
- 80 y.o. male non smoker with a
- history of HTN, T2DM, COPD vs IPF, paroxysmal atrial fibrillation
- childhood TB (treated as a teenager Brazil)
- SX
- fatigue, weakness and weight loss.
- driven by his respiratory symptoms,
- dyspnea on exertion and fatigue since
- COVID 1 year
Respiratory Disease:#COPD
no prior PFTs for review.
- COVID 1 year
- no wheezing or prolonged expiratory phase on exam.
- Interstitial lung disease
- CT 1 year prior
- Interval increase in lower lung subpleural predominant reticular opacities,
- traction bronchiectasis
- Unchanged upper lobe traction bronchiectasis, volume loss and calcified granulomas, .
- CT 1 year prior
- fatigue, weakness and weight loss.
- Current CT
- High-resolution CT scan without contrast
- predominant background disease is
- bronchiectasis and bronchiolectasis
- dominant in the lower lobes but also present in the middle lobe.
- `The trachea is mildly dilated (2.5 cm) and the right and left mainstem bronchi are also dilated.
- predominant background disease is
- interstitial fibrotic component is not dominant and the findings suggest that the bronchiectasis and bronchiolectasis are responsible for the hyperinflation and the clinical presentation.
- no evidence of centrilobular emphysema
- calcified hilar nodes confirm the clinical history of prior tuberculosis which may have in part related to the upper lobe broncholiths.
- right atrial enlargement but without evidence of pulmonary hypertension
- High-resolution CT scan without contrast
-
- COPD Non Smoker
Hyperinflation Bronchiectasis Latent TB
- COPD Non Smoker
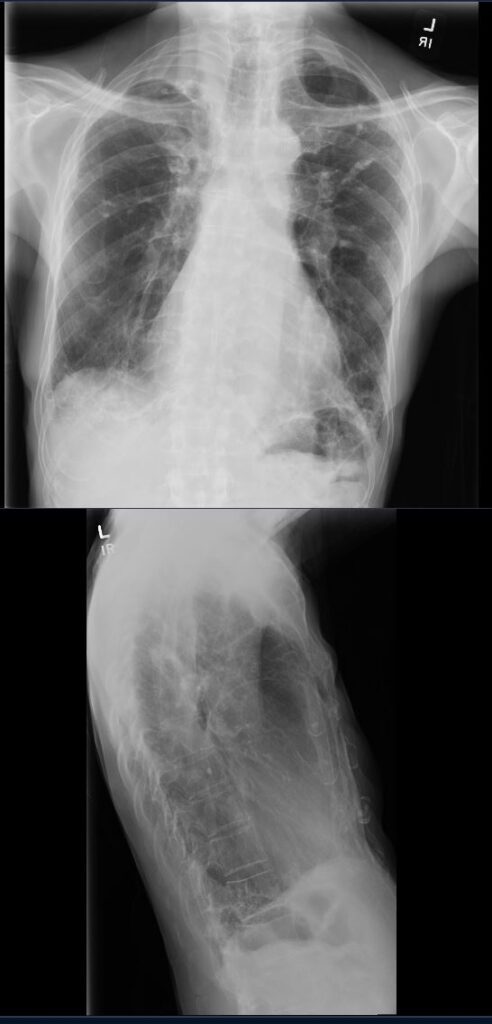
80- year-old non-smoker with childhood history of treated TB, presents with chronic dyspnea
CXR in PA and lateral projections, shows hyperinflation and diffuse interstitial coarsening of the lung markings with upward retraction of the right hilum
Ashley Davidoff TheCommonVein.net 292Lu 136625
COPD Hyperinflation Bronchiectasis Broncholiths
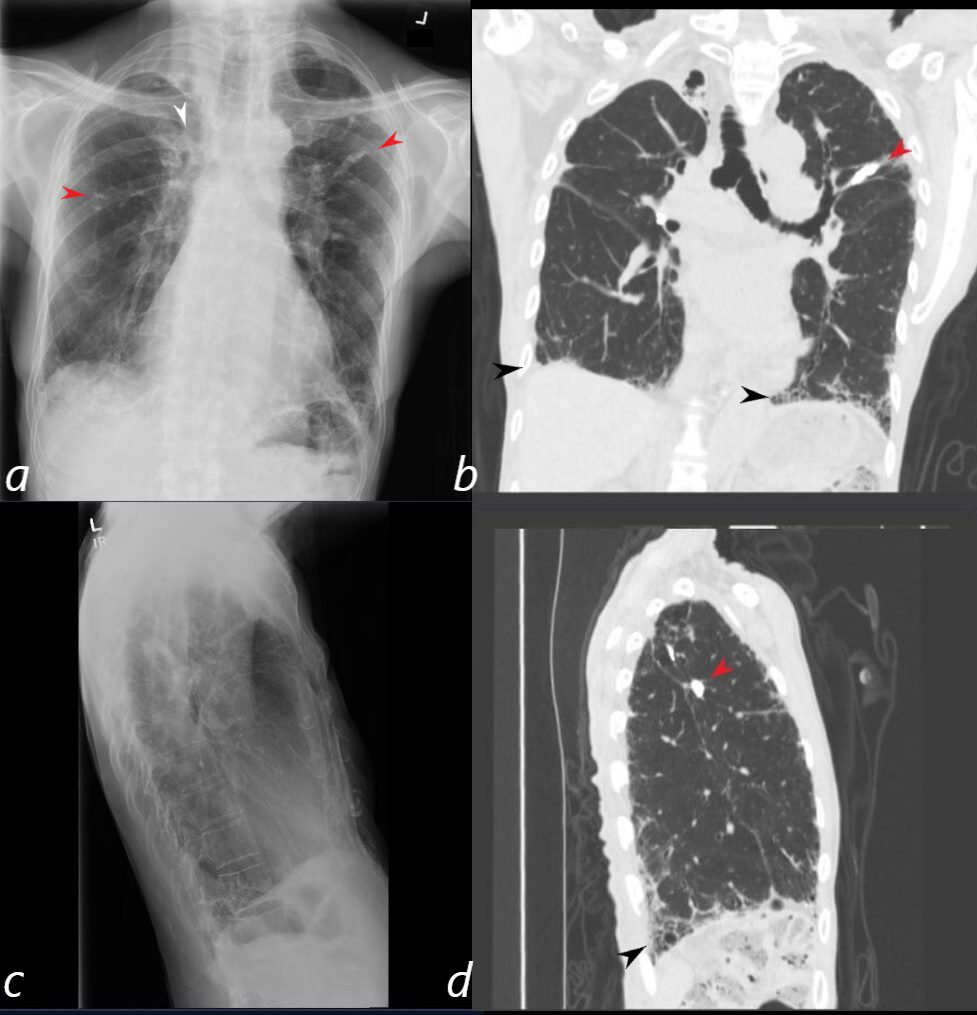
80- year-old non-smoker with childhood history of treated TB, presents with chronic dyspnea
Corresponding images of a CXR and CT scan show hyperinflation and diffuse interstitial coarsening of the lung markings with upward retraction of the right hilum (a, white arrowhead) a calcified broncholith in the LUL (b, and d red arrowheads) a calcified granuloma in the RUL (a, red arrowhead) and basilar interstitial process (black arrowheads b and d)
Ashley Davidoff MD TheCommonVein.net 292Lu 136625cL
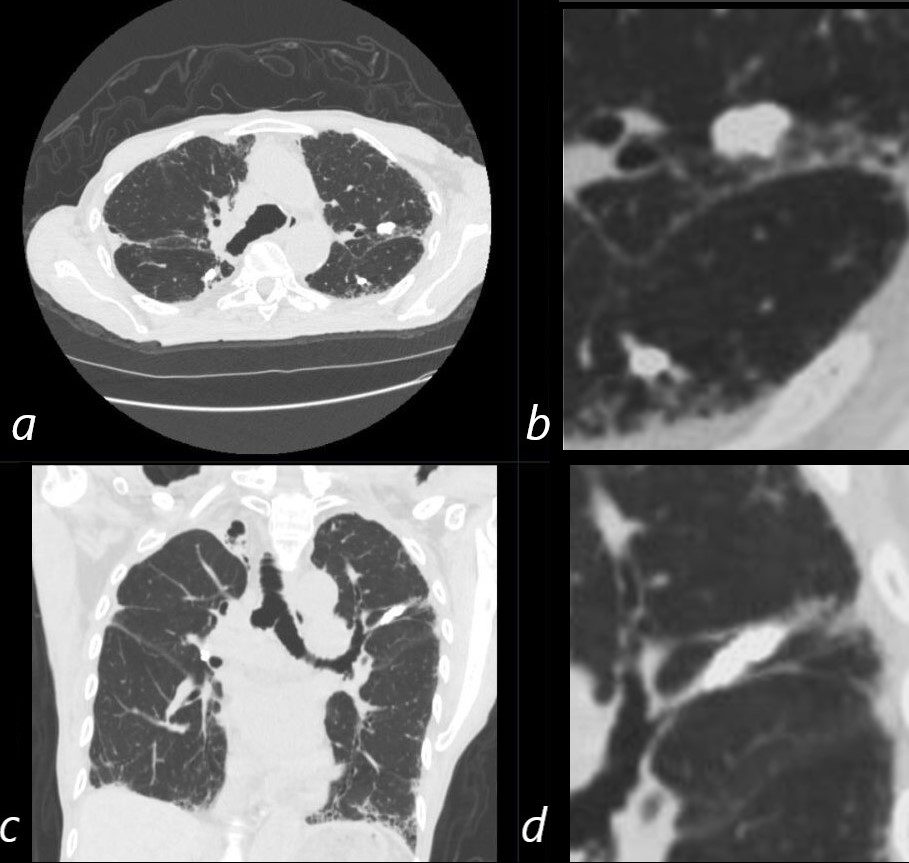
CT in axial and coronal projections of an 80- year-old non-smoker with childhood history of treated TB, shows multiple calcifications with tubular morphology (c and d) consistent with broncholiths. There is interstitial coarsening of the lung markings
Ashley Davidoff MD TheCommonVein.net 292Lu 136626c01
Right Apex Latent TB and Bronchiectasis
80- year-old non-smoker with childhood history of treated TB, presents with a chronic cough
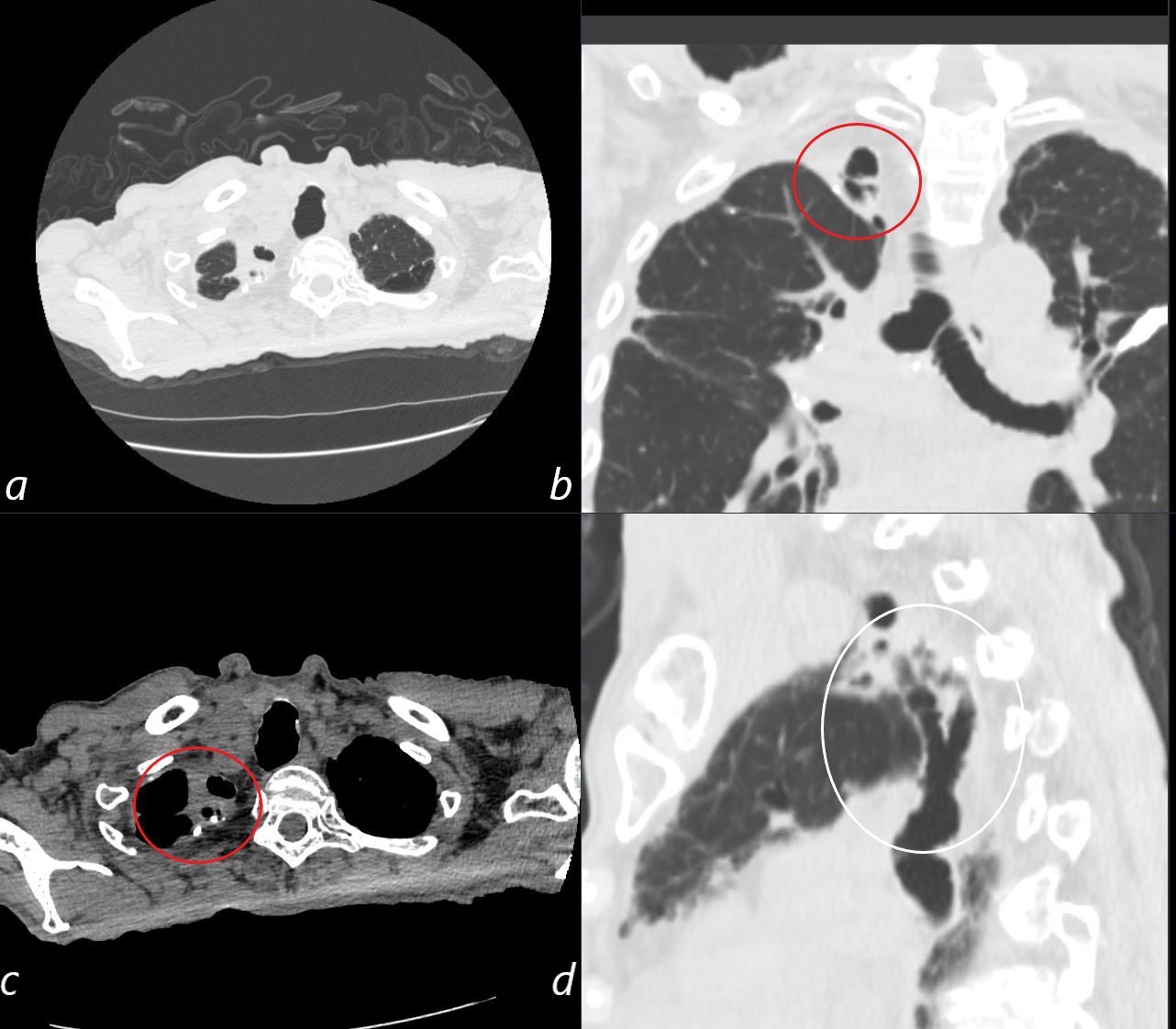
Axial images (a, and b) show chronic granulomatous changes (red ring) with calcification and fibrosis, confirmed in the coronal projection (b, red ring)
The sagittal projection (d) shows bronchiectasis of the superior and posterior segmental bronchi to the left upper lobe (d, white ring)
Ashley Davidoff MD TheCommonVein.net 292Lu 136627cL
COPD Bronchiectasis Latent TB
Scarring No Emphysema
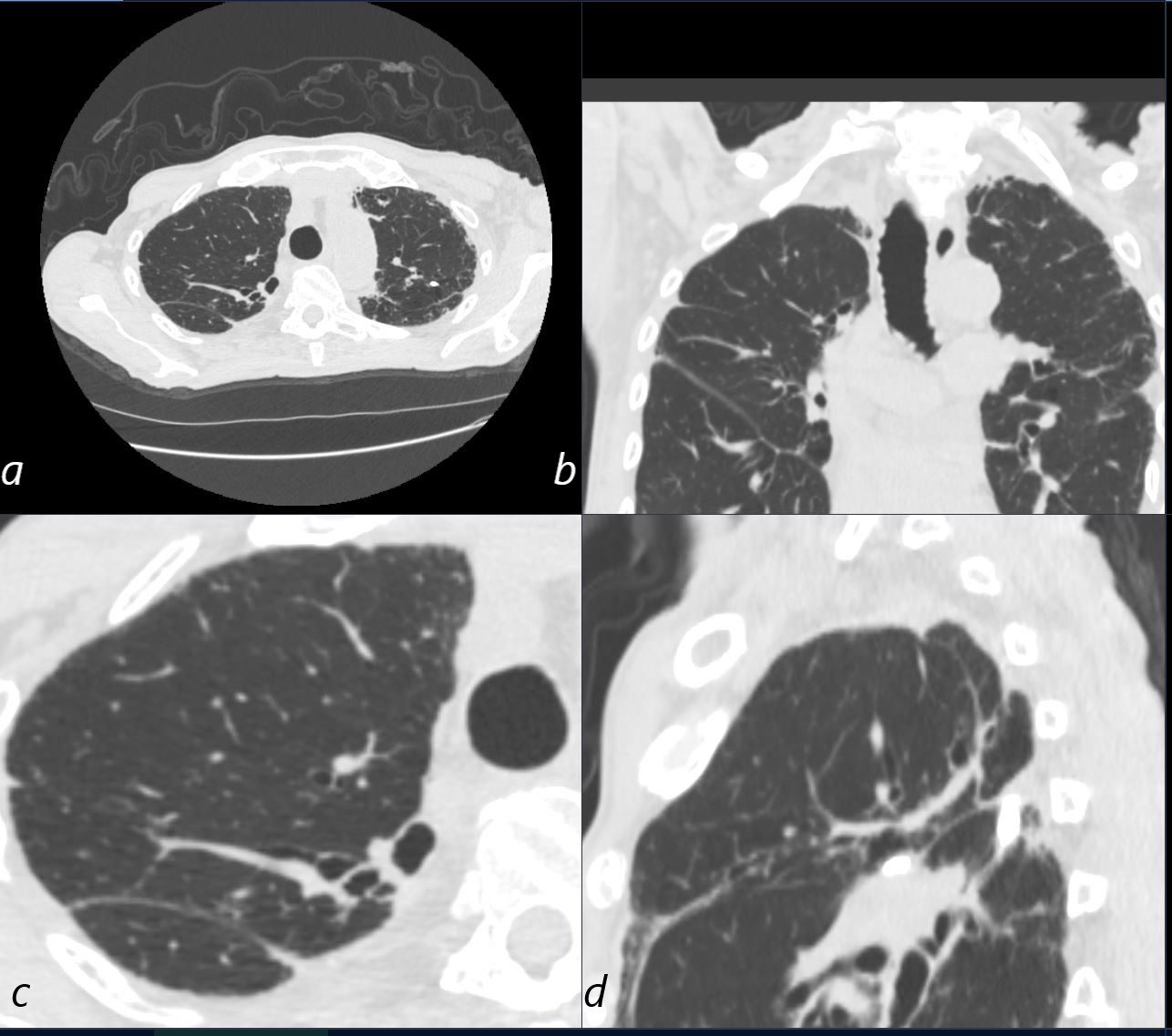
80- year-old non-smoker with childhood history of treated TB, presents with a chronic cough
CT scan of the upper lobes in the axial (a, c), coronal (b) and sagittal (d) planes, show no evidence of centrilobular emphysema, but with evidence of thin fibrotic bands exemplified in d and perhaps some overall lucency indicating hyperinflation.
Ashley Davidoff MD TheCommonVein.net 292Lu 136628cL
Calcified Hilar and Mediastinal Nodes
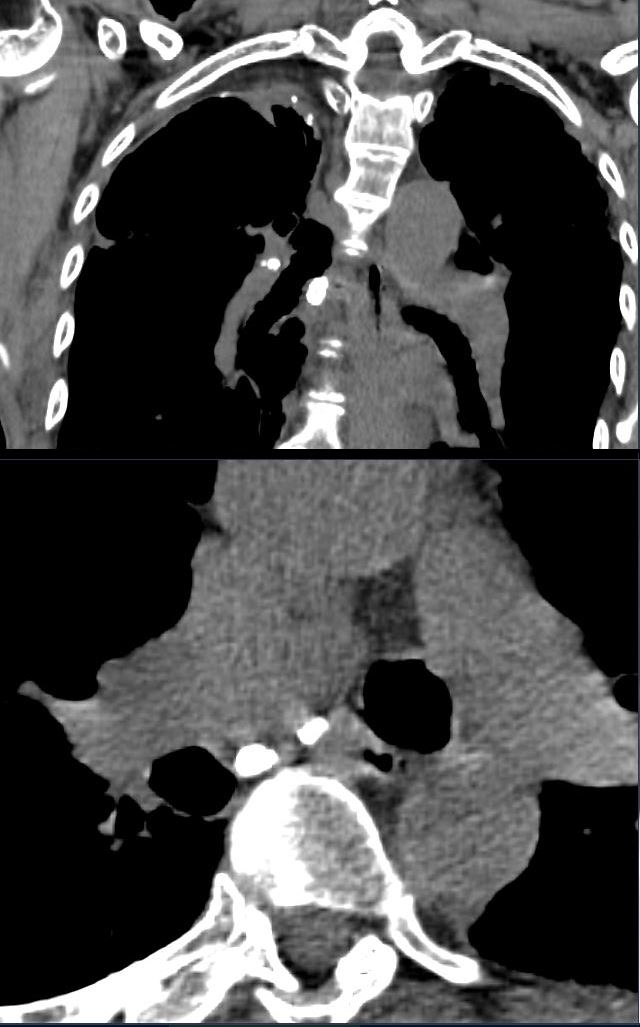
80- year-old non-smoker with childhood history of treated TB, presents with a chronic cough
CT scan in the coronal (upper image) and axial (lower image) planes show calcified hilar and mediastinal nodes consistent with chronic granulomatous disease
Ashley Davidoff MD TheCommonVein.net 292Lu 136629c
Basilar Bronchiolectasis
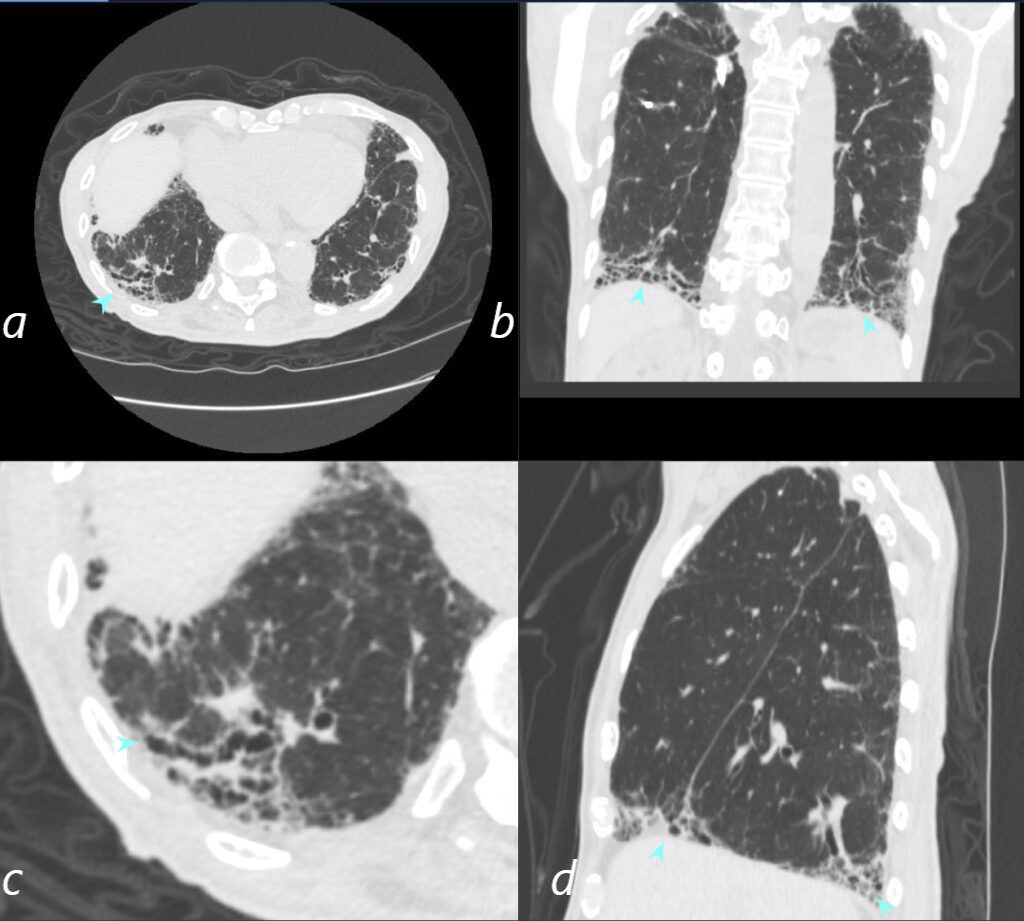
80- year-old non-smoker with childhood history of treated TB, presents with a chronic cough
CT scan in the axial plane (a, magnified in b) shows a wedge shaped conglomerate of dilated bronchioles (blue arrowheads. The coronal image (b) and sagittal image b and c) again show the wedge shaped regions of bibasilar bronchiolectasis
Ashley Davidoff TheCommonVein.net292Lu 136631cL
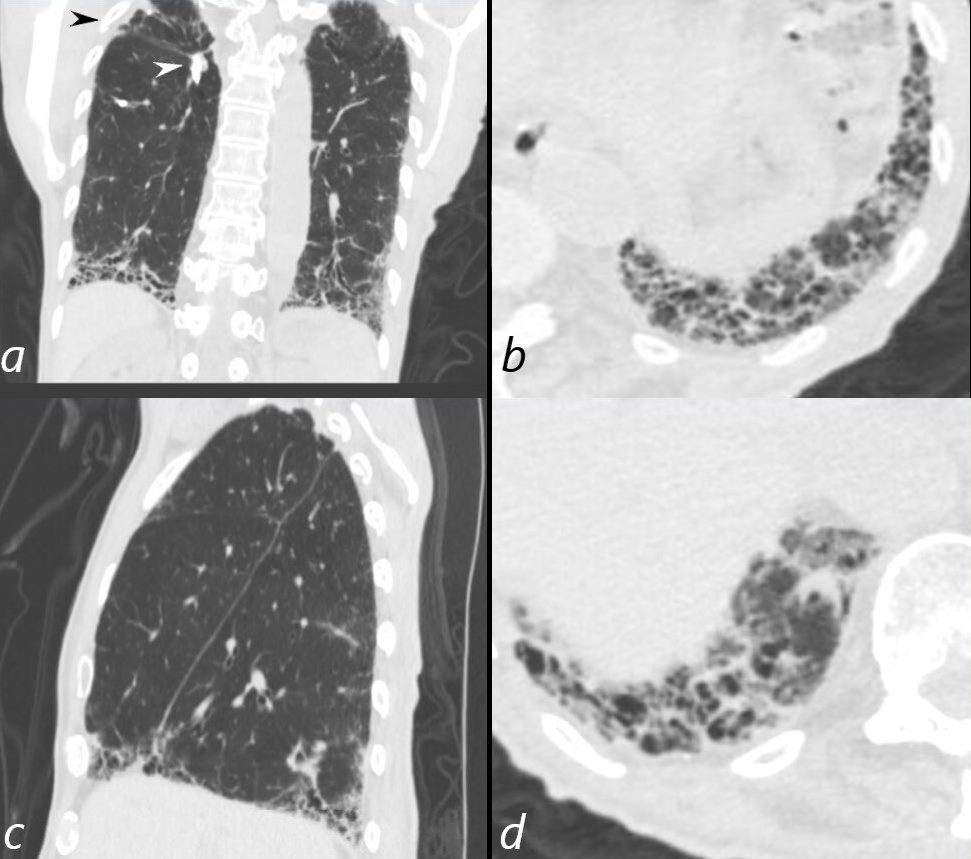
80- year-old non-smoker with childhood history of treated TB, presents with a chronic cough
CT scan in the coronal plane (a) shows volume loss in the right upper lobe (black arrowhead) and a subtending calcified broncholith (white arrowhead, a).
Basilar peripheral bronchiolectasis is demonstrated in the coronal (a) and sagittal planes (b) , and magnified in the axial planes at the left posterior recess (c) and right posterior recess (d)
Ashley Davidoff MD TheCommonVein.net 292Lu 136632cL
Flattened Right Heart Border by Hyperinflation
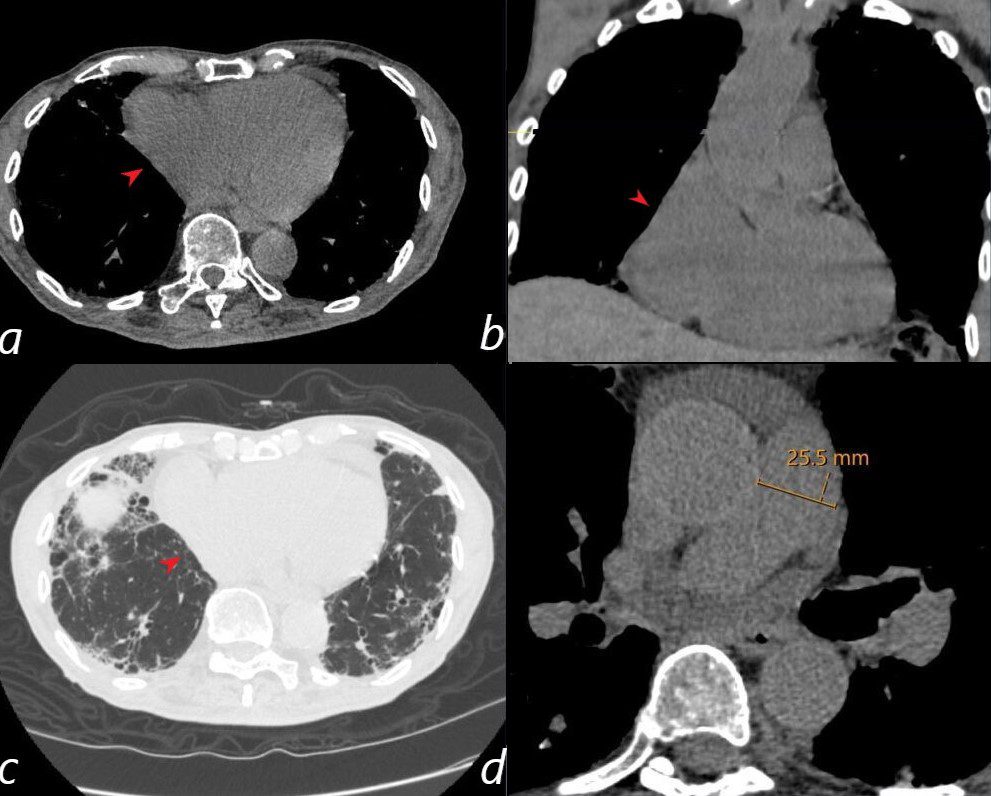
80- year-old non-smoker with childhood history of treated TB, presents with a chronic cough
CT scan in the axial plane shows flattening of its outer border caused by the hyperinflated lungs (a, red arrowhead) The coronal CT (b) confirms the enlargement of the RA and the flattening of its lateral border (red arrowhead)
The axial CT using lung windows, shows the mild interstitial fibrotic changes with ground glass changes and bronchiolectasis in the anterior lung field. (c) The red arrowhead shows flattening of the RA.
Image d, shows a normal sized main pulmonary artery.
Ashley Davidoff MD TheCommonVein.net 292Lu 136633cL