
Parts
Size
Large Lungs
Increased Retrosternal Space
Small Heart
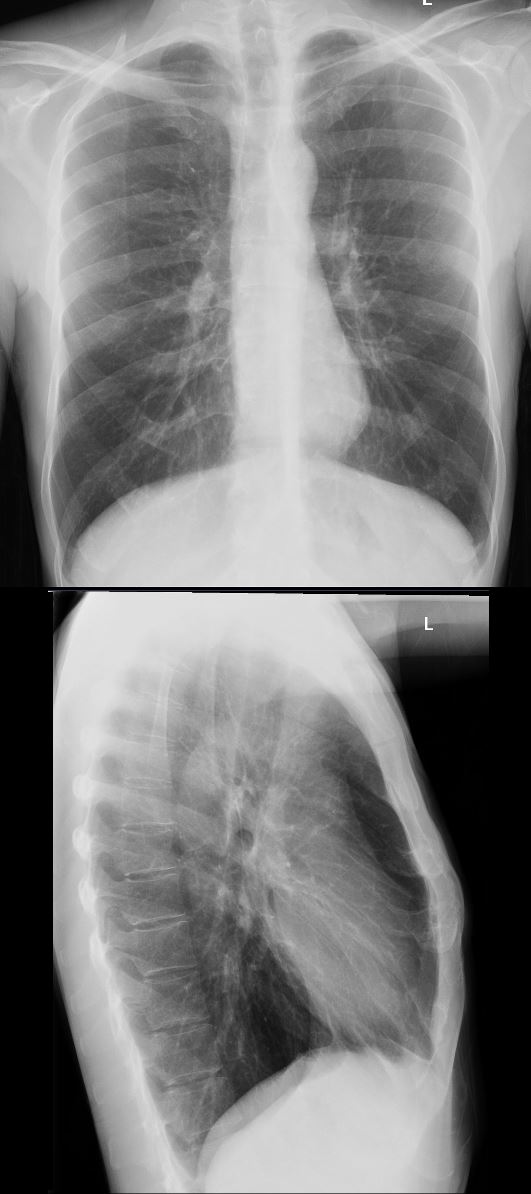
58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart and the lateral chest X-ray shows multiple juxtaphrenic lung markings and juxtaphrenic peaks.
Ashley Davidoff MD TheCommonVein.net 117246c01
Mild
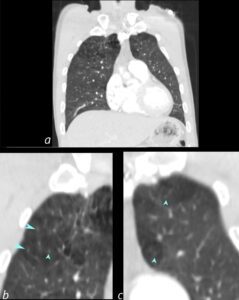
CT shows mild upper lobe centrilobular emphysema
The lower images (b and c) are magnifications and show the classical Swiss cheese appearance of emphysema with a few of the areas revealing centrilobular structures (teal arrowheads).
Ashley Davidoff MD
The CommonVein.net 139241cL 28Lu
Mild to Moderate
CT Emphysema and Small Heart

Ashley Davidoff MD TheCommonVein.net 63M 001

Ashley Davidoff MD TheCommonVein.net 63M 002

Ashley Davidoff MD TheCommonVein.net 63M 003
Shape
Position
Character
Time
Associated Findings
Juxtaphrenic Peaking- Juxtaphrenic Lung Markings
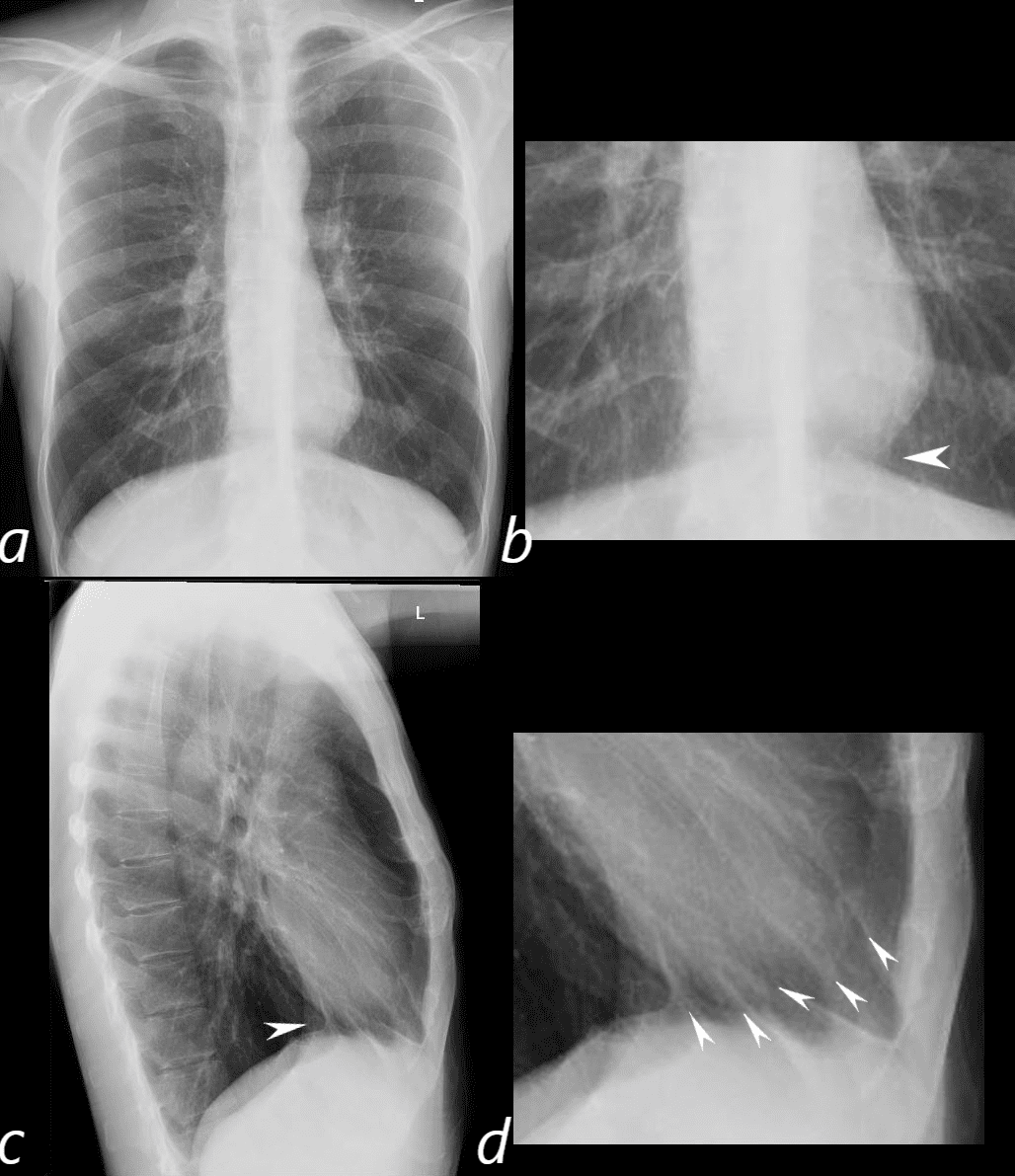
58-year-old male presents with dyspnea. The lungs are hyperinflated with flattening of the diaphragms and increase in the retrosternal space on the lateral examination. The person also has an asthenic build with a relatively straight back and narrow A-P dimension. Frontal CXR shows a small heart with structures of the heart visualized to the right of the midline caused by compression of the low-pressure right atrium. The increased in the retrosternal airspace also compresses the relatively low pressure anteriorly positioned right ventricle. The heart is also lifted off the diaphragm (band c white arrowheads) and results in juxtaphrenic lung markings and peaks below the heart (d, arrowheads)
Ashley Davidoff MD TheCommonVein.net 136232c01L
Infection
Inflammation
Malignancy
Mechanical
Atelectasis
Trauma
Metabolic
Circulatory-
Hemorrhage
Immune Infiltrative Idiopathic Iatrogenic
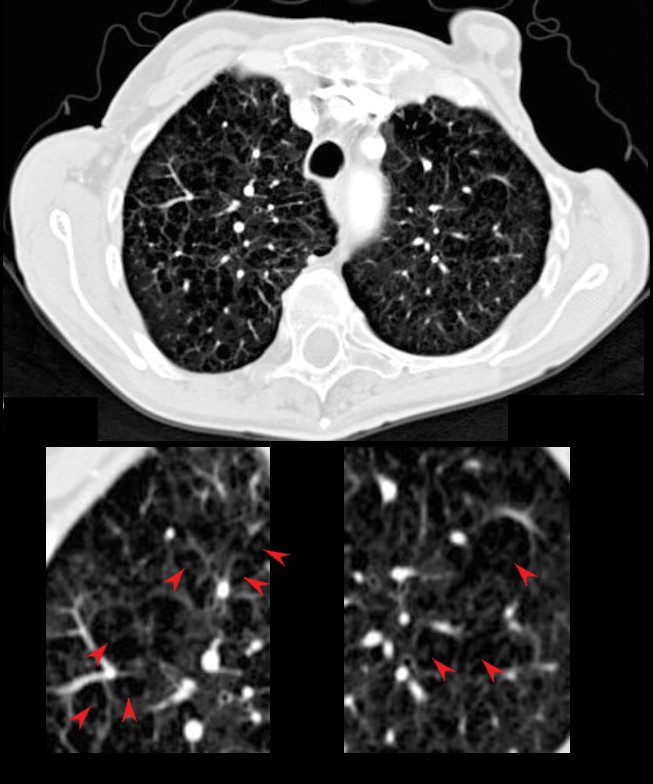
The red arrows point to the soft tissues of the centrilobular emphysema consisting of the arterioles and bronchiolar walls (not usually visible.
71-year-old female presents with history emphysema
Chest X-ray shows hyperinflated lungs with flattened hemidiaphragms and increase in the retrosternal space and right ventricular enlargement based on the decrease in the retrosternal air space
CT scan confirms the presence of centrilobular emphysema, predominantly in the upper lobes with associated right atrial, right ventricular and pulmonary arterial enlargement. The LA and LV are normal
These findings are consistent with cor pulmonale and pulmonary hypertension, secondary to emphysema.
Ashley Davidoff MD

71-year-old female presents with history emphysema
Chest X-ray shows hyperinflated lungs with flattened hemidiaphragms and increase in the retrosternal space and right ventricular enlargement based on the decrease in the retrosternal air space
CT scan confirms the presence of centrilobular emphysema, predominantly in the upper lobes with associated right atrial, right ventricular and pulmonary arterial enlargement. The LA and LV are normal
These findings are consistent with cor pulmonale and pulmonary hypertension, secondary to emphysema.
Ashley Davidoff MD

Ashley Davidoff MD TheCommonvein.net
Emphysema Upper Lung Fields
Enlarged Group of Secondary Lobules
Thickened Irregular Interlobular Septa
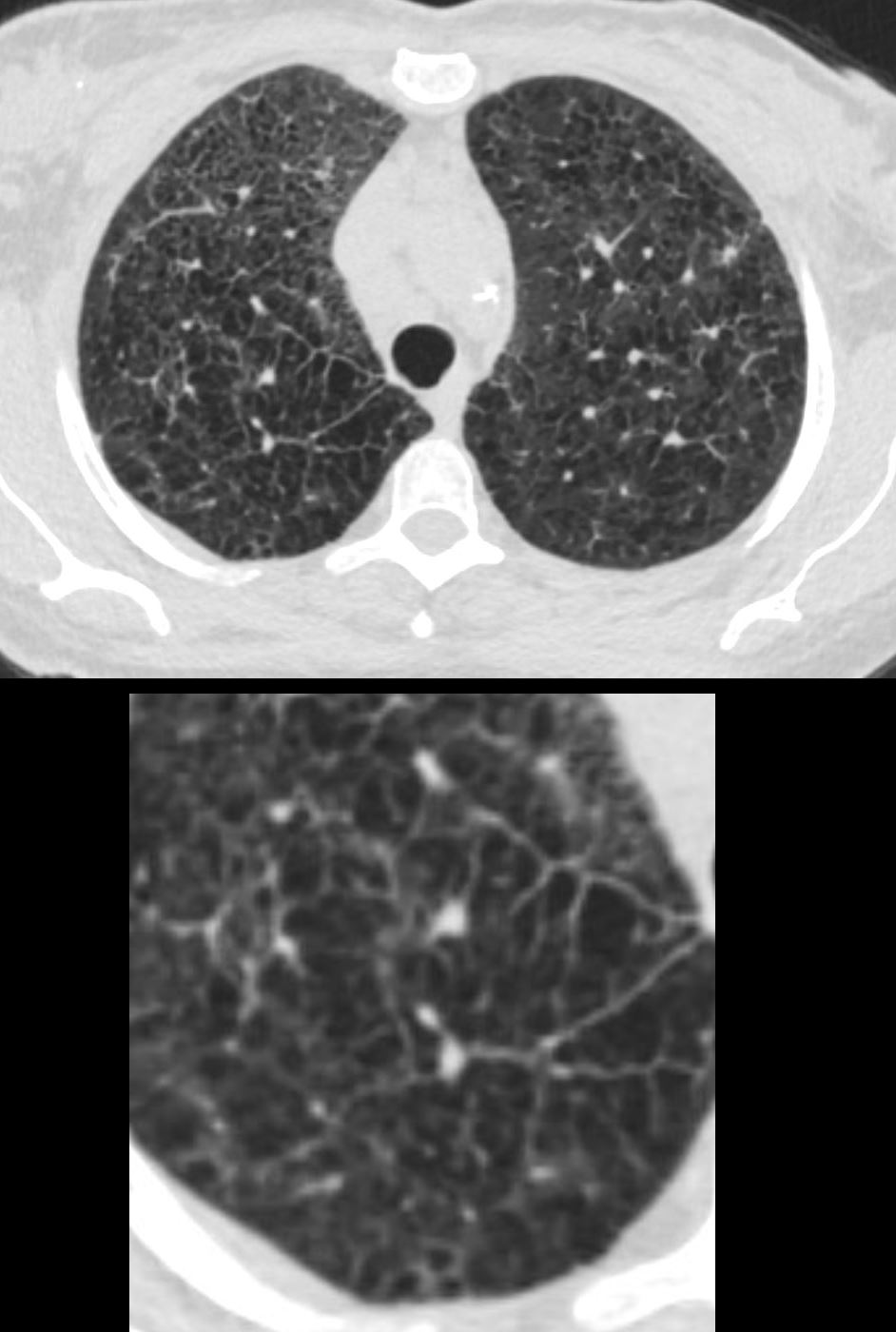
51-year-old female smoker with a history of COPD asthma and pulmonary hypertension presents with progressive dyspnea. Axial CT through the upper lung fields shows extensive changes of centrilobular emphysema and an expanded group of secondary lobules noted in the right upper lobe Path confirmed a diagnosis of DIP
Ashley Davidoff MD TheCommonVein.net 252Lu 135963c
Fissural Changes from Traction
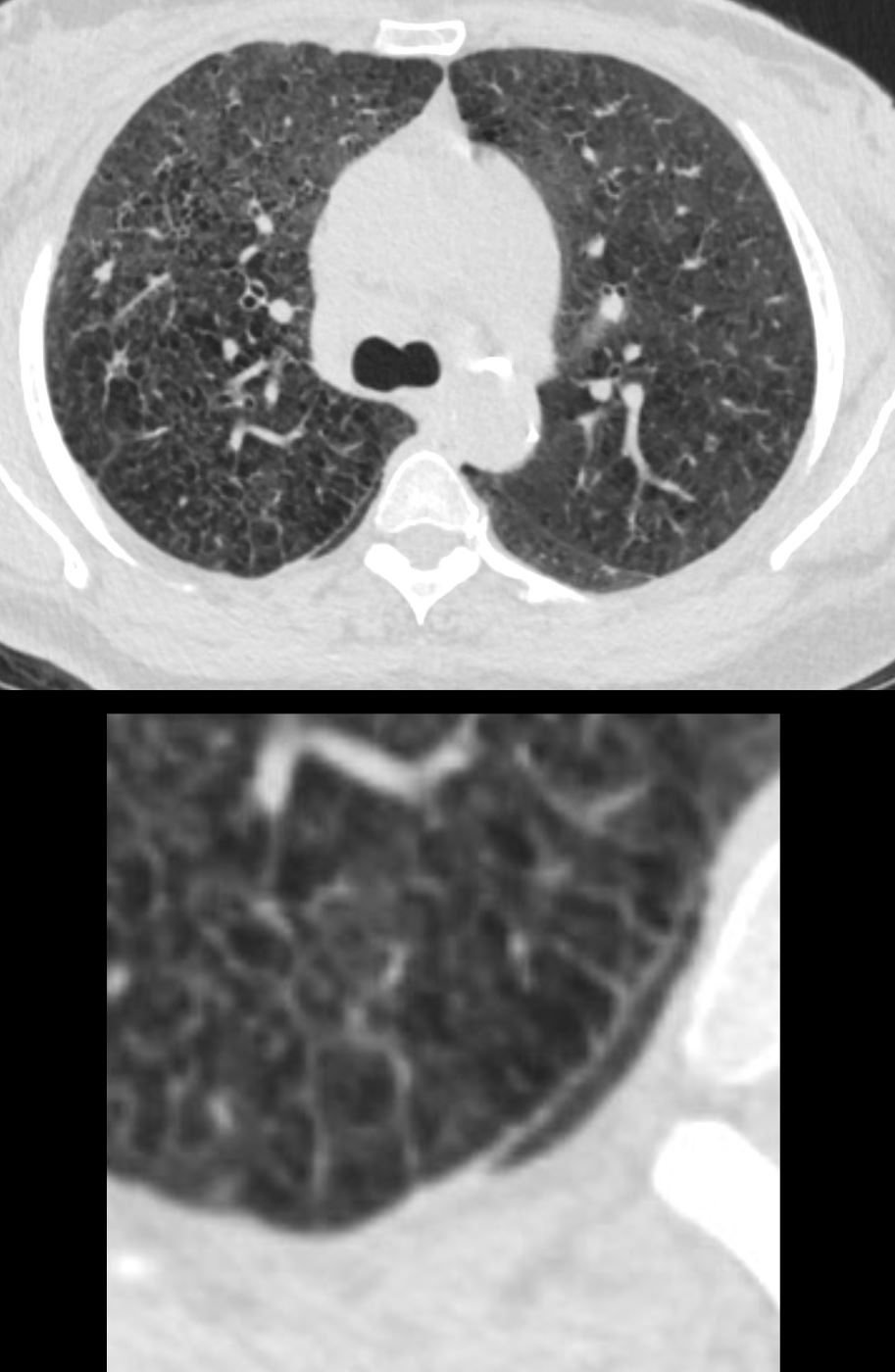
51-year-old female smoker with a history of COPD asthma and pulmonary hypertension presents with progressive dyspnea. Axial CT through the upper lung fields at the level of the carina shows extensive changes of centrilobular emphysema and ground glasses changes in the anterior segments – right more prominent than the left. In addition there is irregularity of the right major fissure (lower panel) seemingly as a result of the enlarged secondary lobule, and stress on the fissure by the interlobular septa. Path confirmed a diagnosis of DIP
Ashley Davidoff MD TheCommonVein.net 252Lu 135965c
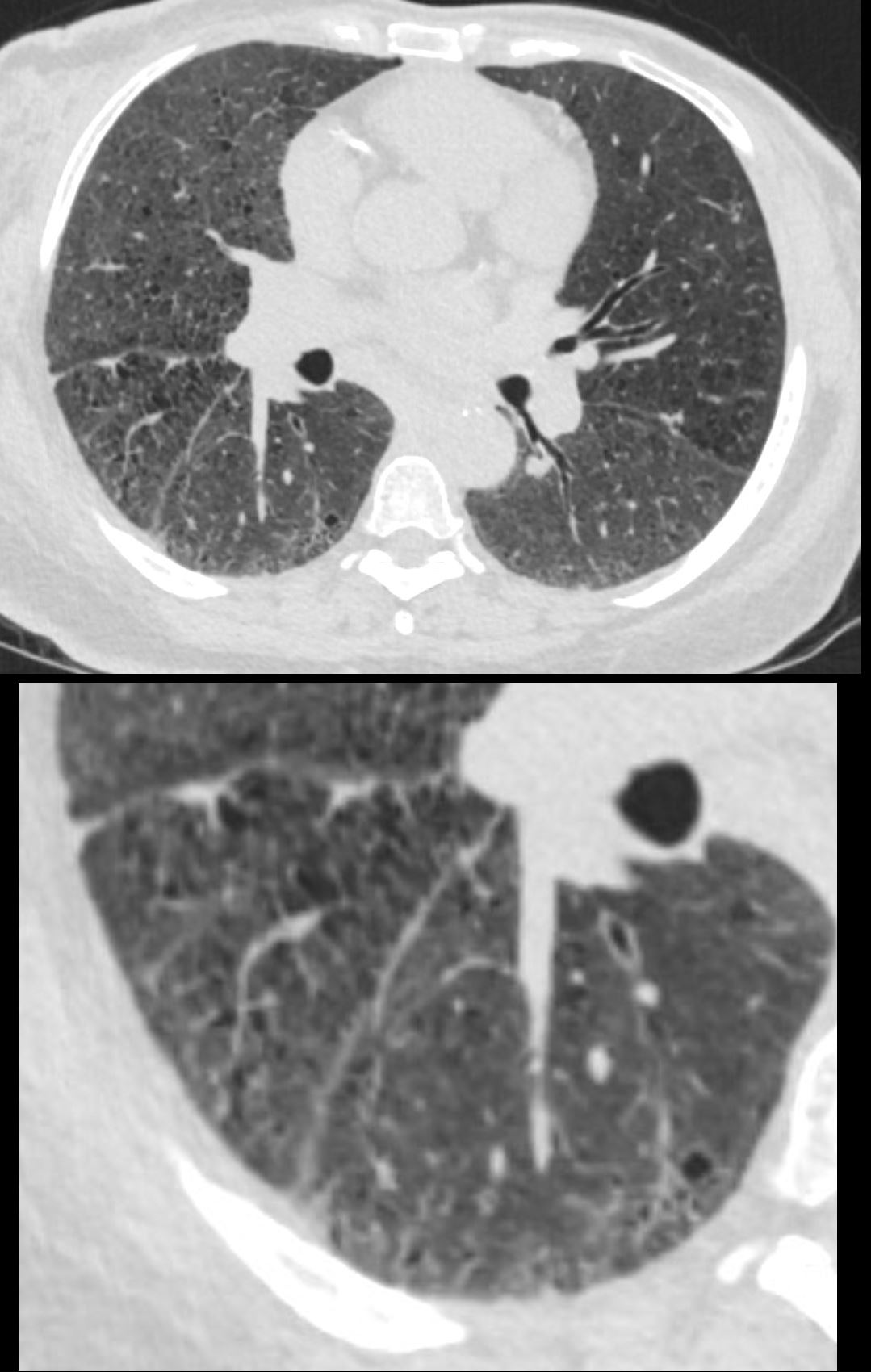
51-year-old female smoker with a history of COPD asthma and pulmonary hypertension presents with progressive dyspnea. Axial CT through the upper lung fields at the level of the carina shows progression from extensive centrilobular changes to ground glass changes in the left anterior segment, and diffuse ground glass changes in the lower lobes. In addition, there is irregularity of the right major fissure (lower panel) seemingly as a result of the enlarged secondary lobule, and stress on the fissure by the interlobular septa. Path confirmed a diagnosis of DIP
Ashley Davidoff MD TheCommonVein.net 252Lu 135966c