The term “architectural distortion” originates from the Latin word architectura, meaning “construction,” and reflects the disruption of normal lung structure.
AKA
None.
Definition
What is it?
Architectural distortion refers to the abnormal displacement or distortion of normal lung structures, including bronchi, vessels, fissures, or pleura, typically caused by scarring or external pressure.
Caused by:
Fibrosis: Interstitial lung diseases such as usual interstitial pneumonia (UIP) or non-specific interstitial pneumonia (NSIP).
Trauma: Lung contusion, surgery, or radiation therapy.
Infections: Chronic or unresolved infections, such as tuberculosis or fungal infections.
Neoplasms: Tumors causing distortion through mass effect or fibrosis (e.g., post-treatment scarring).
Abnormal alignment or retraction of anatomical landmarks, such as fissures, vessels, or the bronchi.
Functional impairments, including ventilation and perfusion mismatches.
Structural Changes:
Retraction of pleural surfaces.
Displacement of bronchi and vessels.
Thickened interlobular septa and irregular fissures.
Pathophysiology:
The distortion results from a combination of parenchymal injury, repair mechanisms (fibrosis or scarring), and mechanical traction exerted by the surrounding tissue.
Chronic inflammation or fibroproliferative processes can stiffen and contract the lung parenchyma, leading to abnormal positioning of nearby structures.
Pathology:
Dense collagen deposition in the interstitial spaces.
Inflammatory cell infiltration or chronic granulomatous inflammation.
Thickened alveolar septa and remodeled lung tissue.
Diagnosis
Clinical:
Symptoms depend on the underlying cause and severity:
Progressive dyspnea in fibrotic lung diseases.
Chronic cough or chest discomfort.
Radiology:
CXR:
Abnormal displacement of fissures, bronchi, or vessels.
Retraction or deformity of the lung contour.
CT:
Precise evaluation of distorted anatomy with associated findings such as honeycombing, traction bronchiectasis, or fibrotic bands.
Labs:
Supportive tests may include autoimmune markers for fibrotic diseases or microbiological studies for infections.
Treatment
Directed at the underlying cause:
Antifibrotic therapies for UIP or NSIP (e.g., pirfenidone, nintedanib).
Corticosteroids for inflammatory diseases.
Antibiotics or antifungals for infections.
Surgical resection for localized neoplasms.
Radiology in Detail
CXR
Findings:
Displacement or distortion of fissures, bronchi, or vessels.
Volume loss in fibrotic regions.
Associated Findings:
Reticulonodular patterns, opacities, or pleural thickening.
CT
Parts:
Bronchi, blood vessels, interlobular septa, pleura, and fissures.
Size:
Varies with the extent of distortion and underlying pathology.
Shape:
Irregular or retracted lung margins and fissures.
Position:
Abnormal positioning of lung structures, including displacement of hila or retraction toward fibrotic areas.
Character:
Associated with traction bronchiectasis, pleural thickening, or honeycombing.
Time:
Develops progressively in chronic fibrotic conditions.
May stabilize or worsen depending on the disease course or treatment efficacy.
Associated Findings:
Honeycombing in UIP, subpleural sparing in NSIP, or necrotic cavities in infections.
Other Imaging Modalities
MRI/PET CT/NM/US/Angio:
MRI: Limited role but useful for assessing soft tissue and vascular involvement.
PET-CT: Evaluates metabolic activity to differentiate active inflammation or infection from fibrosis.
Ultrasound: May detect pleural involvement or associated effusions.
Key Points and Pearls
Architectural distortion is a hallmark feature of fibrotic lung diseases and chronic structural lung damage.
CT is the gold standard for identifying and characterizing architectural distortion and its associated findings.
The recognition of distortion patterns, combined with clinical and laboratory findings, is essential for diagnosing underlying conditions such as UIP, NSIP, or chronic infections.
Tracking the progression or stabilization of architectural distortion can guide treatment decisions and prognosis.
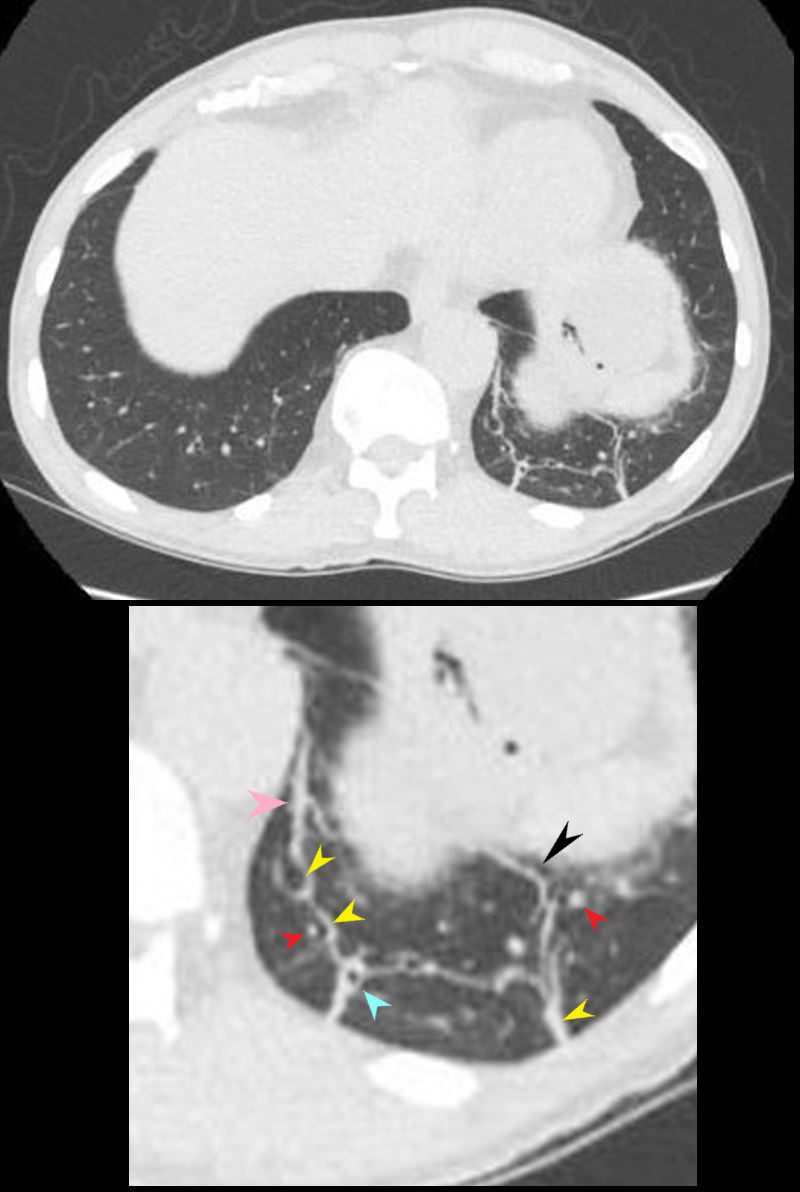
Architectural Distortion CT scan through the lower lung field reveal findings consistent with architectural distortion. The normal arrangement of pulmonary vessels, bronchi, and surrounding structures in the left lower lobe, have a “pulled” or “warped” appearance to the lung parenchyma. In this case scarring associated with bronchial disease with thickening of the bronchial wall, thickening of the interlobular septa, and the presence of and centrilobular nodules, results in linear atelectasis and linear subpleural bands with distortion of the architecture Ashley Davidoff MD TheCommonVein.net 136787-01Architectural Distortion CT scan through the lower lung field reveal findings consistent with architectural distortion. The normal arrangement of pulmonary vessels, bronchi, and surrounding structures in the left lower lobe, have a “pulled” or “warped” appearance to the lung parenchyma (black arrowhead). In this case scarring associated with bronchial disease with thickening of the bronchial wall (teal arrowhead), thickening of the interlobular septa, (yellow arrowheads), and the presence of centrilobular nodules (red arrowheads) results in linear atelectasis and linear subpleural bands (pink arrowhead) with distortion of the architecture Ashley Davidoff MD TheCommonVein.net 136787-01 136787-01LArchitectural Distortion CT scan through the lower lung field reveal findings consistent with architectural distortion. The normal arrangement of pulmonary vessels, bronchi, and surrounding structures in the left lower lobe, have a “pulled” or “warped” appearance to the lung parenchyma. In this case scarring associated with bronchial disease with thickening of the bronchial wall, thickening of the interlobular septa, and the presence of and centrilobular nodules, results in linear atelectasis and linear subpleural bands with distortion of the architecture Ashley Davidoff MD TheCommonVein.net 136787-02
Causes of Architectural Distortion
Architectural distortion can be caused by various conditions, including:
Pulmonary fibrosis or interstitial lung disease, where chronic inflammation or scarring alters lung structure.
Post-infectious scarring, such as after tuberculosis or bacterial pneumonia.
Tumors (primary or metastatic), which can “pull” surrounding structures and alter the lung architecture.
Prior lung surgery or trauma, which can lead to scarring and distortion in the affected areas.
Granulomatous diseases like sarcoidosis, which can produce fibrotic changes.
Radiologic Features
On imaging (X-ray or CT scan), architectural distortion may present with:
Displacement or distortion of bronchi and pulmonary vessels.
Retraction of pleura or fissures towards an area of fibrosis or scarring.
Areas of dense, irregular tissue that lack the typical open and airy appearance of normal lung tissue.
Clinical Significance
Architectural distortion is a non-specific finding but often indicates underlying chronic disease, fibrosis, or malignancy. In cases where architectural distortion is present, additional imaging (e.g., high-resolution CT) or even biopsy may be required to identify the underlying cause, especially if there is no prior history of infection, surgery, or known lung disease.
Architectural distortion is thus an important radiologic sign, prompting further evaluation to rule out serious conditions, including malignancy or advanced interstitial lung disease.
Pathology.—Architectural distortion is characterized by abnormal displacement of bronchi, vessels, fissures, or septa caused by diffuse or localized lung disease, particularly interstitial fibrosis.
CT scans.—Lung anatomy has a distorted appearance and is usually associated with pulmonary fibrosis (,Fig 7) and accompanied by volume loss.
References:
.[1] Raghu G, Remy-Jardin M, Richeldi L, et al. Idiopathic Pulmonary Fibrosis (An Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. American Journal of Respiratory and Critical Care Medicine. 2022;205(9):e18-e47.