
Bullous emphysema is a type of chronic obstructive pulmonary
disease characterized by the formation of large air-filled spaces,
known as bullae, within the lung tissue. These bullae arise from the
destruction of alveolar walls and coalesce into large spaces that
can occupy significant portions of the lung. The pathogenesis
involves chronic inflammation, often due to smoking or
environmental exposure, leading to the breakdown of elastic lung
tissue. As a result, individuals with bullous emphysema experience
symptoms such as shortness of breath, reduced exercise tolerance,
and an increased risk of pneumothorax (collapsed lung) if a bulla
ruptures. Diagnosis is confirmed through imaging, with chest X-rays
or CT scans showing enlarged air spaces devoid of lung markings (Etesami)
Carcinoid tumors arise from Kulchitsky cells of the bronchial epithelium which are the stem cells having neuroendocrine activity.
60 years of age. A female predominance
attached to the bronchus by a broad base, may have a polypoid appearance.
Necrosis is present, and they tend to be more aggressive.
- single hilar or perihilar mass which is usually well-defined, round or ovoid
- can be of any size but are typically 2-5 cm
- there is often marked homogeneous contrast enhancement due to high vascularity
- calcification (usually eccentric) can occur but is not a common feature
Immunochemistry of atypical carcinoid positive for chromogranin
higher probability to metastasize, to recur, and to have a worse outcome and prognosis.
the 5-year survival ranges from 65% to 75% in
Carcinoid Tumor Causing Post Obstructive Atelectasis
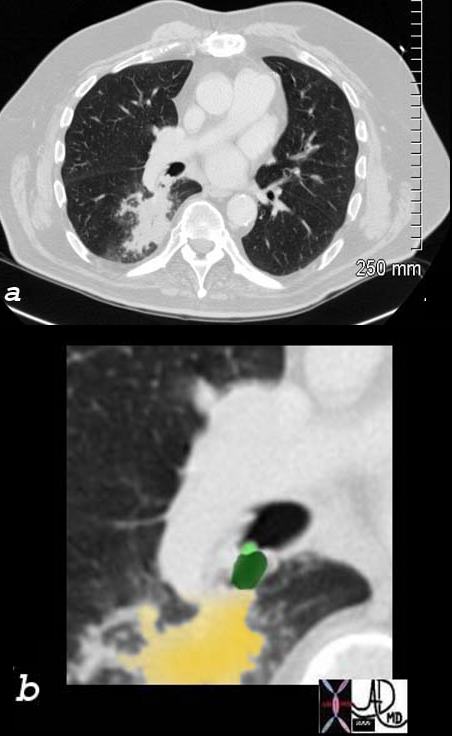
65 year old female presents with a cough. CT shows a mass (green) in proximal portion of the right lower lobe bronchus with post obstructive atelectasis in the superior segment of the right lower lobe (yellow) pathology revealed carcinoid tumor
Ashley Davidoff MD TheCommonVein.net
75679c02
CT Obstructing Nodule in the Left Main Stem Bronchus
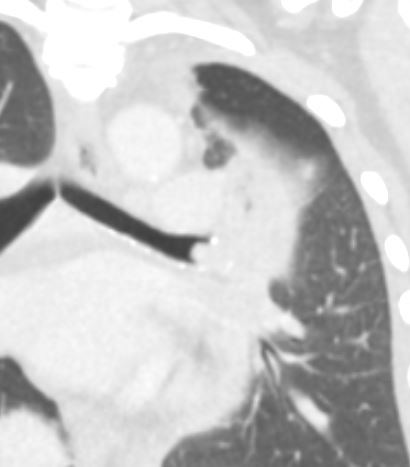
58-year-old female presents with a cough Coronal CT shows a nodule at the branching of the more horizontally oriented left mainstem bronchus with post obstructive atelectasis of the lingula and mild hyperinflation of the upper lobe segments.
Pathology revealed findings consistent with a carcinoid tumor of the left bronchus.
Ashley Davidoff MD TheCommonVein.net 257Lu 136118
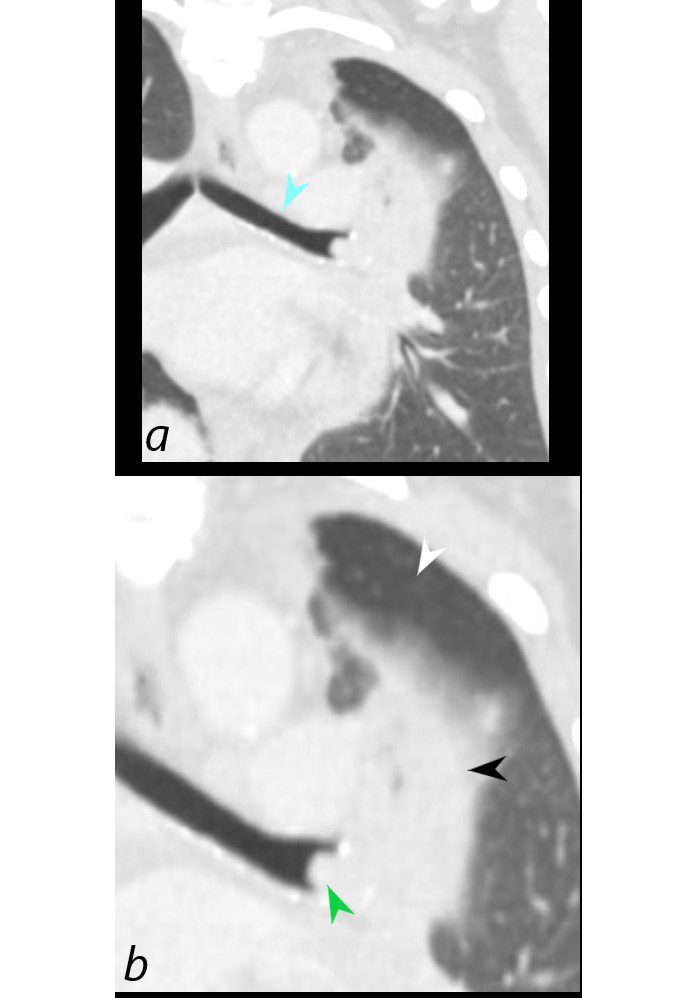
58-year-old female presents with a cough. Coronal CT shows a nodule (green arrowhead, b) at the branching of the more horizontally oriented left mainstem bronchus (teal arrow, a) with post obstructive atelectasis of the lingula (black arrowhead, b) and hyperinflation of the superior aspect of the lower lobe (white arrowhead) which occupies portion of the left apex. (Luftsichel sign)
Pathology revealed findings consistent with a carcinoid tumor
Ashley Davidoff MD TheCommonVein.net 257Lu 136118c

58-year-old female presents with a cough. CT in the axial plane on soft tissue windows shows an obstructing lesion in the left mainstem bronchus of the lung with post obstructive atelectasis of the lingula (black arrowhead) and a small portion of aerated left upper lobe anteriorly (white arrowhead).
Pathology revealed findings consistent with a carcinoid tumor of the left bronchus.
Ashley Davidoff MD TheCommonVein.net 257Lu 136114
Links and References