are destroyed causing large subpleural, variably sized, subpleural, thick walled, stacked, cystic spaces . The appearance is reminiscent of a honeycomb and indicates end stage fibrosis
Ashley Davidoff MD thecommonvein.net lungs-0738bh
NSIP
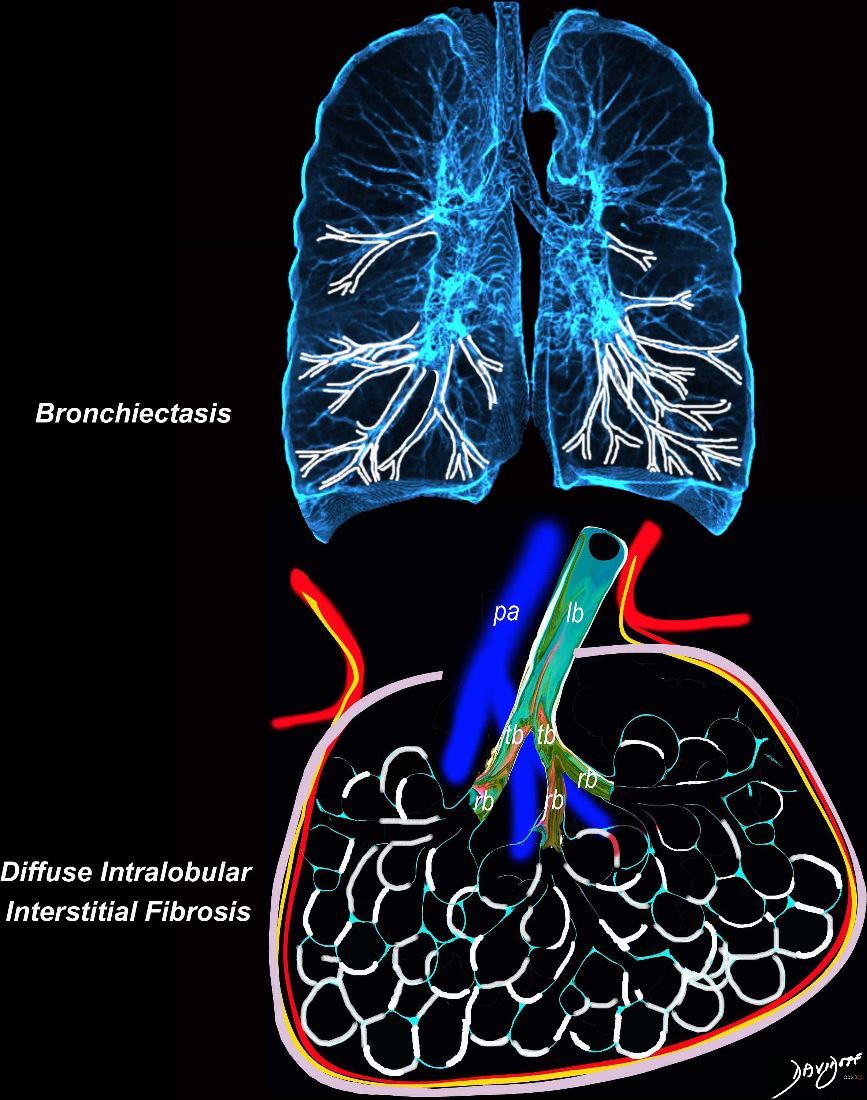
Broncho vascular and inter- alveolar interstitial fibrosis dominantly in the lower lobes but affecting the middle and upper lobes to lesser extent resulting in bronchiectasis and reticulations. The overall increase in density results in ground glass changes
Ashley Davidoff MD TheCommonvein.net lungs-0738 NSIP
When there are extensive interstitial fibrotic changes in the interstitial compartments of the lung which include the and the interalveolar septa, and the supporting interstitium of the lung between the acini and small airways, the overall net density of the region of involvement will be gray, and when adjacent to the black air filled airways, a ground glass appearance will be apparent
Ashley Davidoff
TheCommonVein.net
ssb = subsegmental bronchiole
tb = terminal bronchiole
rb = respiratory bronchiole
as = alveolar duct
as = alvelar sac
is = anteralveolar septum
Ashley Davidoff
TheCommonVein.net lungs-00682
COVID 19
The virus replicates and invades more cells of the alveoli
As COVID-19 causes inflammation of the the lungs, infected fluid fills the lungs thus disrupting gas exchange.
Ashley Davidoff TheCommonVein.net lungs-0043
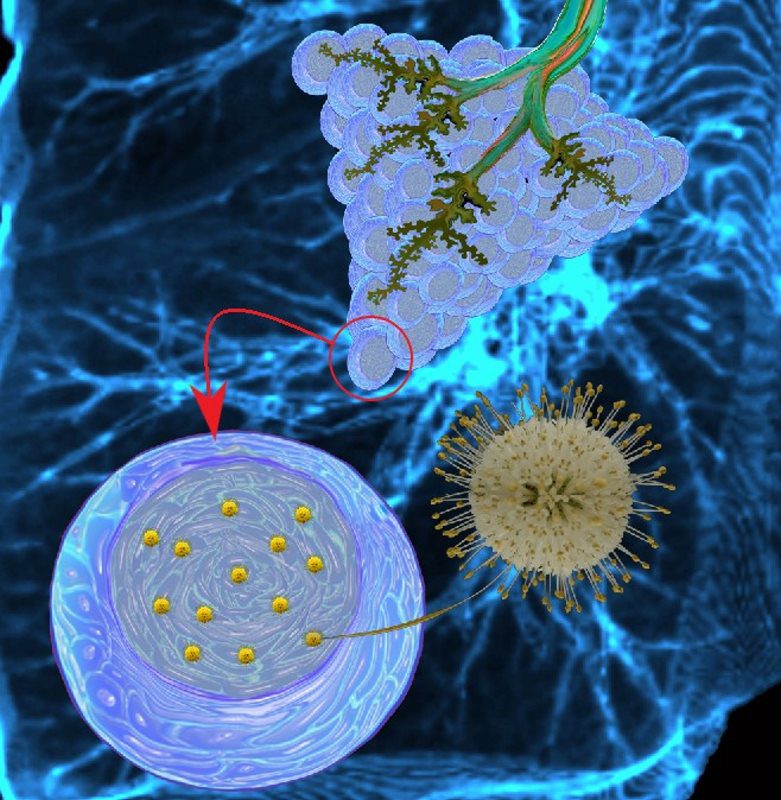
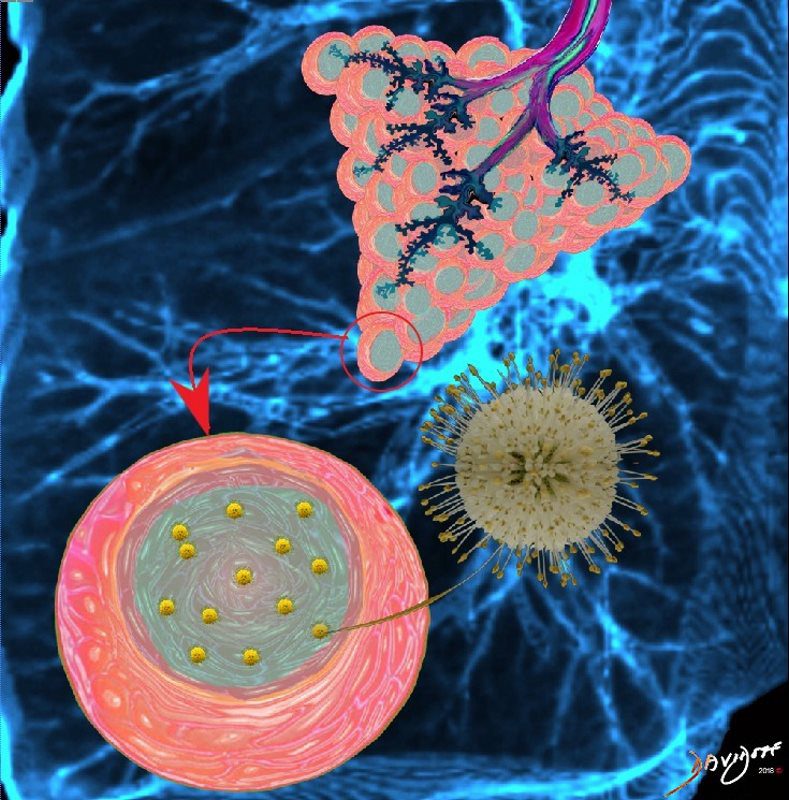
Corona virus invades the cells of the alveoli by using its spike glycoproteins. These spike proteins attach to the cell membrane and the virus can then enter the cell.
Ashley Davidoff TheCommonVein.net lungs-0042
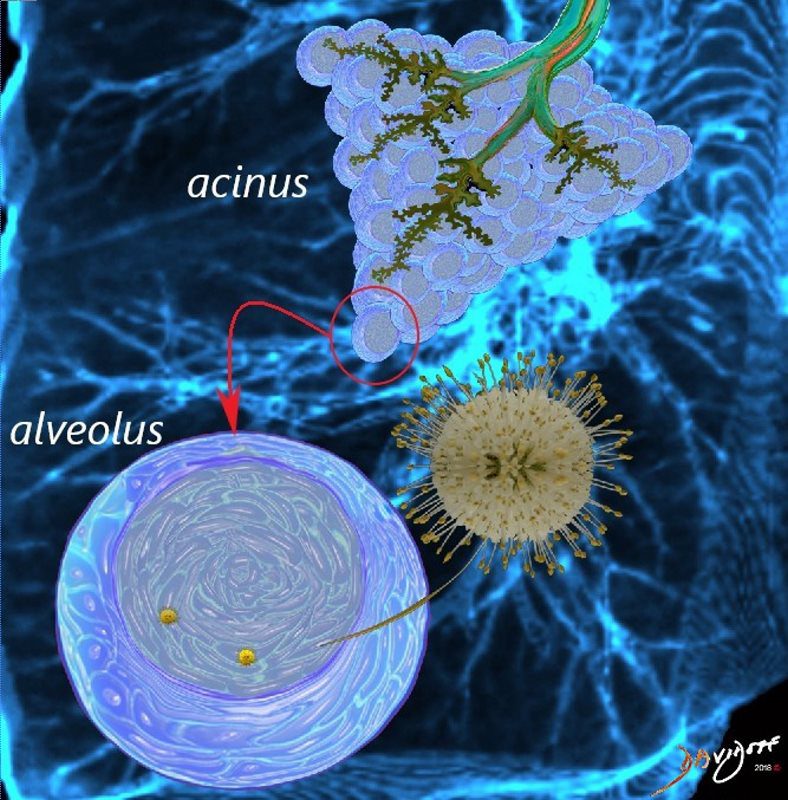
Corona virus invades the cells of the alveoli by using its spike glycoproteins. These spike proteins attach to the cell membrane and the virus can then enter the cell.
Ashley Davidoff TheCommonVein.net lungs-0040

The virus enters the lungs and travels to the smallest parts of the lungs, tiny lung sacs called the alveoli where oxygen exchange takes place
Ashley Davidoff TheCommonVein.net lungs-0039

Ashley Davidoff MD TheCommonVein.net lungs-0057
Eosinophilic Pneumonia
Ashley Davidoff TheCommonVein.net
lungs-0756b01
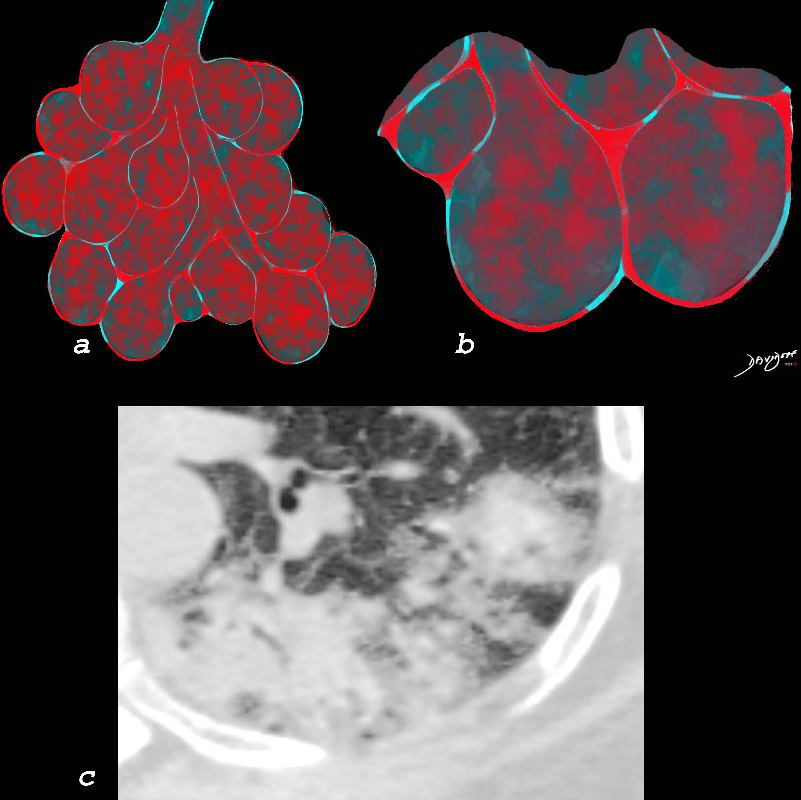
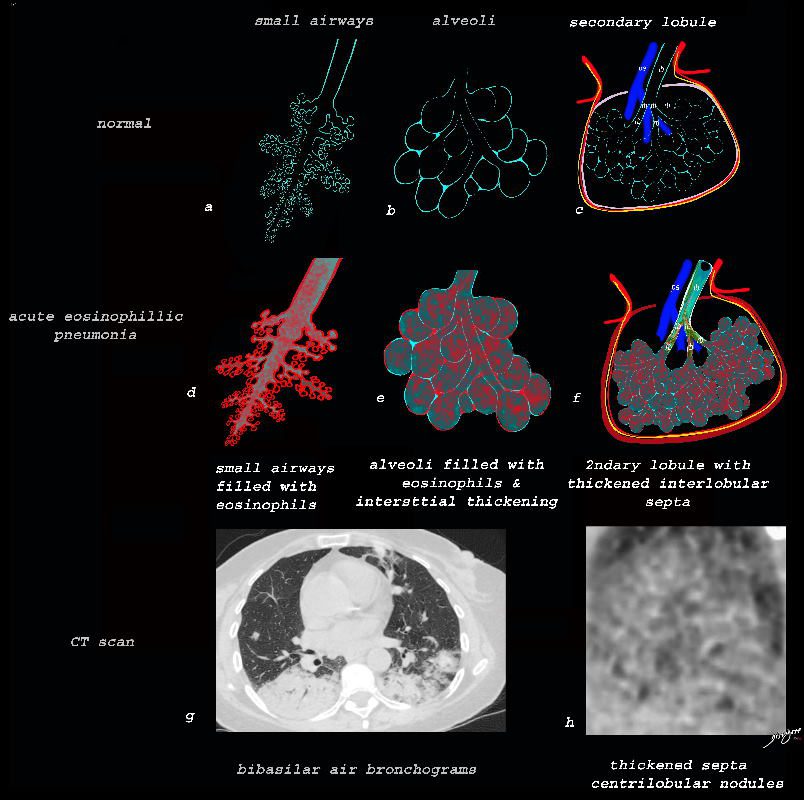
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows a peripheral consolidation in the left upper lobe
Ashley Davidoff MD The CommonVein.net lungs-0764
This diagram reveals the important structural changes in the secondary lobule that includes filling of the alveoli with eosinophils and proteinaceous and fibrinous exudate as well as infiltration into the alveoar septa and interstitium (redwalls) . An important component of the disease is the thickening of the interlobular septa (maroon) which results in Kerley B lines and an interstitial pattern reminiscent of cardiogenic interstitial edema.
Ashley Davidoff TheCommonVein.net lungs-0758
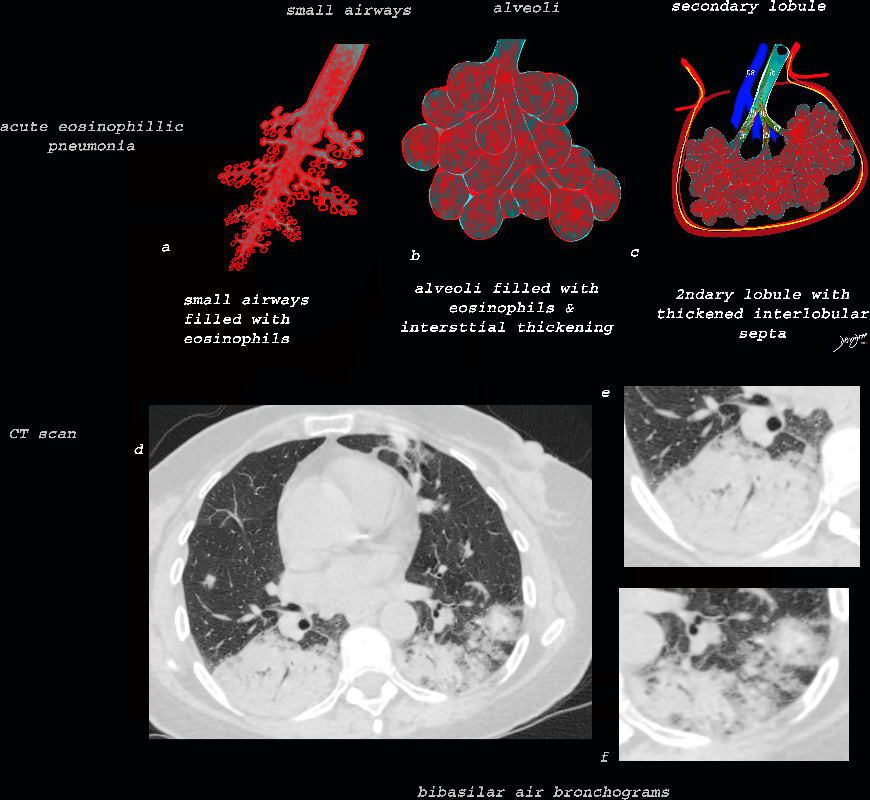
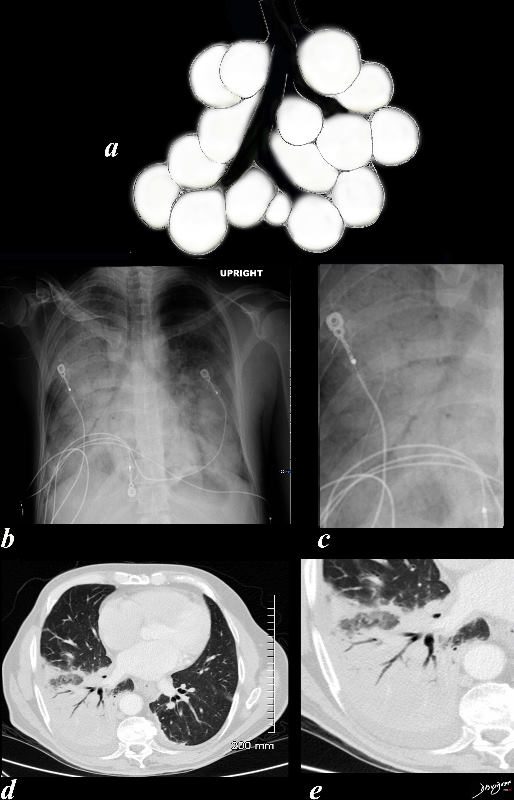
As the disease advances the small airways, and alveoli, get progressively filled with eosinophils, inflammatory cells and fluids resulting in consolidation. This image reveals progressive filling of the small airways, (a) alveoli, (b) and secondary lobules (c) with eosinophils and products of inflammation resulting in multi-segmental consolidations (d), in the lung bases, with air bronchograms at the right base (e), and less dense consolidation at the left base (f)
Ashley Davidoff MD The CommonVein.net lungs-0763
Ashley Davidoff TheCommonVein.net lungs-0757b