
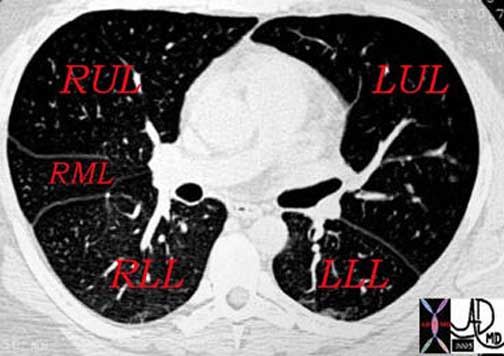
lobes, with the right lung having two fissures (horizontal and
oblique) and the left lung having one (oblique). These fissures, lined
by pleura, allow the lobes to move independently during breathing.
On imaging studies like chest X-rays or CT scans, fissures appear as
thin lines, and changes such as thickening, displacement, or fluid
accumulation can indicate various lung conditions, including
pleural effusion, pneumonia, fibrosis, or atelectasis. (Etesami)

This lateral examination of the chest demonstrates the major fissure in orange, which divides the LUL from the LLL, with LUL being the anterior lobe and the LLL being the posterior lobe.
Courtesy of: Ashley Davidoff, M.D.
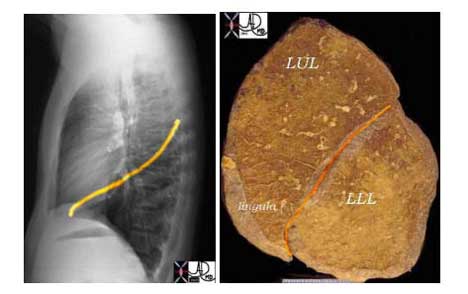
This lateral examination of the chest and corresponding lung specimen in sagital section demonstrates the major fissure in orange, which divides the LUL from the LLL.
Courtesy of: Ashley Davidoff, M.D.

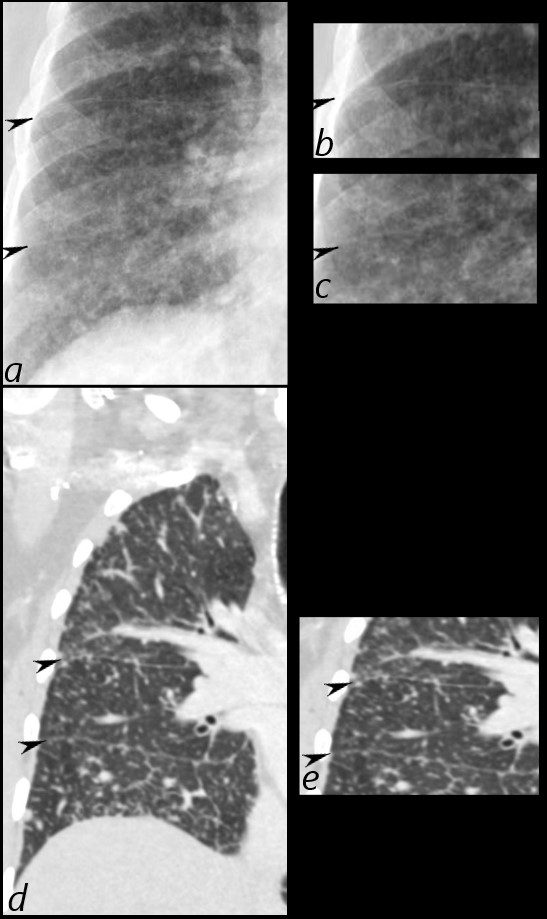
Disease and the Fissures

CXR
Ashley Davidoff MD
thecommonvein.net
CT
Ashley Davidoff MD
thecommonvein.net
CT
Ashley Davidoff MD
thecommonvein.net
CT
Ashley Davidoff MD
thecommonvein.net
Lymphovascular Involvement in Malignancy
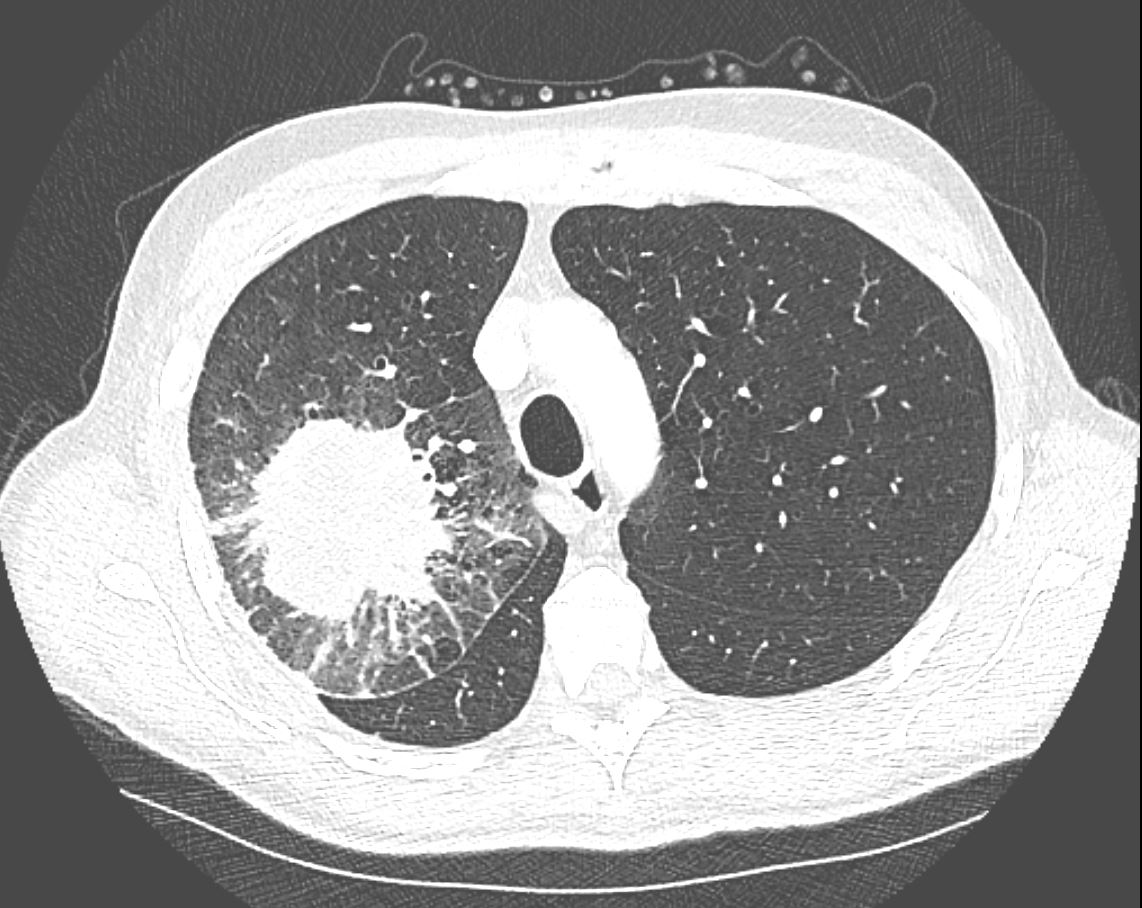
CT in the axial plane demonstrates a large, spiculated mass in the right upper lobe with surrounding halo likely reflecting hemorrhage or lymphatic edema around the mass. In addition, there is evidence of irregular interlobular septal thickening likely reflecting lymphatic invasion and indicating lymphangitis carcinomatosa. There is irregular thickening of the major fissure suggesting involvement.
Ashley Davidoff MD TheCommonVein.net 135865
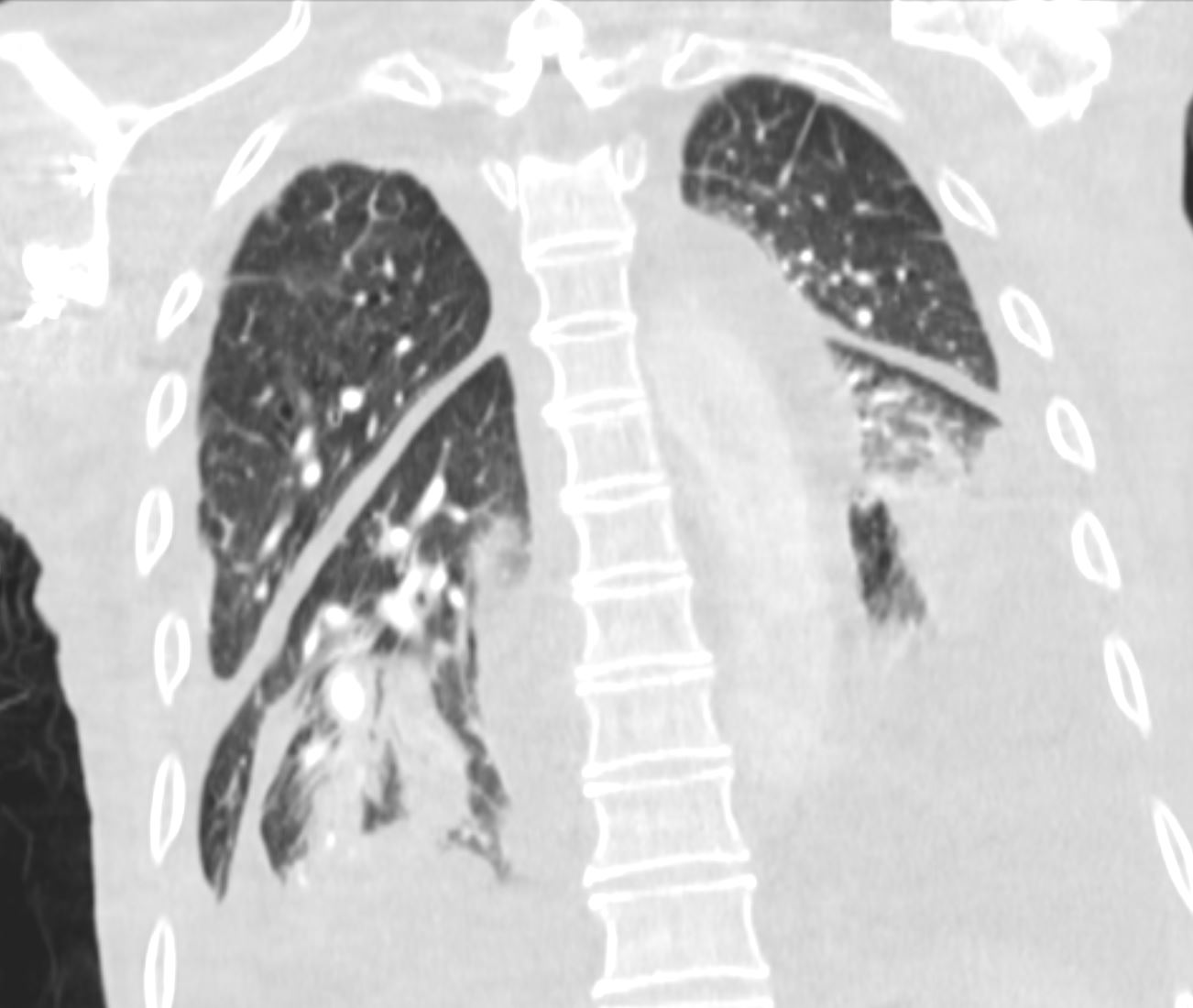
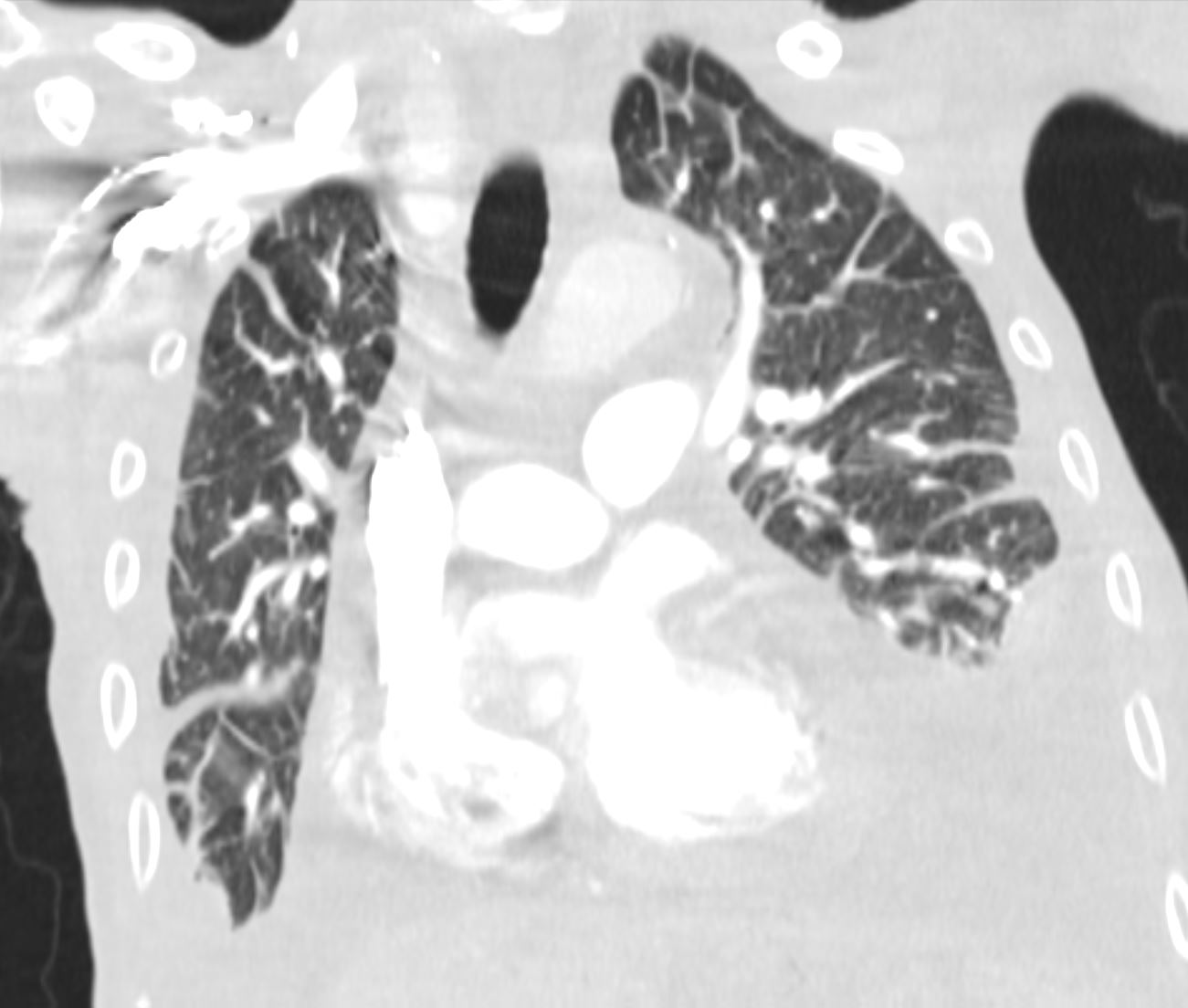
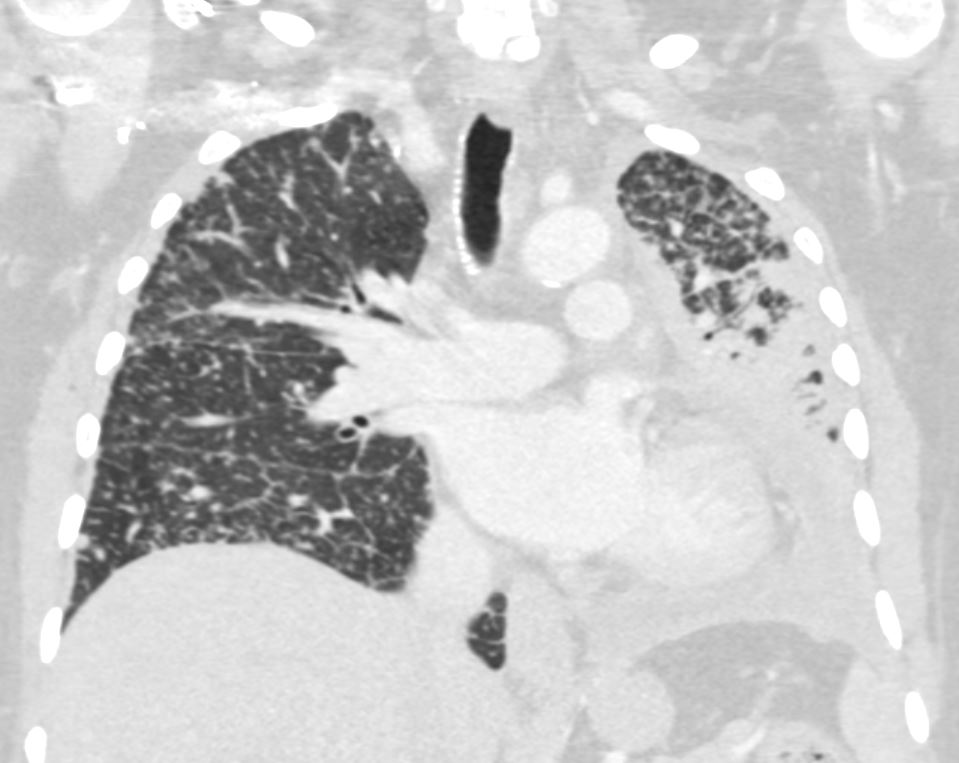
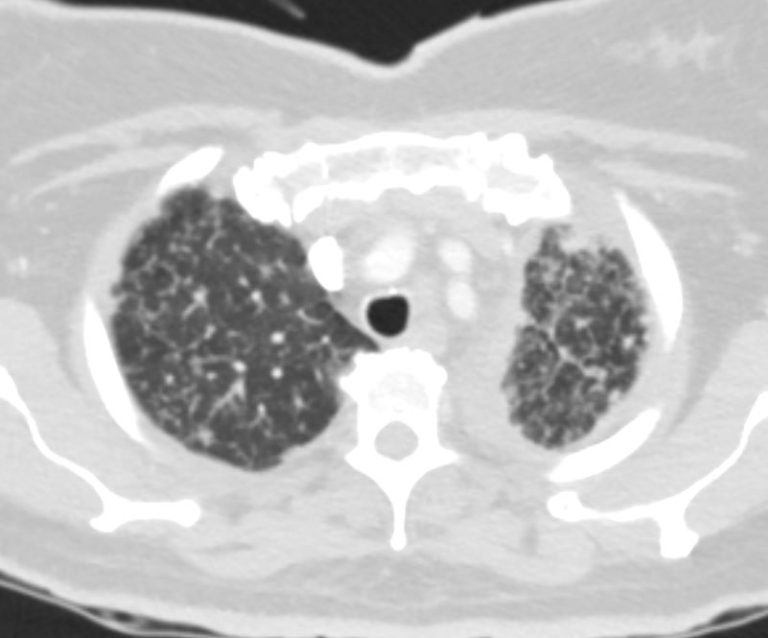
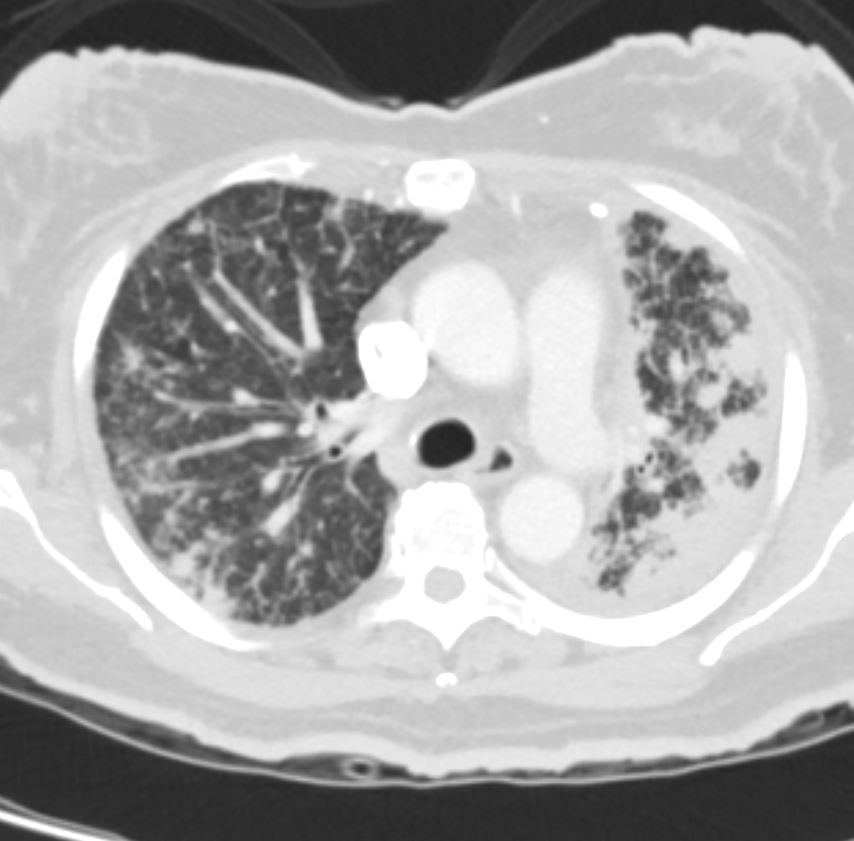
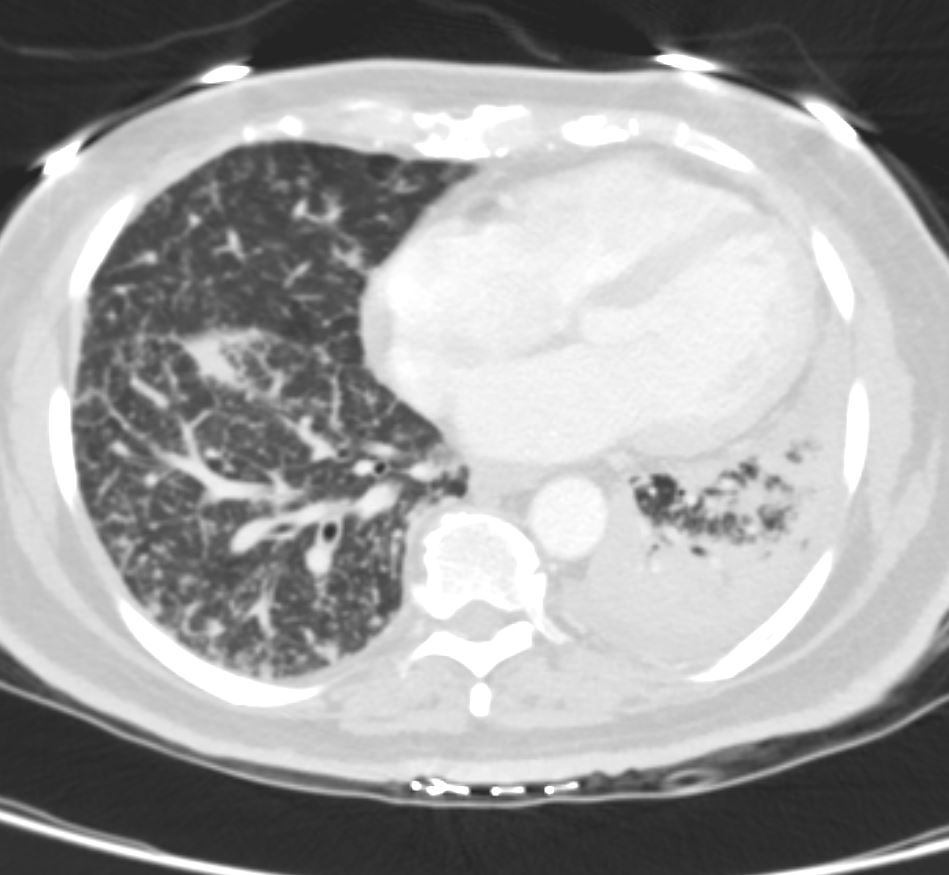
Bilateral Lymphangitis Carcinomatosis in a Patient with Adenocarcinoma

50 year old female with primary adenocarcinoma of the left lung with diffuse bilateral lymphangitic spread of disease characterized by lymphovascular distribution.
The nodularity on the fissures characterize the lymphatic distribution and the nodules are likely of a mixed nature, some being in the interlobular septa, and some in a centrilobular distribution .
Ashley Davidoff MD
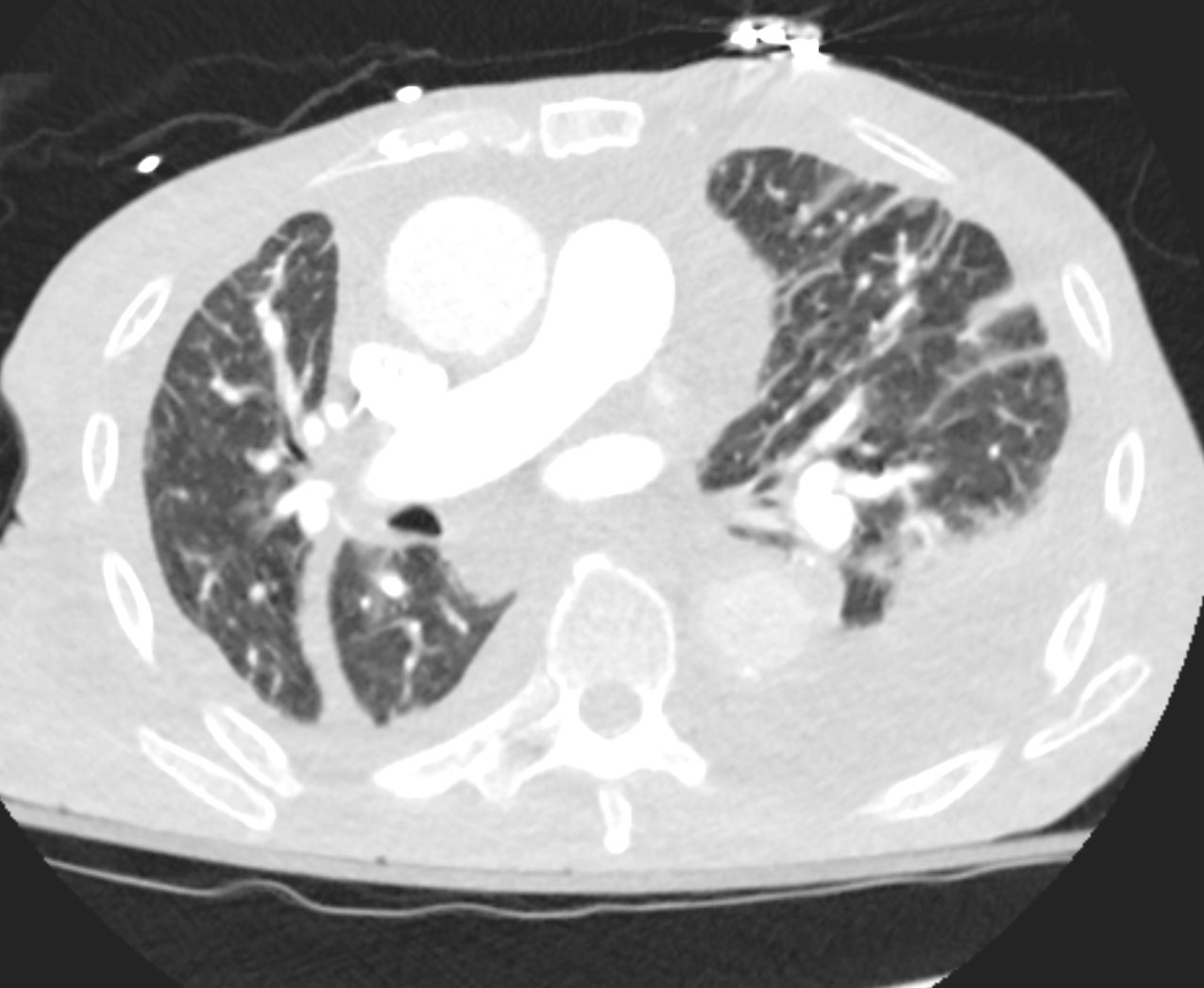
50 year old female with primary adenocarcinoma of the left lung with diffuse bilateral lymphangitic spread of disease characterized by lymphovascular distribution.
The nodularity on the fissures characterize the lymphatic distribution and the nodules are likely of a mixed nature, some being in the interlobular septa, and some in a centrilobular distribution .
Ashley Davidoff MD




Calcification of the Fissures
Calcified nodules on the lung fissures can be caused by a variety of conditions, including previous infections such as tuberculosis, fungal infections, or histoplasmosis. These nodules can also be caused by non-infectious conditions such as sarcoidosis or silicosis, which are conditions that can lead to the formation of granulomas or scar tissue in the lungs.
Lymphoid tissue is present in the lung fissures and is generally considered a normal finding. It can sometimes be associated with underlying conditions such as autoimmune disorders or chronic infections.
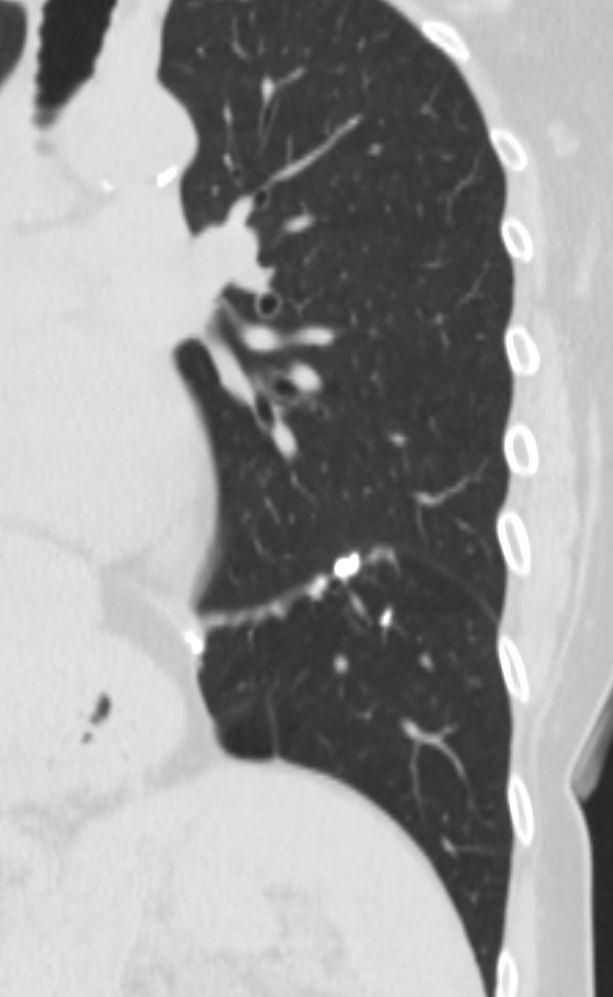
Infection TB
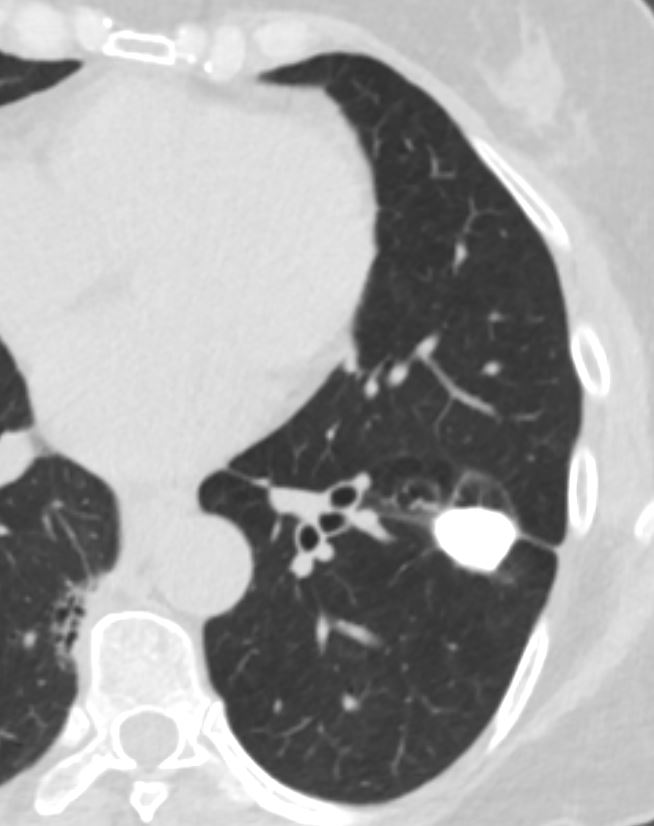
CT scan of TB with Calcified Graulomata Centered around Major fissure and Bronchioles with Atelectasis and Bronchiolectasis
Ashley Davidoff MD The CommonVein.net granulomata-along-fissures-005
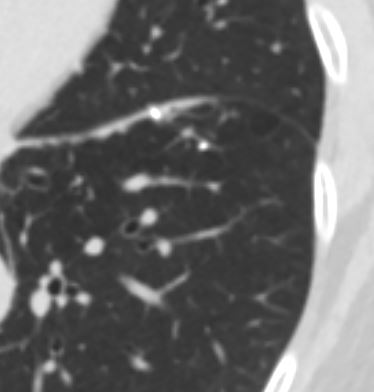
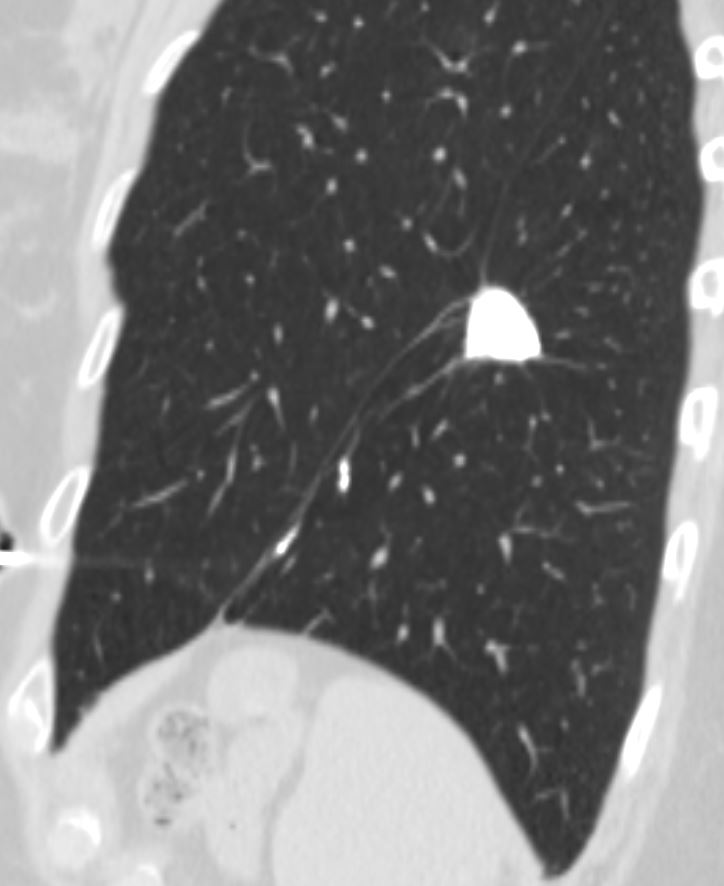
CT scan of TB with Calcified Graulomata Centered around Major fissure and Bronchioles with Atelectasis and Bronchiolectasis
Ashley Davidoff MD The CommonVein.net granulomata-along-fissures-006
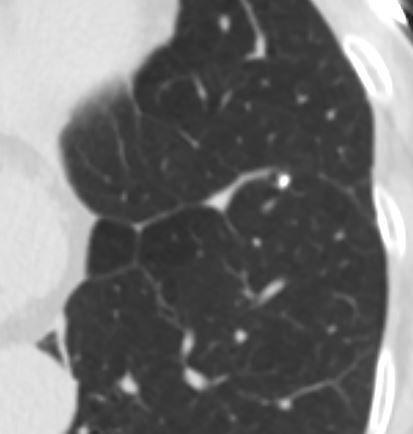
CT scan of TB with Calcified Graulomata Centered around Major fissure and Bronchioles with Atelectasis and Bronchiolectasis
Ashley Davidoff MD The CommonVein.net granulomata-along-fissures-007
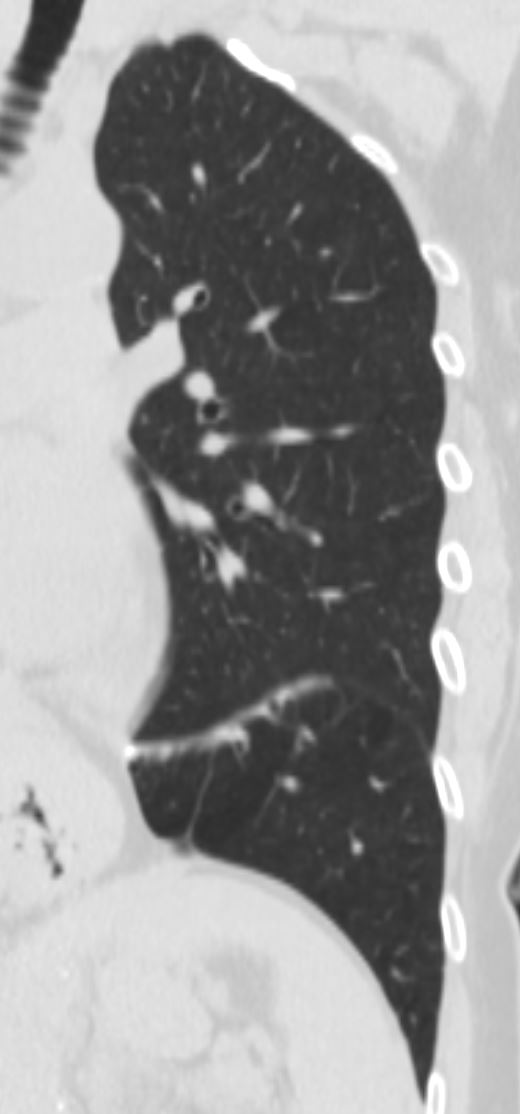
CT scan of TB with Calcified Graulomata Centered around Major fissure and Bronchioles with Atelectasis and Bronchiolectasis
Ashley Davidoff MD The CommonVein.net granulomata-along-fissures-010
CT scan of TB with Calcified Graulomata Centered around Major fissure and Bronchioles with Atelectasis and Bronchiolectasis
Ashley Davidoff MD The CommonVein.net granulomata-along-fissures-010
Ashley Davidoff MD The CommonVein.net granulomata-along-fissures-018