
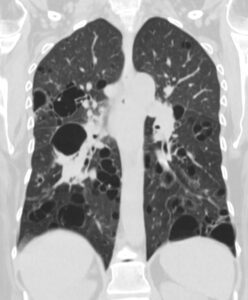
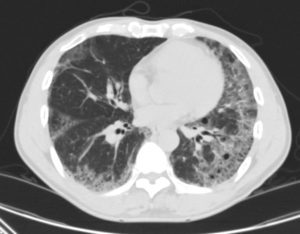
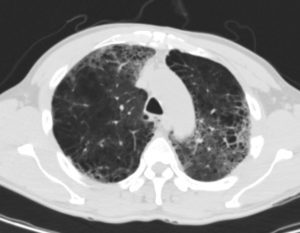
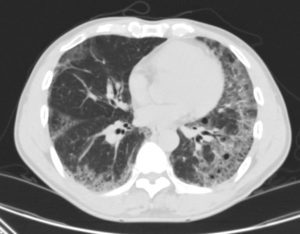
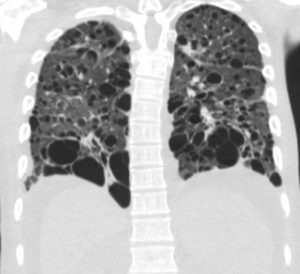
47 F SLE Sjogrens LIP vs Birt-Hogg-Dube basilar thin walled cysts lymphadenopathy
Subsegmental right lower lobe infiltrate
Ashley Davidoff TheCommonVein.net











LIP HIV AIDS and LYMPHOMA
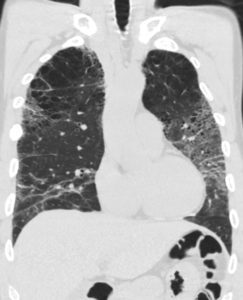
27 year old male with a history of perinatal HIV with intermittent highly active antiretroviral therapy (HAART) compliance with a CD4 count of < 50 with biopsy confirmed B cell lymphoma of the liver, s/p CHOP therapy , chronic esophageal strictures s/p dilatations, esophageal candidiasis, LIP, bronchiectasis pancreatitis, and portal vein and splenic vein thrombosis.
Initial Chest X-ray shows a diffuse reticular pattern with cystic changes dominant at the bases.
CT at that time confirmed the presence of diffuse cystic changes with the largest cysts at the lung bases. Ascites and splenomegaly are also present
He presented one month later with fever and neutropenia.
CT showed an abscess cavity in the right upper lobe in the right upper lobe, thickened distal esophagus with edematous wall, atrophic gastritis and ascites. Bronchovascular thickening along a bronchiectatic segment in the right upper lobe was present in the last CT
Ashley Davidoff MD
LIP HIV AIDS and LYMPHOMA
27 year old male with a history of perinatal HIV with intermittent highly active antiretroviral therapy (HAART) compliance with a CD4 count of < 50 with biopsy confirmed B cell lymphoma of the liver, s/p CHOP therapy , chronic esophageal strictures s/p dilatations, esophageal candidiasis, LIP, bronchiectasis pancreatitis, and portal vein and splenic vein thrombosis.
Initial Chest X-ray shows a diffuse reticular pattern with cystic changes dominant at the bases.
CT at that time confirmed the presence of diffuse cystic changes with the largest cysts at the lung bases. Ascites and splenomegaly are also present
He presented one month later with fever and neutropenia.
CT showed an abscess cavity in the right upper lobe in the right upper lobe, thickened distal esophagus with edematous wall, atrophic gastritis and ascites. Bronchovascular thickening along a bronchiectatic segment in the right upper lobe was present in the last CT
Ashley Davidoff MD
LIP HIV AIDS and LYMPHOMA
27 year old male with a history of perinatal HIV with intermittent highly active antiretroviral therapy (HAART) compliance with a CD4 count of < 50 with biopsy confirmed B cell lymphoma of the liver, s/p CHOP therapy , chronic esophageal strictures s/p dilatations, esophageal candidiasis, LIP, bronchiectasis pancreatitis, and portal vein and splenic vein thrombosis.
Initial Chest X-ray shows a diffuse reticular pattern with cystic changes dominant at the bases.
CT at that time confirmed the presence of diffuse cystic changes with the largest cysts at the lung bases. Ascites and splenomegaly are also present
He presented one month later with fever and neutropenia.
CT showed an abscess cavity in the right upper lobe in the right upper lobe, thickened distal esophagus with edematous wall, atrophic gastritis and ascites. Bronchovascular thickening along a bronchiectatic segment in the right upper lobe was present in the last CT
Ashley Davidoff MD
LIP HIV AIDS and LYMPHOMA
27 year old male with a history of perinatal HIV with intermittent highly active antiretroviral therapy (HAART) compliance with a CD4 count of < 50 with biopsy confirmed B cell lymphoma of the liver, s/p CHOP therapy , chronic esophageal strictures s/p dilatations, esophageal candidiasis, LIP, bronchiectasis pancreatitis, and portal vein and splenic vein thrombosis.
Initial Chest X-ray shows a diffuse reticular pattern with cystic changes dominant at the bases.
CT at that time confirmed the presence of diffuse cystic changes with the largest cysts at the lung bases. Ascites and splenomegaly are also present
He presented one month later with fever and neutropenia.
CT showed an abscess cavity in the right upper lobe in the right upper lobe, thickened distal esophagus with edematous wall, atrophic gastritis and ascites. Bronchovascular thickening along a bronchiectatic segment in the right upper lobe was present in the last CT
Ashley Davidoff MD

LIP HIV AIDS and LYMPHOMA
27 year old male with a history of perinatal HIV with intermittent highly active antiretroviral therapy (HAART) compliance with a CD4 count of < 50 with biopsy confirmed B cell lymphoma of the liver, s/p CHOP therapy , chronic esophageal strictures s/p dilatations, esophageal candidiasis, LIP, bronchiectasis pancreatitis, and portal vein and splenic vein thrombosis.
Initial Chest X-ray shows a diffuse reticular pattern with cystic changes dominant at the bases.
CT at that time confirmed the presence of diffuse cystic changes with the largest cysts at the lung bases. Ascites and splenomegaly are also present
He presented one month later with fever and neutropenia.
CT showed an abscess cavity in the right upper lobe in the right upper lobe, thickened distal esophagus with edematous wall, atrophic gastritis and ascites. Bronchovascular thickening along a bronchiectatic segment in the right upper lobe was present in the last CT
Ashley Davidoff MD
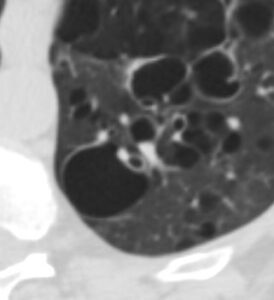
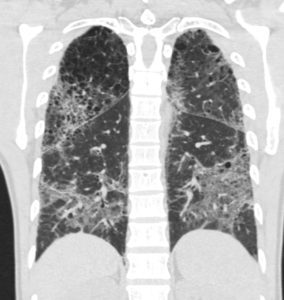
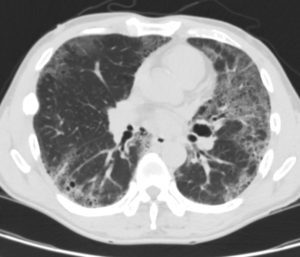
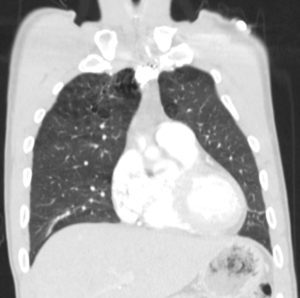
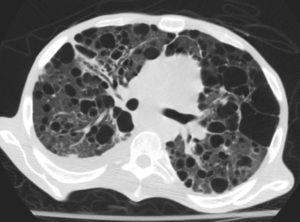
47 F SLE Sjogrens LIP vs Birt-Hogg-Dube basilar thin walled cysts lymphadenopathy
Subsegmental right lower lobe infiltrate
Ashley Davidoff TheCommonVein.net
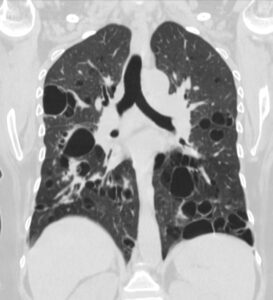
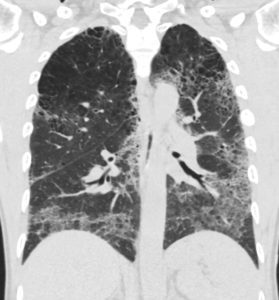
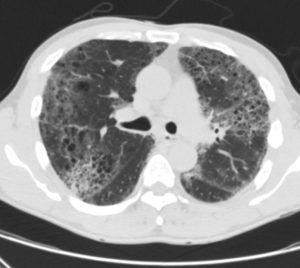
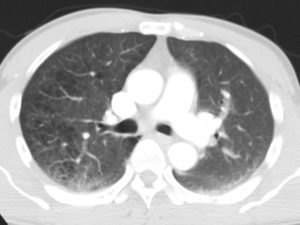
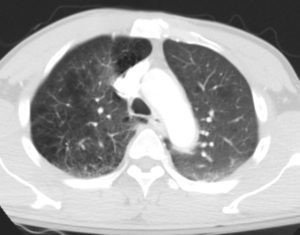
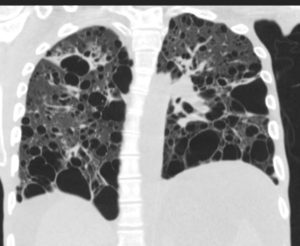
47 F SLE Sjogrens LIP vs Birt-Hogg-Dube basilar thin walled cysts lymphadenopathy
Subsegmental right lower lobe infiltrate
Ashley Davidoff TheCommonVein.net