
Metastatic Prostate Cancer with Blastic and Lytic Bone Metastases and Acute Right Heart Failure
45-year-old male with metastatic prostate cancer and extensive osseous metastases complicated by pathologic fracture, presents with multiorgan failure, and acute pulmonary hypertension resulting in right ventricular (RV) failure and heart failure.
Metastatic Prostate Cancer with Blastic and Lytic Bone Metastases and Acute Right Heart Failure
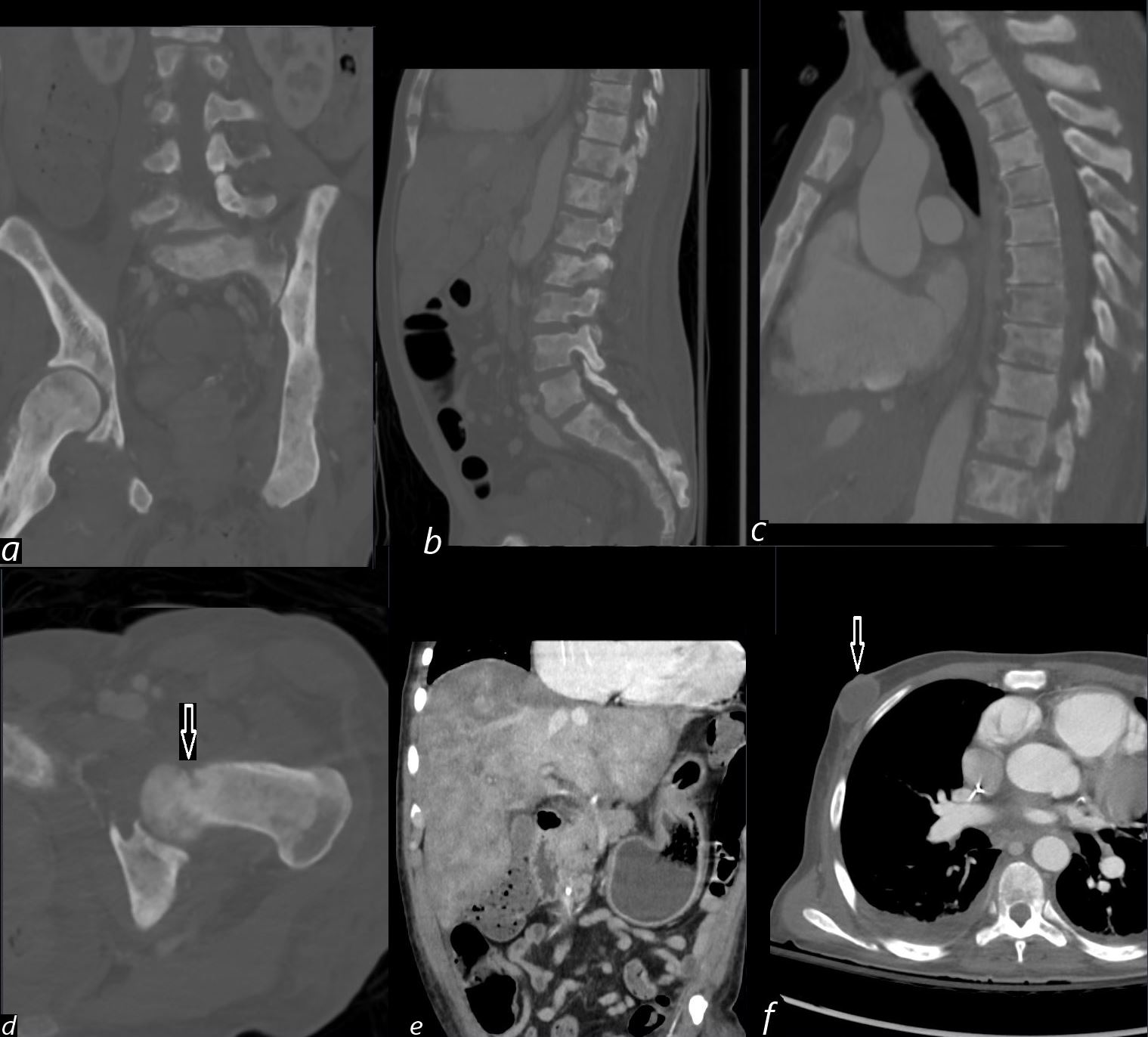
A 45-year-old male with metastatic prostate cancer presenting with acute right heart failure. CT shows blastic and lytic bone metastases to the pelvis (a) and spine ( b, d) with a pathologic fracture of the lesser trochanter (d, arrow). Liver metastases are also noted (e) along with an incidental breast abscess (f, arrow).
Comment:
The combination of blastic and lytic bone metastases is characteristic of advanced prostate cancer. The pathologic fracture and metastatic liver involvement highlight the extent of systemic disease. The acute right heart failure may be secondary to pulmonary hypertension or extensive metastatic burden.
Ashley Davidoff MD TheCommonVein.net b11488-05L (308Lu).
Acute Right Heart Failure
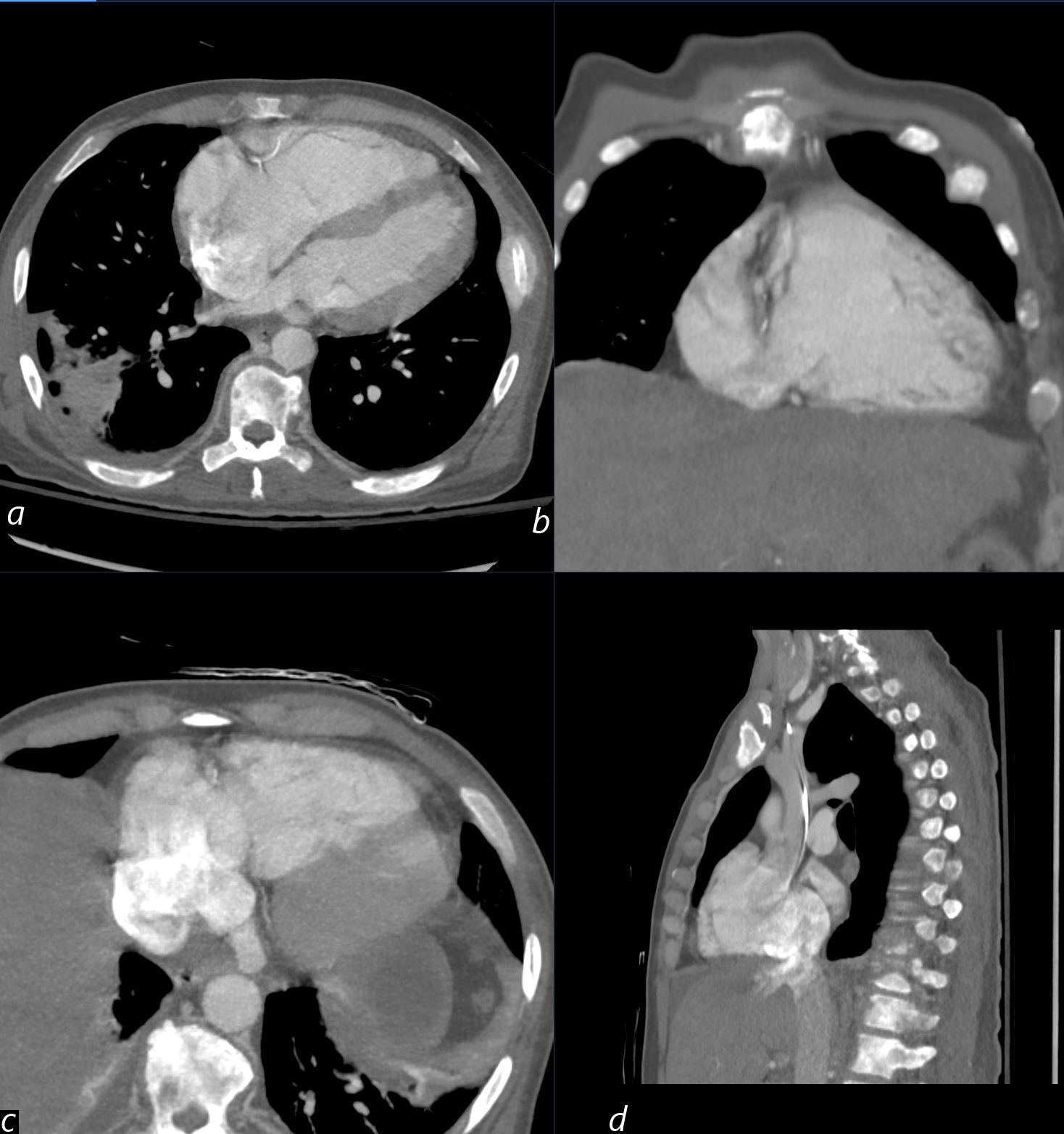
A 45-year-old male with metastatic prostate carcinoma presents with findings of acute right ventricular failure (RVF). CT of the chest (axial mid-right ventricle, sagittal, and coronal projections) show right atrial enlargement (RAE)(c), right ventricular enlargement (RVE) (a,b,c) , and tricuspid regurgitation (TR) (d).
Additional findings include interatrial septal bowing (a) and a straightened interventricular septum,(a) consistent with right heart strain and pressure overload. A wedge-shaped opacity in the right lower lobe (RLL) abutting the pleura is also noted, raising the possibility of an isolated pulmonary infarction but without evidence of acute PE.
Ashley Davidoff MD TheCommonVein.net (b11488) (308Lu).
Comment:
Acute right ventricular failure (RVF) often presents with right atrial dilation, right ventricular enlargement, and a straightened interventricular septum, which occurs due to pressure overload in the right heart chambers. Interatrial septal bowing toward the left atrium suggests elevated right atrial pressure, commonly associated with conditions such as pulmonary embolism, pulmonary hypertension, or severe tricuspid regurgitation (TR). The presence of a wedge-shaped opacity in the right lower lobe adjacent to the pleura raises concern for a pulmonary infarction, which can occur due to pulmonary embolism and subsequent vascular obstruction. Further correlation with perfusion imaging or echocardiography may be warranted.
A 45-year-old male presents with findings of acute right ventricular failure (RVF).
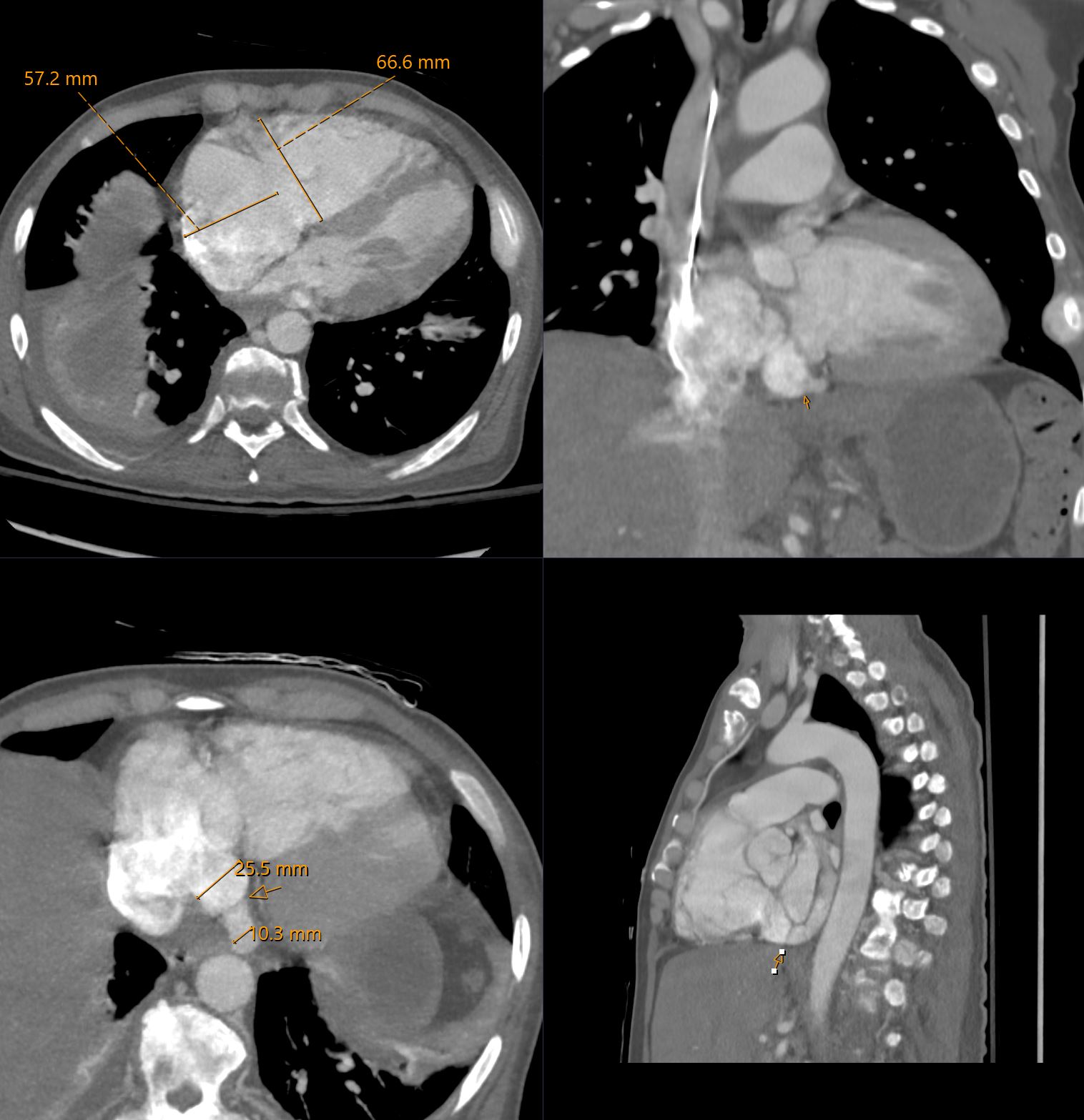
CT of the chest (axial mid-right ventricle, sagittal, and coronal projections) shows right atrial enlargement (RAE) measuring 57mm (a), right ventricular enlargement (RVE) measuring 67mm (a, c, d), and tricuspid regurgitation (TR) (b). Additional findings include a straightened interventricular septum (a) and a dilated coronary sinus measuring 25mm as it enters the RA and 10mm upstream from the Thebesian valve. These findings are consistent with right heart strain and pressure overload. This is a good example of the Thebesian valve at the downstream end of the coronary sinus (arrows b, c, and d). A subpleural effusion associated with compressive atelectasis is noted in the right lower lobe (RLL)(a).
Ashley Davidoff MD TheCommonVein.net (b11488)(308Lu).
Comment:
Acute right ventricular failure (RVF) often presents with right atrial dilation, right ventricular enlargement, and a straightened interventricular septum, which occurs due to pressure overload in the right heart chambers. Interatrial septal bowing toward the left atrium suggests elevated right atrial pressure, commonly associated with conditions such as pulmonary embolism, pulmonary hypertension, or severe tricuspid regurgitation (TR). Additionally, the dilated coronary sinus and the Thebesian valve finding emphasize right heart strain with increased venous return, commonly observed in RV pressure overload states.
Metastatic Prostate Cancer with Bone and Liver Metastases Presenting with Acute Right Heart Failure and Pulmonary Hypertension
A 45-year-old male with a diagnosis of metastatic prostate cancer involving the bone and liver presents with acute right heart failure and pulmonary hypertension.
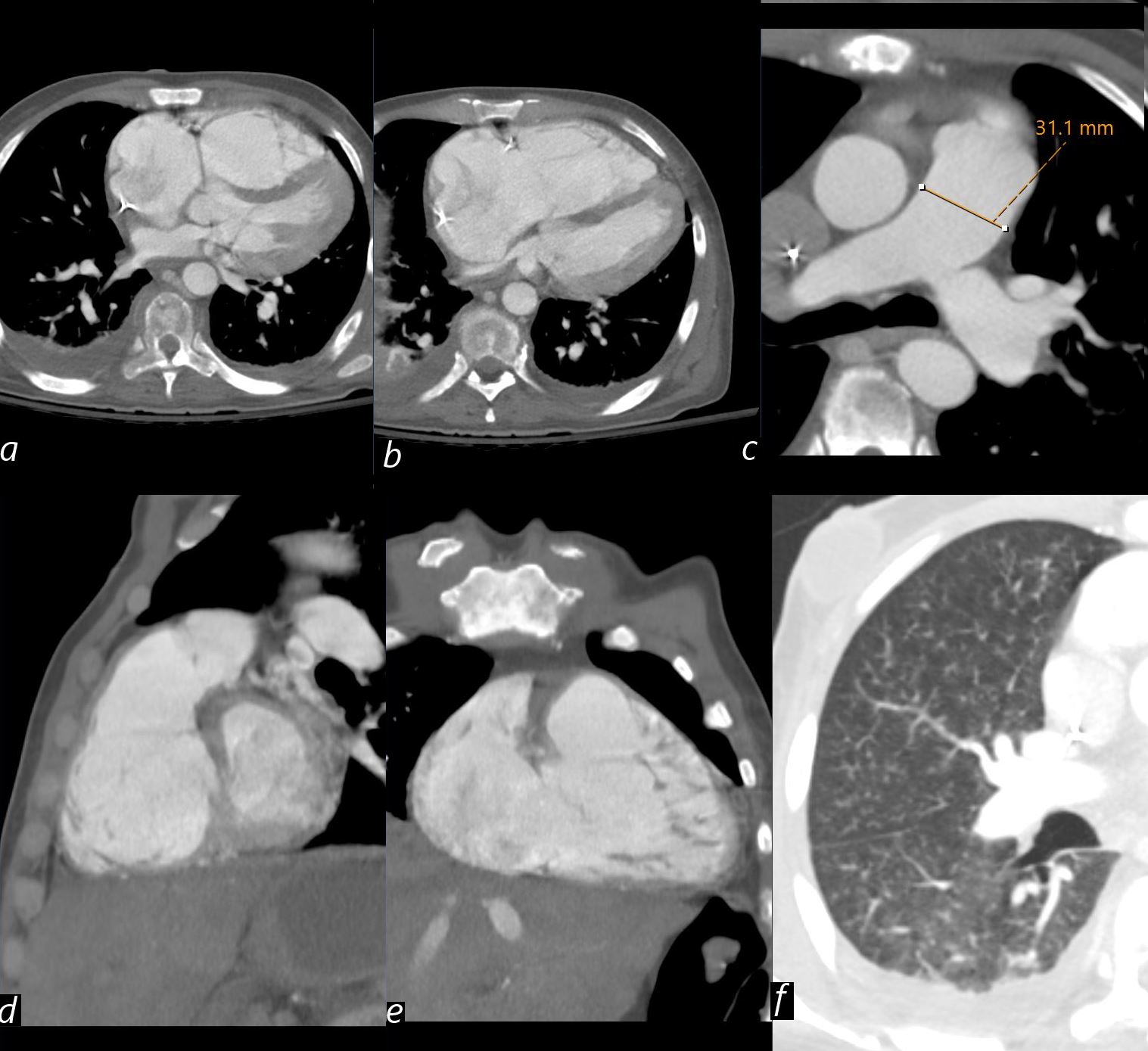
CT shows significant septal bowing toward the right ventricle (RV) impinging on the left ventricular (LV) cavity and a small left atrium (a, axial).
Right atrial enlargement (RAE), right ventricular enlargement (RVE), a straightened interventricular septum, and a small LV cavity are observed (b, axial).
Pulmonary artery dilatation to 31 mm, consistent with pulmonary arterial hypertension, is noted (c, axial).
Right atrial enlargement (RAE), right ventricular enlargement (RVE) again noted in (d, sagittal and e, coronal) Lung windows (f, axial) reveal extensive micronodularity.
possibly representing micrometastases and contributing to acute right ventricular failure.
Comment:
Septal bowing, right atrial and ventricular enlargement, and pulmonary artery dilation suggest severe right heart strain secondary to pulmonary hypertension, likely driven by extensive metastatic burden with suspected micrometastases.
Ashley Davidoff MD TheCommonVein.net b11488-04 (308Lu).
Echocardiogram Showed
- Severely enlarged RV with apex-forming RV and flattening of the ventricular septum in both systole and diastole, consistent with RV pressure and volume overload.
- Underfilled left ventricular (LV) cavity, suggestive of reverse Bernheim effect.
- RV basal diameter measured at 5.5 cm.
- RV function significantly reduced, with preserved function limited to the ape
What is the Reverse Bernheim Effect?
The reverse Bernheim effect occurs when right ventricular (RV) hypertrophy or dilation compresses the left ventricular (LV) cavity, leading to impaired LV filling and reduced LV output. This phenomenon arises due to the abnormal displacement of the interventricular septum into the LV cavity, which compromises LV diastolic filling.
Mechanism:
- Right ventricular pressure and volume overload (as seen in pulmonary hypertension and severe RV failure) causes the RV to enlarge.
- The interventricular septum bows towards the LV, reducing the LV end-diastolic volume.
- This results in decreased LV preload and subsequently reduced cardiac output.
Clinical Context:
- Often observed in conditions such as severe pulmonary hypertension, right heart failure, and chronic RV pressure overload.
- It is called reverse because the classic Bernheim effect described LV hypertrophy compressing the RV, whereas this involves the opposite situation with RV enlargement compressing the LV.
. Tumor Microembolism (Pulmonary Tumor Thrombotic Microangiopathy – PTTM)
- Pulmonary Tumor Thrombotic Microangiopathy (PTTM) is a rare but severe complication where tumor microemboli (even if not visible on imaging) obstruct pulmonary arterioles.
- Mechanism:
- Tumor cell emboli trigger fibrocellular intimal proliferation, leading to narrowing and occlusion of small arterioles.
- Release of growth factors (e.g., VEGF, PDGF) induces vascular remodeling and vasospasm.
- Clinical Clues:
- Acute or subacute onset of dyspnea and severe pulmonary hypertension.
- Often occurs in adenocarcinomas, including prostate cancer.
- No overt large pulmonary emboli on CT-PA.
- Diagnosis:
- Consider ventilation-perfusion (V/Q) scan or pulmonary angiography.
- Confirmed histologically on wedge biopsy (if clinically stable).
Hypercalcemia-Induced Vasospasm (Bone Metastases-Related)
- Hypercalcemia from bone metastases can cause vasoconstriction in the pulmonary vasculature.
- Mechanism:
- Elevated calcium levels trigger arteriolar constriction.
- Calcium activates smooth muscle contraction in pulmonary vessels.
- Diagnosis:
- Check serum calcium and PTHrP.