
Septic Emboli:
- Septic emboli are infected thromboembolic material originating from a distant infectious source, traveling via the bloodstream, and lodging in the pulmonary vasculature.
- They result in localized infection and inflammation, leading to pulmonary parenchymal damage.
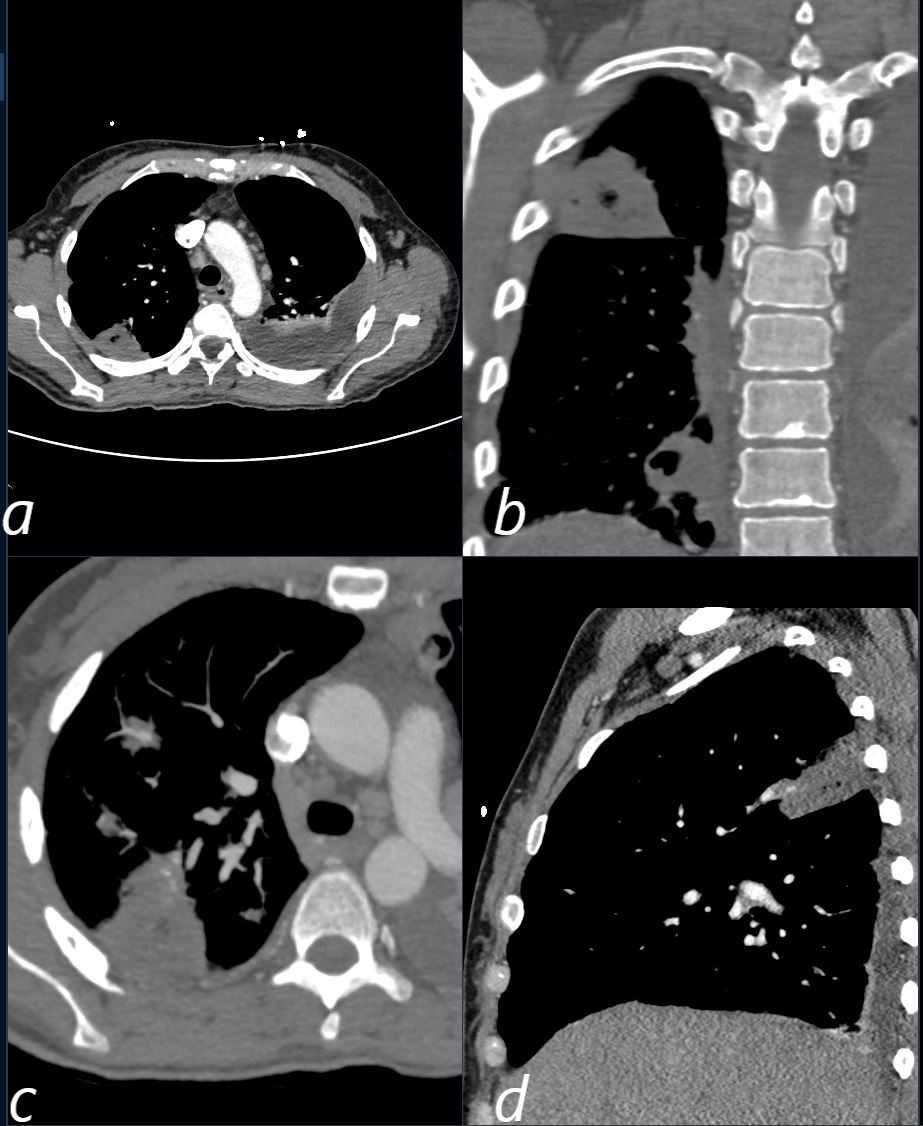
CT scan in a 39 year old female with endocarditis presents with a fever and right sided chest pain.
Multiple views in axial (a,c) coronal (b) and sagittal reveals the presence of a wedge shaped consolidation with cavitation confirming the presence of an infected and cavitating infarction in the posterior segment of the left upper lobe. A loculated effusion is noted at the left base.
Ashley Davidoff TheCommonVein.net
b11422c
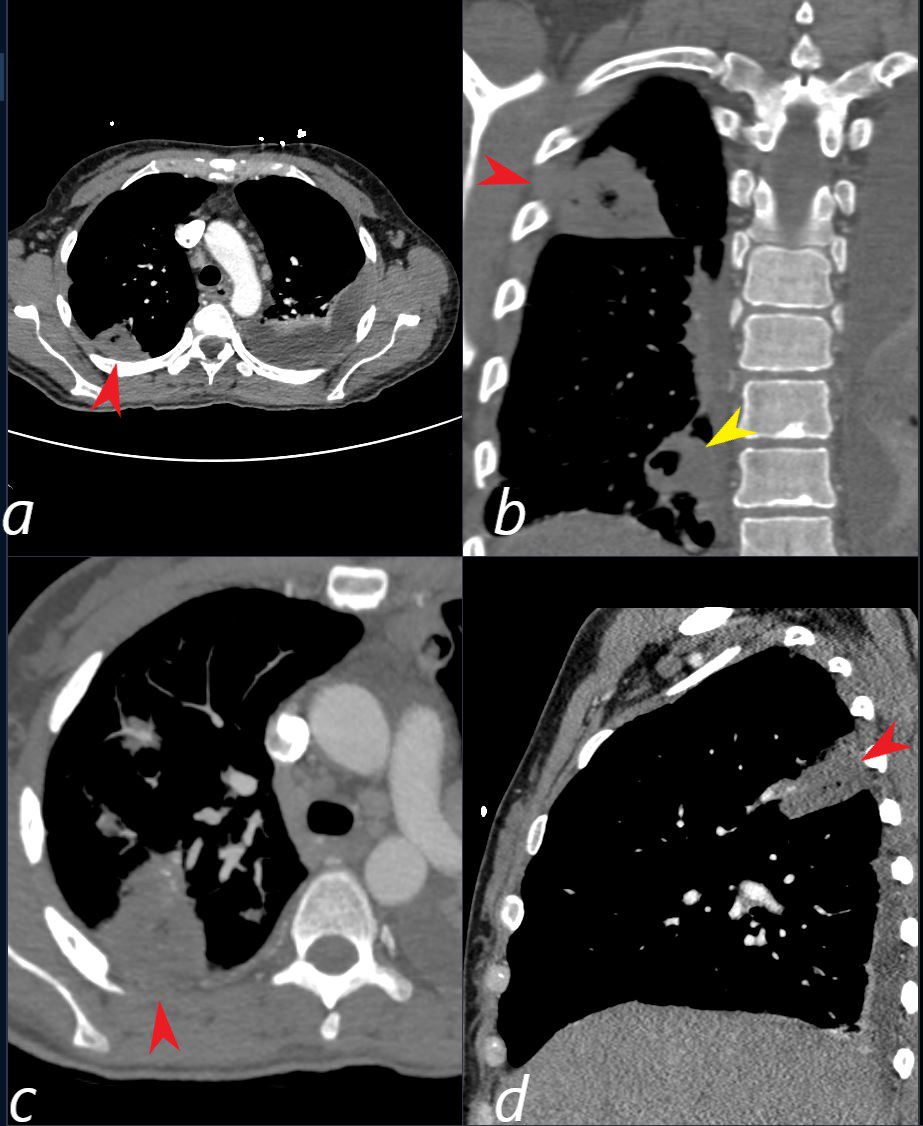
CT scan in a 39 year old female with endocarditis presents with a fever and right sided chest pain.
Multiple view in axial (a,c) coronal (b) and sagittal confirm the presence of a wedge shaped consolidation with cavitation (red arrowhead a,b,c, and d) confirming the presence of an infected and cavitating infarction in the posterior segment of the left upper lobe. A second similar subsegmental infarct and abscess (yellow arrowhead, is noted in the right lower lobe (b yellow arrowhead) . A loculated effusion is noted at the left base.
Ashley Davidoff TheCommonVein.net b11422cL
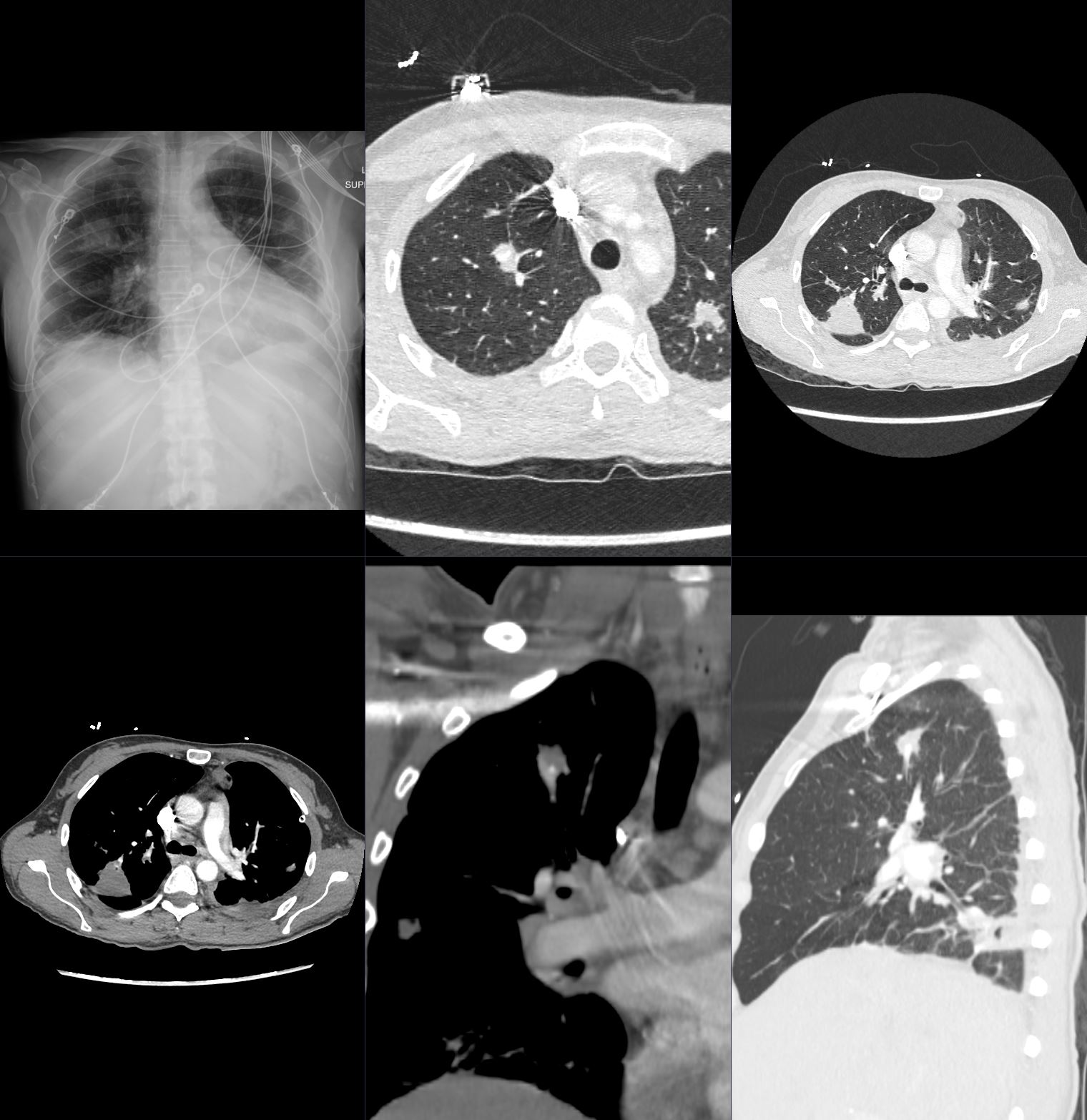
Bacterial Endocarditis (BE) and Mycotic Pseudoaneurysm Lung Abscess 39F
Ashley Davidoff TheCommonVein.net b11422b02

Ashley Davidoff MD TheCommonvein.net 24f PE Hampton’s hump 003

Ashley Davidoff MD TheCommonvein.net 24f PE Hampton’s hump 002
Causes
- Primary Infections:
- Infective endocarditis (most common).
- Infected venous catheters.
- Soft tissue infections (e.g., abscesses, IV drug use-related infections).
- Septic thrombophlebitis.
- Organisms: Staphylococcus aureus (including MRSA), Streptococcus spp., and gram-negative organisms.
Results
- Small peripheral pulmonary infarcts with subsequent infection and abscess formation.
- Multiple nodules, cavitation, or consolidations.
- Complications:
- Empyema.
- Pleural effusion.
- Bronchopleural fistulas.
Diagnosis
- Clinical Presentation:
- Fever, chills, and malaise.
- Dyspnea, chest pain, or hemoptysis.
- History of risk factors (e.g., IV drug use, endocarditis, infected devices).
- Imaging:
- Chest X-ray (CXR):
- Multiple, bilateral nodules often in the lung periphery.
- Possible cavitation and air-fluid levels.
- May show pleural effusions or wedge-shaped infarcts.
- Chest CT:
- Multiple nodules or masses, often with cavitation.
- Peripheral and subpleural distribution.
- Feeding vessel sign: visible pulmonary artery leading to the lesion.
- Associated findings: empyema, pleural thickening, infarcts.
- Chest X-ray (CXR):
- Laboratory Tests:
- Elevated inflammatory markers (e.g., CRP, ESR, WBC count).
- Positive blood cultures identifying the pathogen.
- Echocardiography for endocarditis (transthoracic or transesophageal).
Treatment
- Antibiotics:
- Broad-spectrum coverage initially, adjusted based on blood culture results.
- Prolonged duration (e.g., 4–6 weeks for endocarditis-related septic emboli).
- Source Control:
- Remove or treat the primary source of infection (e.g., infected devices, abscess drainage).
- Surgical Intervention:
- Rarely required unless complications such as empyema or persistent infection arise.
Pearls
- Peripheral nodules with cavitation in IV drug users should raise suspicion for septic emboli.
- Always investigate for an underlying source of infection, especially endocarditis or IV drug use.
- Feeding vessel sign on CT is a characteristic finding.
- Early diagnosis and source control are critical to prevent complications.