
TCV Definition: Lung Cicatricial Atelectasis
Etymology
- Derived from the Latin word cicatrix, meaning “scar,” and the Greek word atelectasis, meaning “incomplete expansion.” The term refers to lung collapse due to scarring or fibrosis.
AKA
- Scarring-related lung atelectasis
Definition
What is it?
- Cicatricial atelectasis refers to a form of lung collapse caused by irreversible contraction and shrinkage of lung tissue due to scarring or fibrosis. This condition often results in chronic volume loss and distortion of lung architecture.
Caused by
- Chronic infections such as tuberculosis or fungal infections (e.g., histoplasmosis, aspergillosis)
- Granulomatous diseases like sarcoidosis
- Radiation-induced lung fibrosis
- Interstitial lung diseases (e.g., idiopathic pulmonary fibrosis)
- Post-surgical or traumatic scarring
Resulting in
- Permanent loss of alveolar air spaces
- Reduced lung compliance
- Decreased lung volume and functional capacity
Structural Changes
- Contraction of fibrotic tissue leading to alveolar collapse
- Distortion of adjacent bronchi and vessels
- Compensatory hyperinflation of surrounding lung regions
Pathophysiology
- Cicatricial atelectasis develops due to progressive fibrosis and scarring, which exert mechanical forces on the surrounding lung tissue, leading to alveolar collapse and architectural distortion. Chronic inflammation plays a key role in promoting fibroblast activation and collagen deposition. Over time, this results in irreversible volume loss and traction on nearby structures, such as bronchi and pulmonary vessels.
Pathology
- Dense collagenous fibrosis replacing normal lung parenchyma
- Architectural distortion, including traction bronchiectasis and vascular remodeling
- Evidence of chronic inflammation and fibrotic nodules in underlying diseases (e.g., granulomas in tuberculosis or sarcoidosis)
Radiology in Detail
CXR
Findings
- Localized or diffuse opacities corresponding to fibrotic scarring
- Volume loss with associated shift of fissures or mediastinal structures
- Crowding of bronchi and vessels in the affected area
Associated Findings
- Retraction of the pleura toward the fibrotic region
- Elevation of the diaphragm on the affected side
- Compensatory hyperinflation of adjacent lung segments
CT
Parts
- Affected lobes or segments of lung tissue
Size
- Varies depending on the extent of fibrosis; localized (segmental or lobar) or diffuse
Shape
- Irregular, nodular, or band-like opacities with associated volume loss
Position
- Frequently involves the upper lobes in diseases like tuberculosis or the lower lobes in idiopathic pulmonary fibrosis
Character
- Traction bronchiectasis
- Irregular reticulations
- Fibrotic bands extending to the pleura
Time
- Chronic and progressive over months to years
Associated Findings
- Calcified lymph nodes in granulomatous diseases
- Honeycombing in advanced interstitial lung disease
Other Imaging Modalities
MRI/PET CT/NM/US/Angio
- MRI: Limited role but may help assess soft tissue involvement
- PET-CT: Useful for identifying active infection, malignancy, or inflammatory activity in chronic fibrotic areas
- Ultrasound: May identify associated pleural effusion or diaphragmatic motion abnormalities
Key Points and Pearls
- Cicatricial atelectasis is irreversible and results from chronic scarring processes that lead to lung collapse and distortion.
- Upper lobe involvement is characteristic of post-tuberculous scarring, while lower lobe predominance suggests interstitial lung disease.
- CT is the imaging modality of choice for detailed assessment, identifying fibrosis, traction bronchiectasis, and architectural distortion.
- Prevention and management involve early treatment of underlying causes (e.g., tuberculosis, granulomatous diseases) and symptomatic care for chronic lung impairment.
Atelectasis and Bronchiectasis
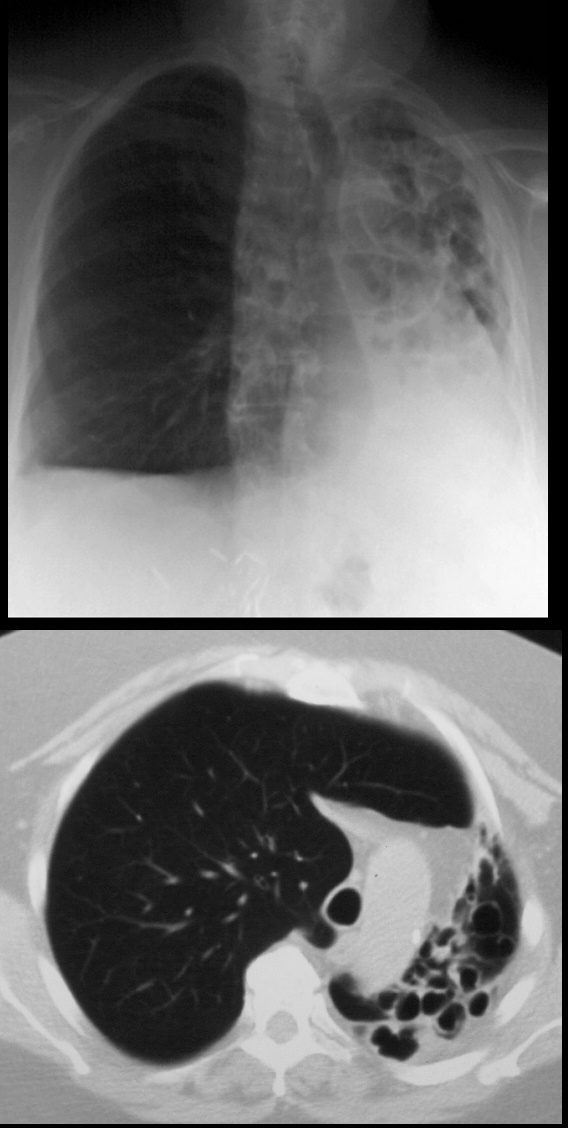
68year old male presents with chronic cough. Chest Xray reveals evidence of tram tracking and bronchiectasis in the left lung with volume loss of the entire right lung with secondary hyperinflation of the right lung, and mediastinal shift. CT scan shows severe volume loss and hyperinflation of the right lung.
Ashley Davidoff MD TheCommonVein.net
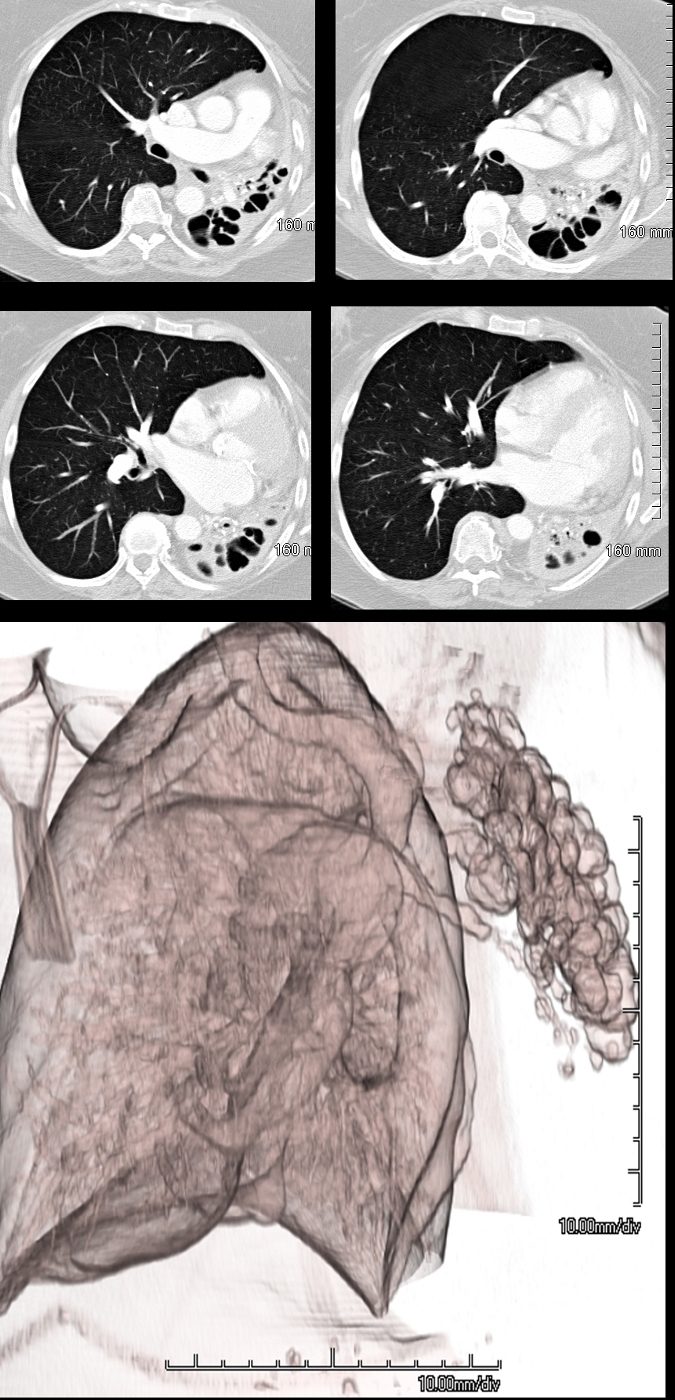
69 year female atrophied left lung secondary to chronic infection and resulting in cystic bronchiectasis (aka saccular bronchiectasis)
The axial images show a totally collapsed left lung with leftward mediastinal shift and hyperinflation of the right lung. The airways of the left lung are large and patent allowing for a 3Dreconstruction of the airways and confirming the diagnosis of saccular bronchiectasis. The atelectasis of the left lung is called cicatricial atelectasis secondary to chronic fibrosis
Ashley Davidoff MD TheCommonvein.net 117955c
Combination of Cicatrization and Obstruction

69year old female with varicose bronchiectasis atelectasis and mucus plugging. The CXR suggests a hilar process with an indistinct margin of the right heart border possibly relating to a middle lobe process. CT scans confirm atelectasis of the middle lobe, varicose bronchiectasis, and the presence of mucoid impaction best revealed in the left lower bronchi
Ashley Davidoff MD TheCommonVein.net
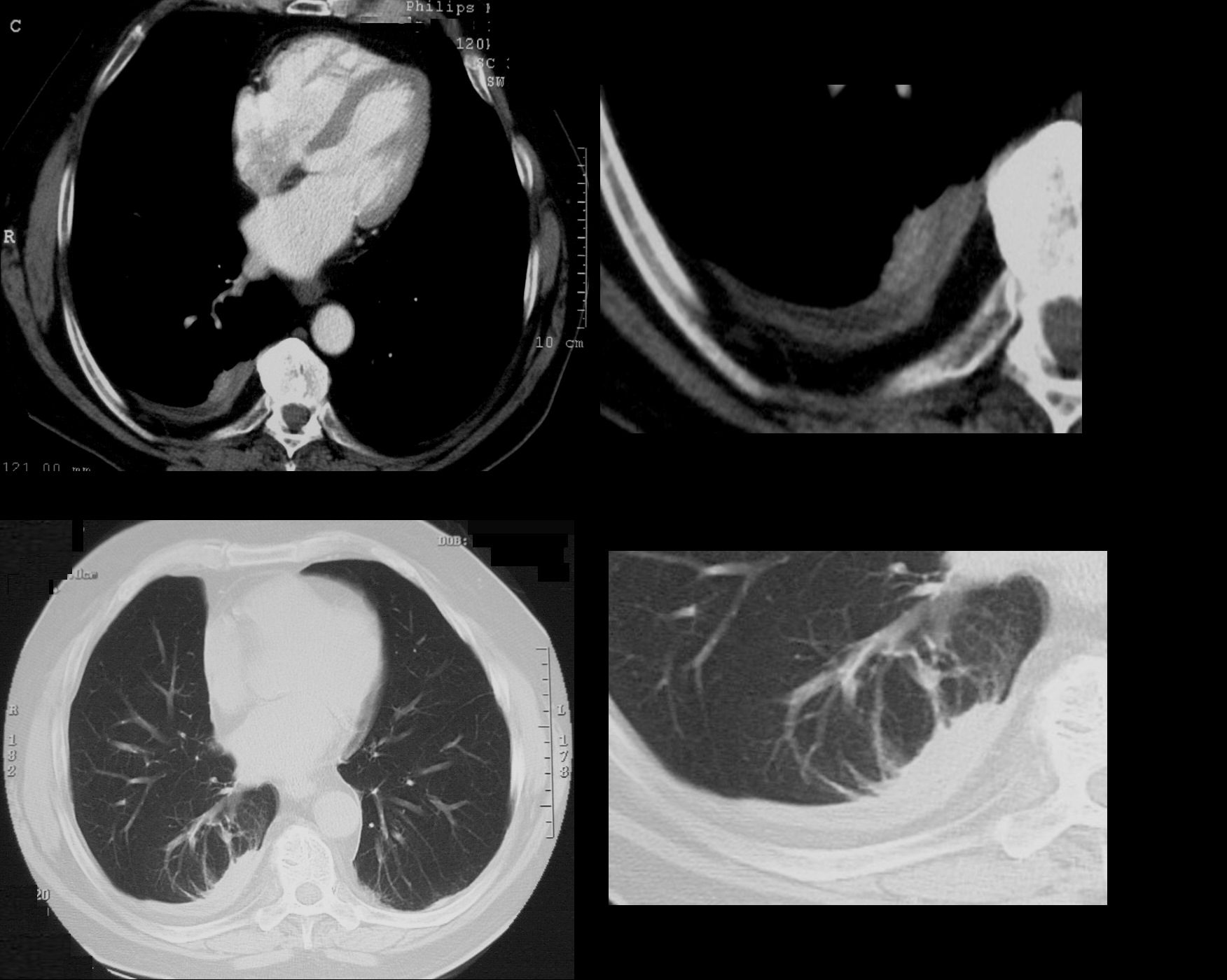
74 year old male with a cough.
CT shows split pleura sign with thickened visceral and parietal pleura with regions of early spiraling of an atelectatic process in the right lower lobe consistent with early rounded atelectasis
Ashley Davidoff MD TheCommonVein.net
31563c