
- What is it:
- The mediastinum is the central compartment of the thoracic cavity, located between the pleural cavities.
- It contains vital structures such as the heart, great vessels, trachea, esophagus, thymus, lymph nodes, and nerves, surrounded by connective tissue.
- Parts:
The mediastinum is divided into three main compartments for clinical and radiological purposes:- Anterior mediastinum: Located between the sternum and pericardium.
- Middle mediastinum: Contains the heart, great vessels, and surrounding structures.
- Posterior mediastinum: Positioned between the pericardium and vertebral column.
-
Anterior Mediastinum
- Size:
- Extends vertically from the thoracic inlet to the diaphragm.
- Width varies but is generally narrow in healthy individuals; enlargement suggests pathology (e.g., masses or effusion).
- Shape:
- Triangular in cross-section, with the base along the diaphragm and apex at the thoracic inlet.
- Position:
- Bounded anteriorly by the sternum.
- Posteriorly by the pericardium and great vessels.
- Lies medial to the pleural spaces.
- Character:
- Contains fat, the thymus gland (in children and young adults), lymph nodes, and small vessels.
- Abnormalities include:
- Masses: Thymomas, teratomas, lymphomas, or ectopic thyroid tissue.
- Density changes: Increased density (on CT) due to fat stranding, calcifications, or soft tissue mass.
Middle Mediastinum
- Size:
- Larger compared to the anterior compartment, spanning the heart and great vessels.
- Width can increase in cases of lymphadenopathy or cardiomegaly.
- Shape:
- Oval or rectangular in shape, depending on the imaging plane.
- Well-defined borders in healthy individuals.
- Position:
- Bounded anteriorly by the pericardium.
- Posteriorly by the posterior pericardium and trachea.
- Centrally located, containing the heart, pericardium, great vessels, trachea, and esophagus.
- Character:
- Contains vascular structures (aorta, pulmonary arteries and veins, superior vena cava), airways (trachea and main bronchi), and lymph nodes.
- Abnormalities include:
- Masses: Bronchogenic cysts, lymphadenopathy, or vascular anomalies.
- Airway changes: Tracheal deviation or compression from adjacent masses.
- Calcifications: Often seen in lymph nodes due to old infections (e.g., tuberculosis).
- Size:
-
- The mediastinum consists of various tissues, including fat, connective tissue, lymph nodes, and organs.
- Each compartment has unique structures and pathologies associated with it.
- Blood supply:
- Mediastinal structures receive blood from branches of the internal thoracic, bronchial, intercostal, and subclavian arteries.
- Venous drainage:
- Mediastinal veins drain into the superior vena cava, azygos vein, hemiazygos vein, and internal thoracic veins.
- Lymphatic drainage:
- Mediastinal lymph nodes are distributed across various stations (e.g., paratracheal, subcarinal).
- These nodes drain into the thoracic duct or the right lymphatic duct.
- Nerve supply:
- Mediastinal structures are innervated by the vagus nerves, sympathetic chains, and phrenic nerves.
- Embryology:
- Mediastinal structures develop from distinct embryological origins:
- Heart and great vessels: Derived from mesoderm.
- Thymus: Derived from the third pharyngeal pouch.
- Trachea and esophagus: Derived from the foregut.
- Mediastinal structures develop from distinct embryological origins:
- Applied anatomy:
- Imaging Application:
- Plain chest radiography: Useful for identifying mediastinal widening or gross masses but lacks compartmental specificity.
- CT (preferred): Provides detailed compartmentalization and characterization of structures and masses.
- MRI: Used for soft tissue characterization and vascular involvement.
- PET-CT: Assesses metabolic activity of mediastinal masses or lymphadenopathy.
- Surgical Application: The mediastinum’s compartments guide thoracic surgeons for resection of masses or lymph node sampling.
- Imaging Application:
Key Points and Pearls
- Anterior mediastinum: Most common site for thymomas, germ cell tumors, and thyroid masses.
- Middle mediastinum: Dominated by lymph nodes, vascular abnormalities, and bronchogenic cysts.
- Posterior mediastinum: Often involved in neurogenic tumors, esophageal disorders, or descending aortic pathology.
- Clear delineation of compartments on imaging helps narrow the differential diagnosis and guide clinical management.
The mediastinum is densely populated with important structures. Often the first signs of disease are recognized on the chest X-ray as a result of subtle changes in the shape of the mediastinum. It is therefore imperative that radiologists are extremely familiar with the normal shape of the mediastinum. Review of the shape may start with the left side at the apex – Think of yourself skiing down a mogul trail and consider the bumpy ride that may challenge you. There is a left sided slope and the right sided slope – both are black diamonds. Get your skis and helmets on– these are tough slopes
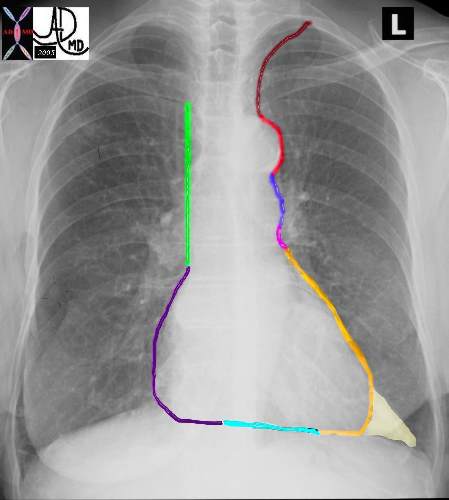
Start with the left slope at the apex of the left lung. After you get off the ski-lift, follow the signs to the “Subclavian Steel” which is painted in dark maroon – just like blood. You will gain speed very quickly off this slope which starts with the subclavian artery. This is the most dangerous of the slopes since you are almost upside down as you start. As you gather speed come across the bump of the aorta. This trail is called the “Aortic Notch” and its sign is colored in bright red. – This trail holds the biggest mogul. A shallow mogul of the MPA (“Lung Artree” dark blue) comes next, and then a concave in pink for the left atrial appendage. “Pretty Pendage” (short lived) After that it is a great mild and long slope of the orange LV (“Smooth Elvee”) until you pass alongside the triangular fat pad of the LV.
The second slope on the right starts near the apex of the right lung and is marked with a bright green sign called “vein cave” As you step off the lift – there is a ninety degree drop, and if you look to your left you will see the red cells in the superior vena cava traveling much slower than you. After the “vein cave” route, the gentle curve around the right atrium (purple) takes over and you are brought to an almost negligible slope of the right ventricle. (teal) The right and left slope meet at the bottom by the ski house.
Ashley Davidoff MD TheCommonVein.net 42260bb01
Applied Anatomy
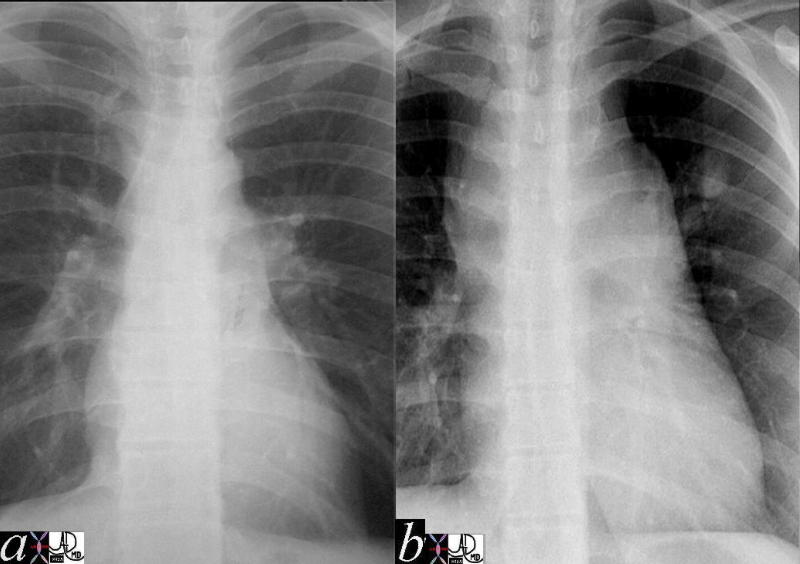
The following image represents one of the many shape changes that occurs in the mediastinum that will tip the radiologist off to a disease process in the chest.
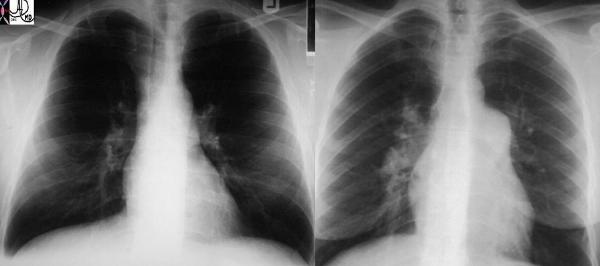
These two P-A chest X-rays show a normal cardio-mediastinal silhouette on the left and an abnormally enlarged MPA and RPA on the right in this patient with pulmonary hypertension. Which mogul has become more prominent? Is it “Subclavian Steel”, “Aortic Notch”, “Lung ArTree”, “Pretty Pendage”, or “Smooth Elvey”? The criminal I am afraid who has enlarged before our eyes is “Lung Artree” and he signifies tension in the house – pulmonary hypertension.
Ashley Davidoff MD TheCommonVein.net 22089c
Enlarged Mediastinum Caused by Adenopathy
Ashley Davidoff MD TheCommonVein.net
42056c01
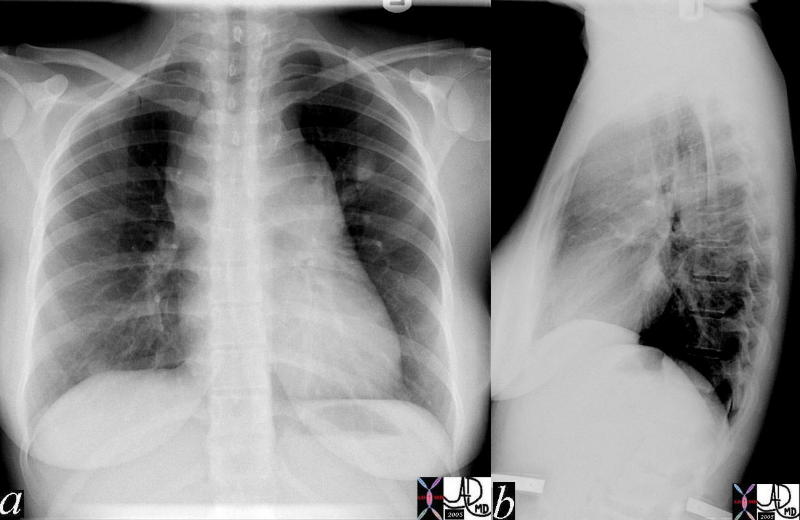
Normal vs Abnormal
The first image represents the normal and the second a mediastinal silhouette that is very abnormal. There are multiple “mogul” enlargements, including the region of the aortic knob, the pulmonary segment and the SVC. The following CT explains the appearance below. Note the nodule in the left upper lobe
Ashley Davidoff MD TheCommonVein.net 2056c02
CT of the Above Patient
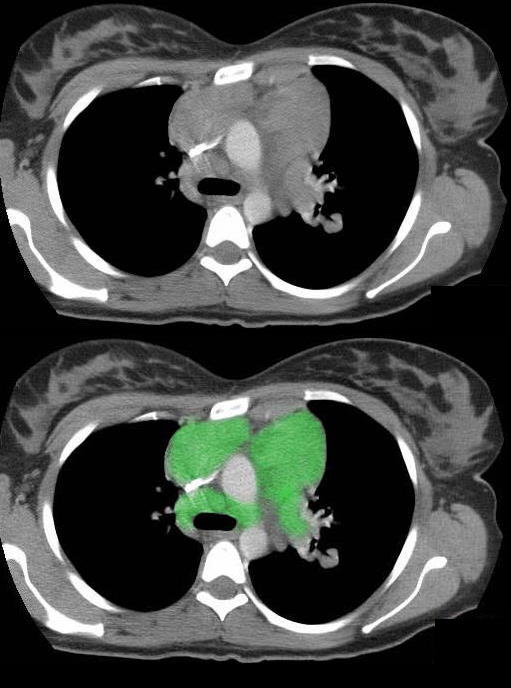
This transverse section through the top of the aortic arch shows multiple enlarged soft tissue masses in the superior mediastinum representing enlarged lymph nodes in this patient with lymphoma.
The enlarged lymph nodes are outlined in green compressing on the superior vena cava (SVC).
Ashley Davidoff MD TheCommonVein.net 42062c01
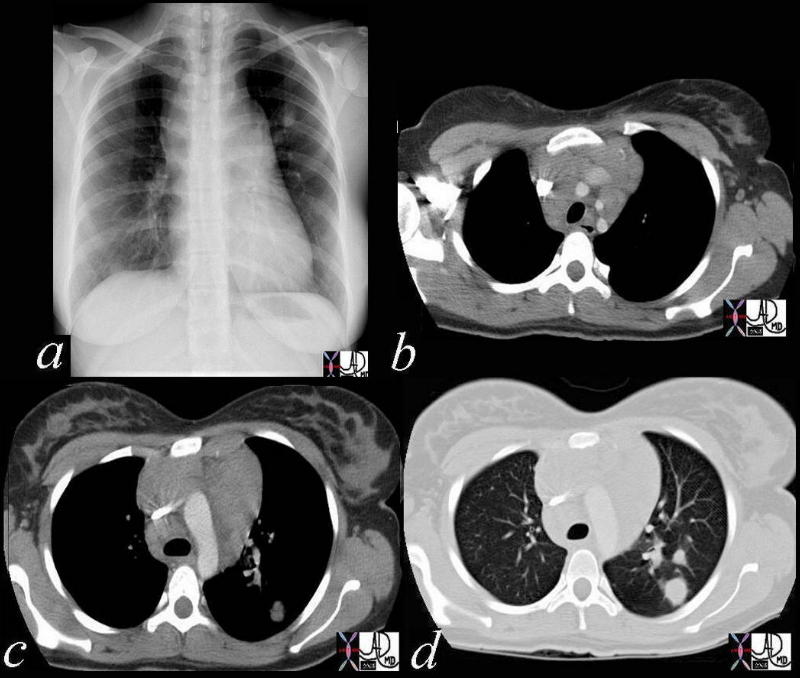
This series of images tells the whole story of the chest with the presenting radiograph (a) the extensive mediastinal adenopathy (b,c) and the lung nodule (d). Within the posterior segment of the left upper lobe there a 2.5 cms nodule with mild reticulations likely a lymphomatous deposit
42068c03
Ashley Davidoff MD TheCommonVein.net