
- AKA:
- NSIP, Uniform Interstitial Pneumonia.
- Etymology:
- The term non-specific reflects the lack of unique histological features compared to other interstitial lung diseases (e.g., UIP).
- What is it:
- NSIP is a chronic inflammatory disease and a subtype of interstitial lung disease (ILD).
- Characterized by:
- Diffuse or patchy interstitial inflammation and/or fibrosis with:
- Lower lobe predominance,
- Bronchovascular distribution,
- Ground-glass opacity,
- Subpleural sparing, and
- Absence of honeycombing.
- Occurs in two forms:
- Cellular NSIP: Predominantly inflammatory changes with minimal fibrosis.
- Fibrotic NSIP: More pronounced fibrosis with associated structural remodeling.
- Diffuse or patchy interstitial inflammation and/or fibrosis with:
- Anatomically affecting:
- Bronchovascular bundles (peribronchial and perivascular interstitium).
- Interstitial spaces (including alveolar septa and interlobular regions).
- Alveolar ducts (connecting airways to alveoli).
- Alveoli (air sacs responsible for gas exchange).
- What causes it:
- Idiopathic NSIP:
- Cause unknown; classified as an idiopathic interstitial pneumonia.
- Secondary NSIP:
- Often associated with systemic autoimmune diseases, such as:
- Systemic sclerosis,
- Sjögren’s syndrome, and
- Polymyositis/dermatomyositis.
- Other potential causes include:
- Drug-induced lung injury (e.g., chemotherapy, immunotherapy),
- Environmental exposures (e.g., dusts or fumes), and
- Chronic viral infections (e.g., HIV).
- Often associated with systemic autoimmune diseases, such as:
- Idiopathic NSIP:
- What is the result:
- Persistent inflammation and fibrosis result in:
- Impaired gas exchange,
- Restriction of lung expansion,
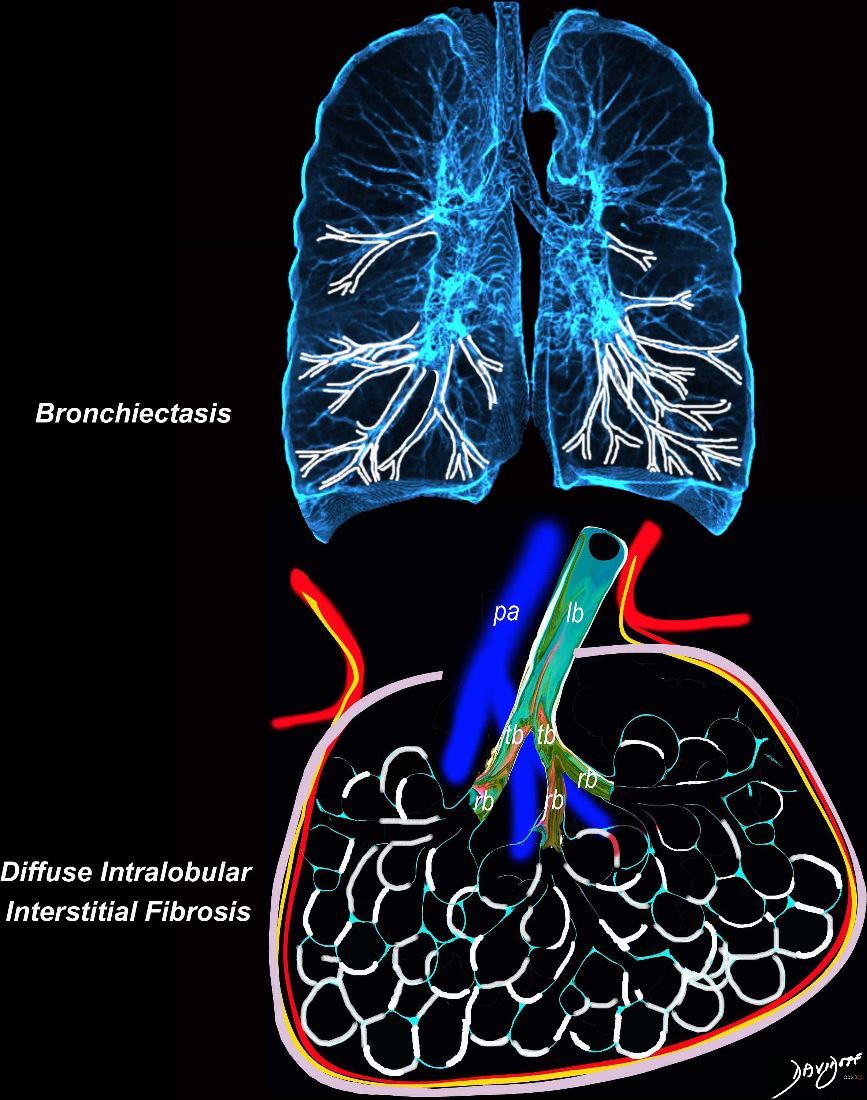
- Development of traction bronchiectasis and bronchiolectasis in advanced cases.
- Persistent inflammation and fibrosis result in:
- How is it diagnosed:
- a) Clinical findings:
- Symptoms include:
- Gradual onset of progressive dyspnea,
- Chronic dry cough, and
- Fatigue, often over months to years.
- Symptoms include:
- b) Imaging studies:
- Chest X-ray:
- Diffuse reticular opacities, often bilateral and symmetrical.
- Chest CT:
- Parts: Diffuse or patchy ground-glass opacities, reticulations, and peribronchovascular thickening.
- Size: Variable, from focal regions to diffuse lung involvement.
- Shape: Homogeneous or reticular.
- Position:
- Lower lobe predominance and bronchovascular distribution.
- Subpleural sparing, a key distinguishing feature of NSIP.
- Character:
- Minimal or absent honeycombing (distinguishing it from UIP).
- Traction bronchiectasis and bronchiolectasis in advanced fibrotic cases.
- Time:
- Slowly progressive but may stabilize or improve with treatment.
- Chest X-ray:
- c) Laboratory findings:
- Autoimmune markers: ANA, anti-Ro/SSA, anti-La/SSB for associated systemic diseases.
- Exclude infections with serologies for chronic viral infections (e.g., HIV, hepatitis).
- a) Clinical findings:
- How is it treated:
- First-line therapy:
- Corticosteroids (e.g., prednisone): Typically effective in reducing inflammation.
- Second-line options:
- Immunosuppressive agents (e.g., mycophenolate mofetil, azathioprine) for refractory or progressive disease.
- Supportive care:
- Oxygen therapy and pulmonary rehabilitation for advanced disease.
- Monitoring:
- Serial imaging and pulmonary function tests to assess response to treatment and detect progression.
- First-line therapy:
- Radiological implications:
- NSIP findings include symmetrical ground-glass opacities, fine reticulations, and subpleural sparing.
- Lower lobe predominance and bronchovascular distribution are hallmark features.
- Honeycombing is rare, further distinguishing NSIP from UIP.
- Traction bronchiectasis and bronchiolectasis reflect advanced fibrotic changes and chronicity.
- Key points and pearls:
- NSIP is often associated with systemic autoimmune diseases, particularly systemic sclerosis.
- Lower lobe predominance and subpleural sparing are highly characteristic.
- The prognosis is better than UIP, as many patients stabilize or improve with corticosteroids or immunosuppressive therapy.
- Histopathology and imaging are critical for distinguishing NSIP from other ILDs.
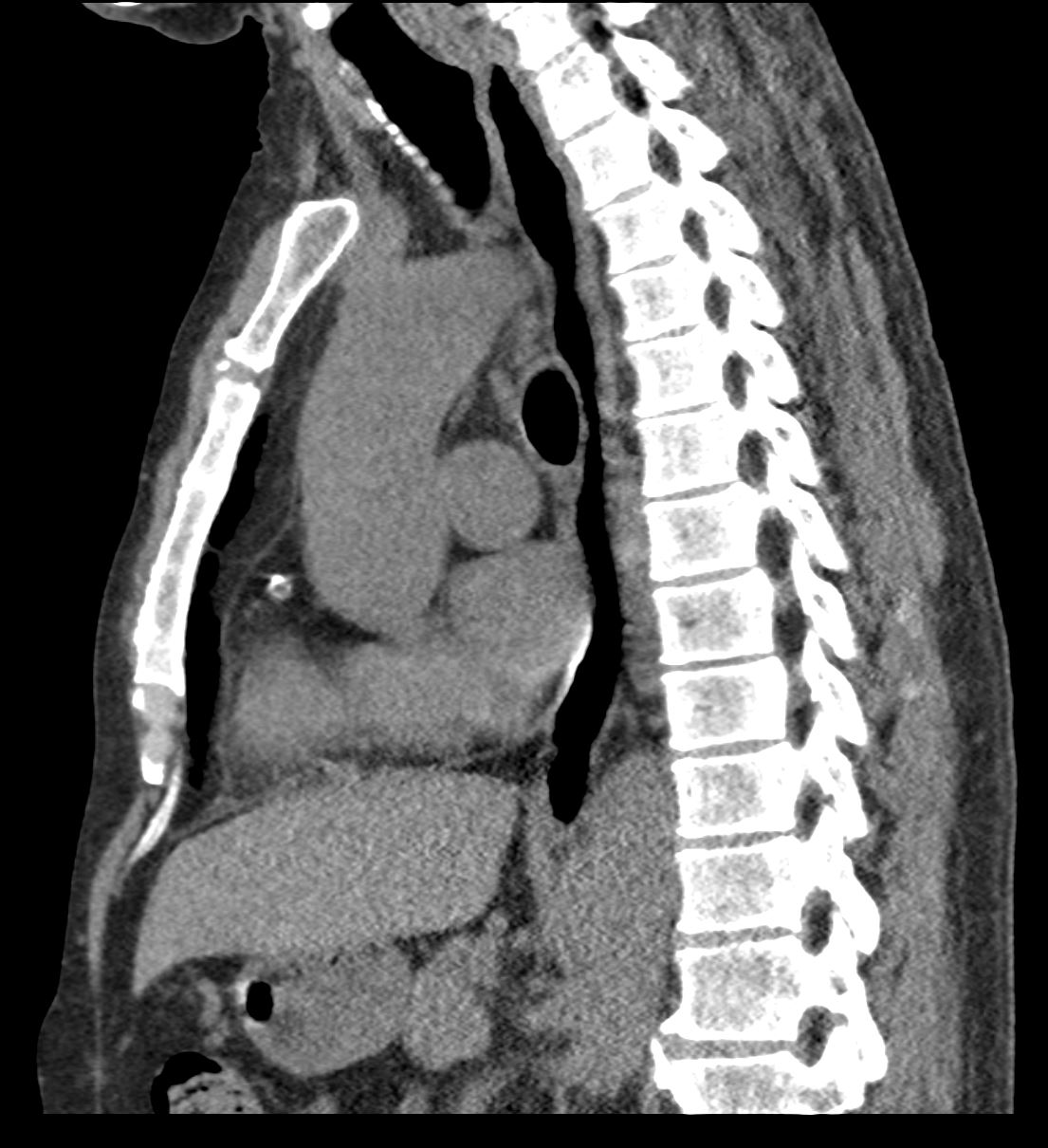
In a Nutshell Buzz (NB)
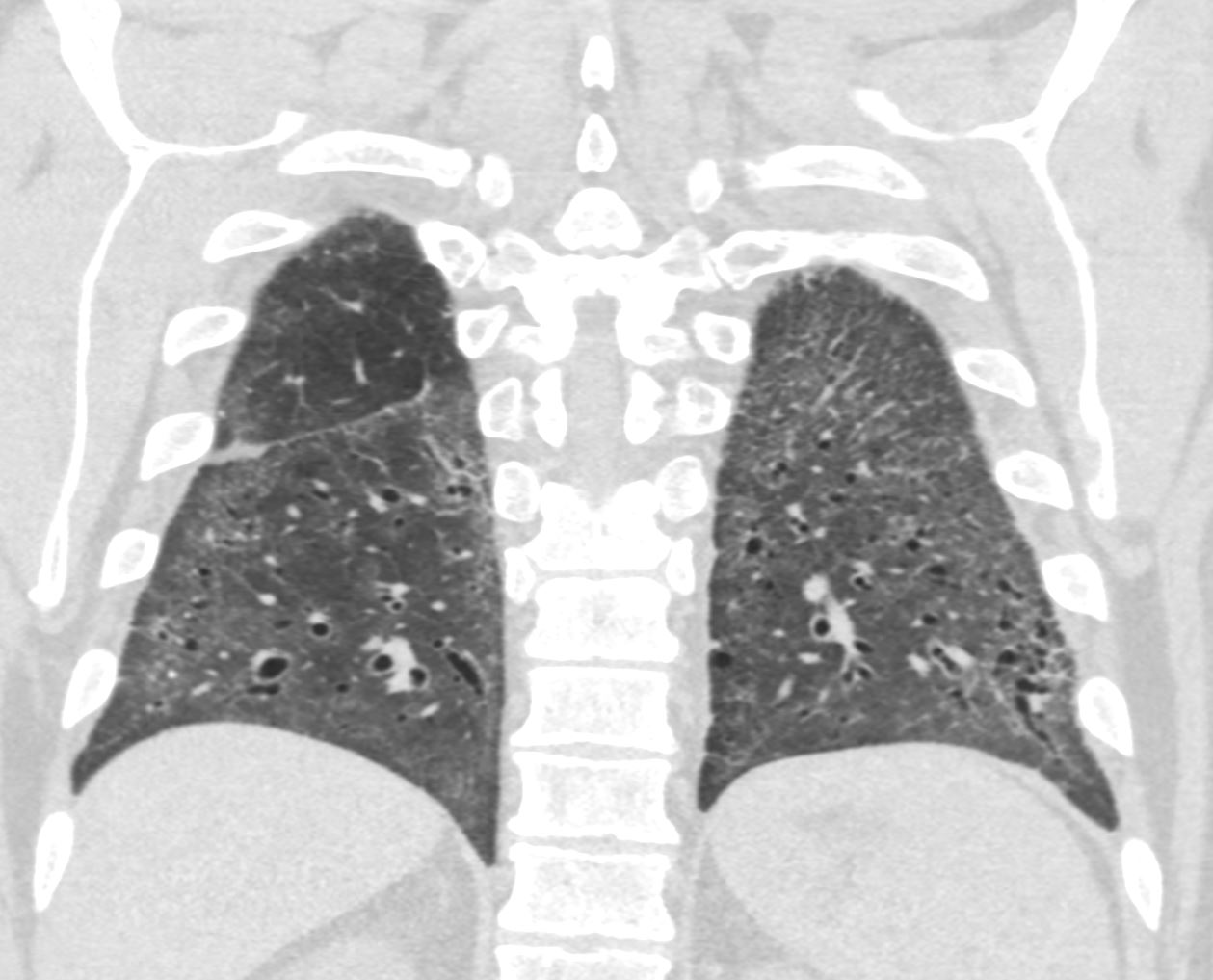
Lower Lobe distribution – apico-basilar gradient
Ashley Davidoff MD TheCommonvein.net lungs-0771
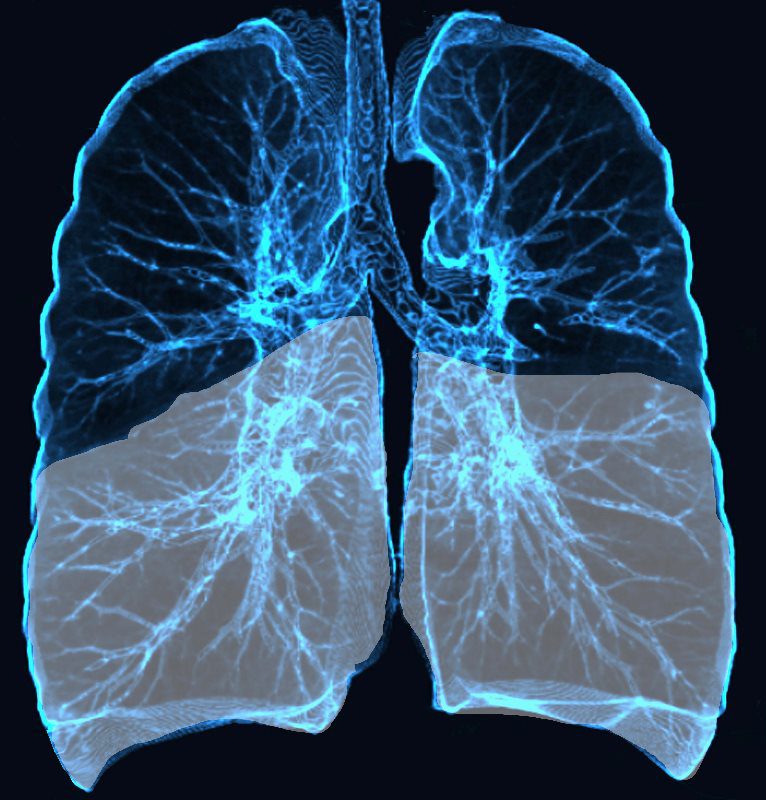
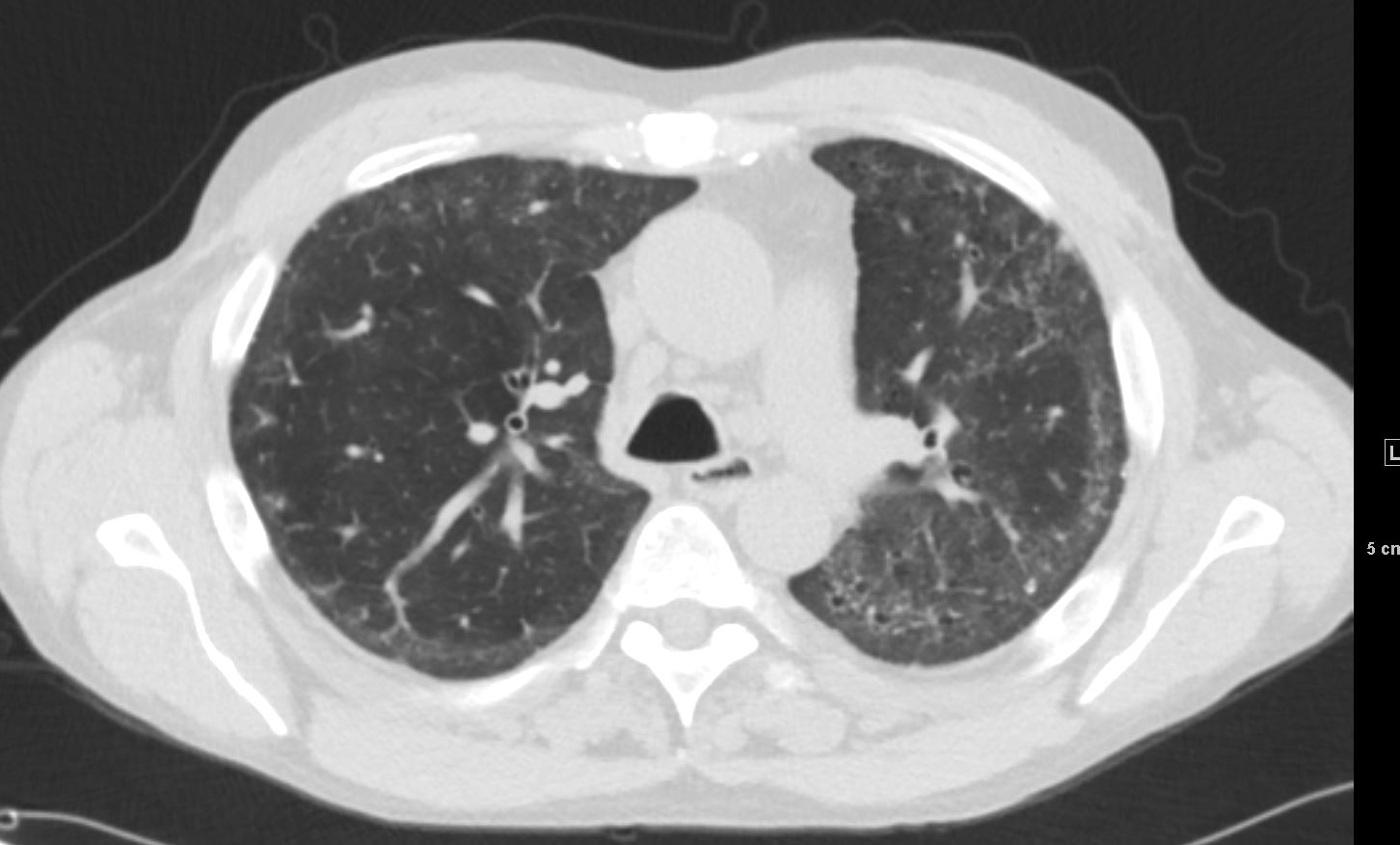
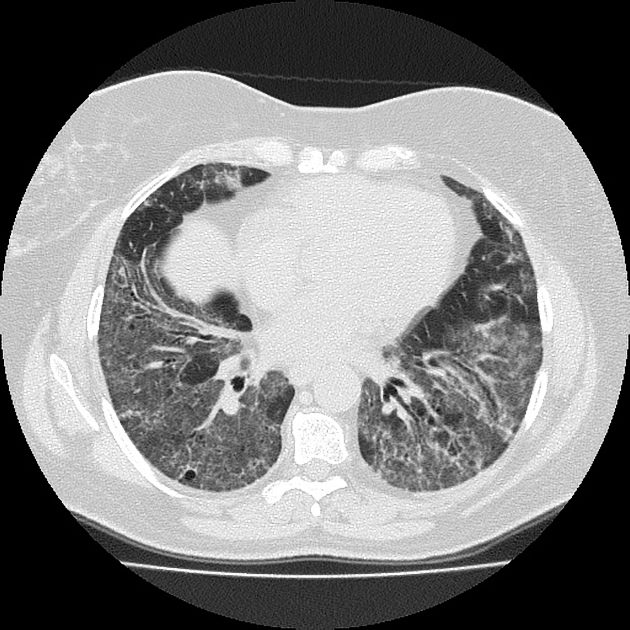
Broncho vascular and inter- alveolar interstitial fibrosis dominantly in the lower lobes but affecting the middle and upper lobes to lesser extent resulting in bronchiectasis and reticulations. The overall increase in density results in ground glass changes
Ashley Davidoff MD TheCommonvein.net lungs-0738 NSIP

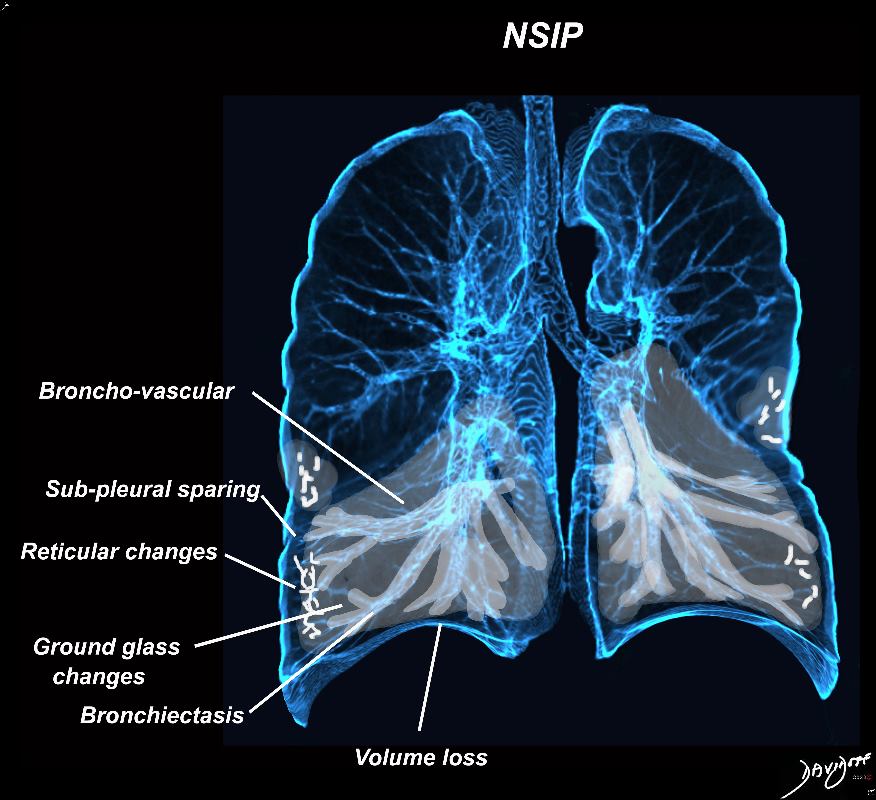
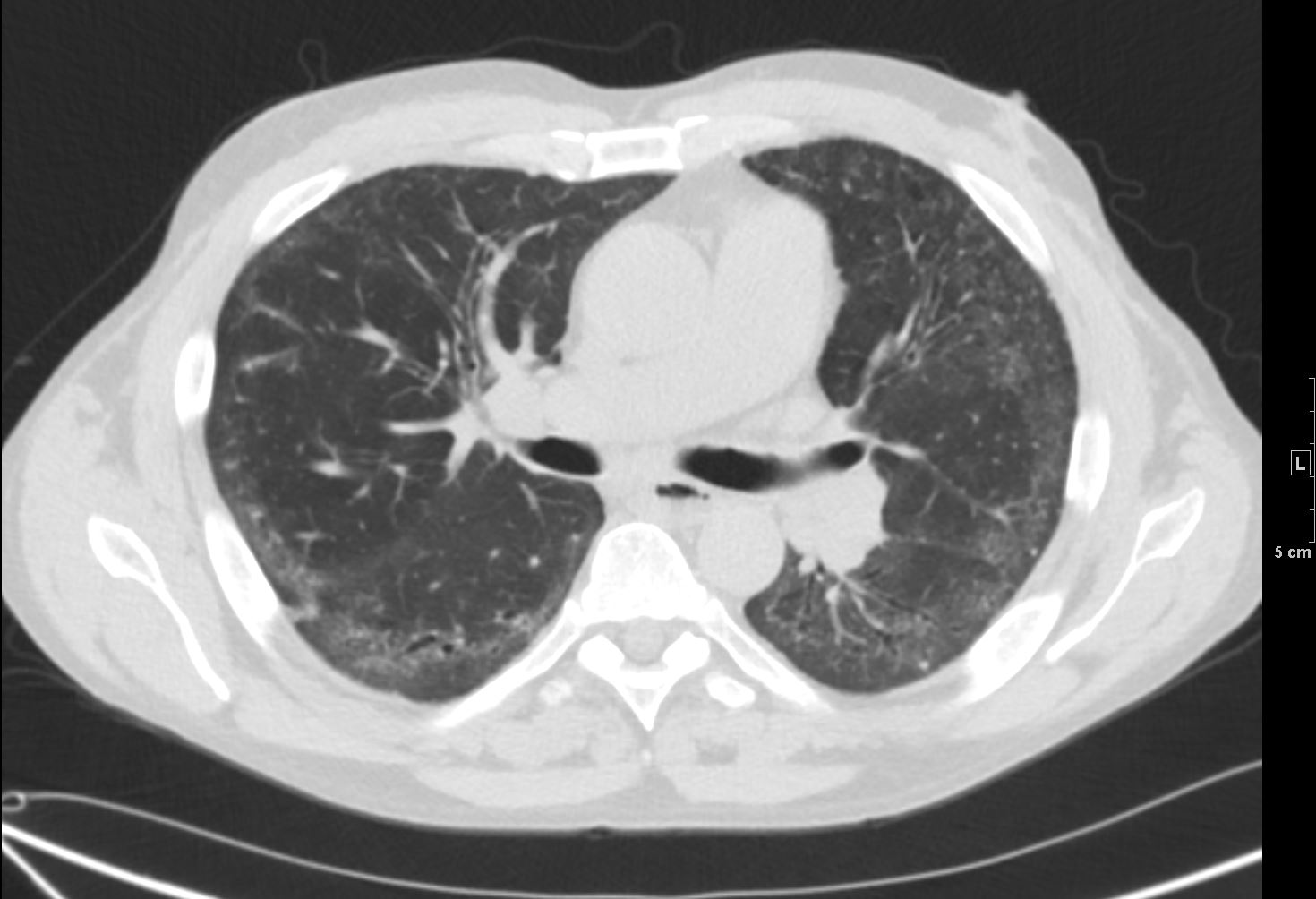
Broncho vascular distribution associated with peripheral sparing, ground glass changes, reticulations, and volume loss, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes
Ashley Davidoff MD TheCommonvein.net lungs-0771b
Broncho vascular distribution associated with peripheral sparing, ground glass changes, reticulations, and volume loss, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes
Ashley Davidoff MD TheCommonvein.net lungs-0771b
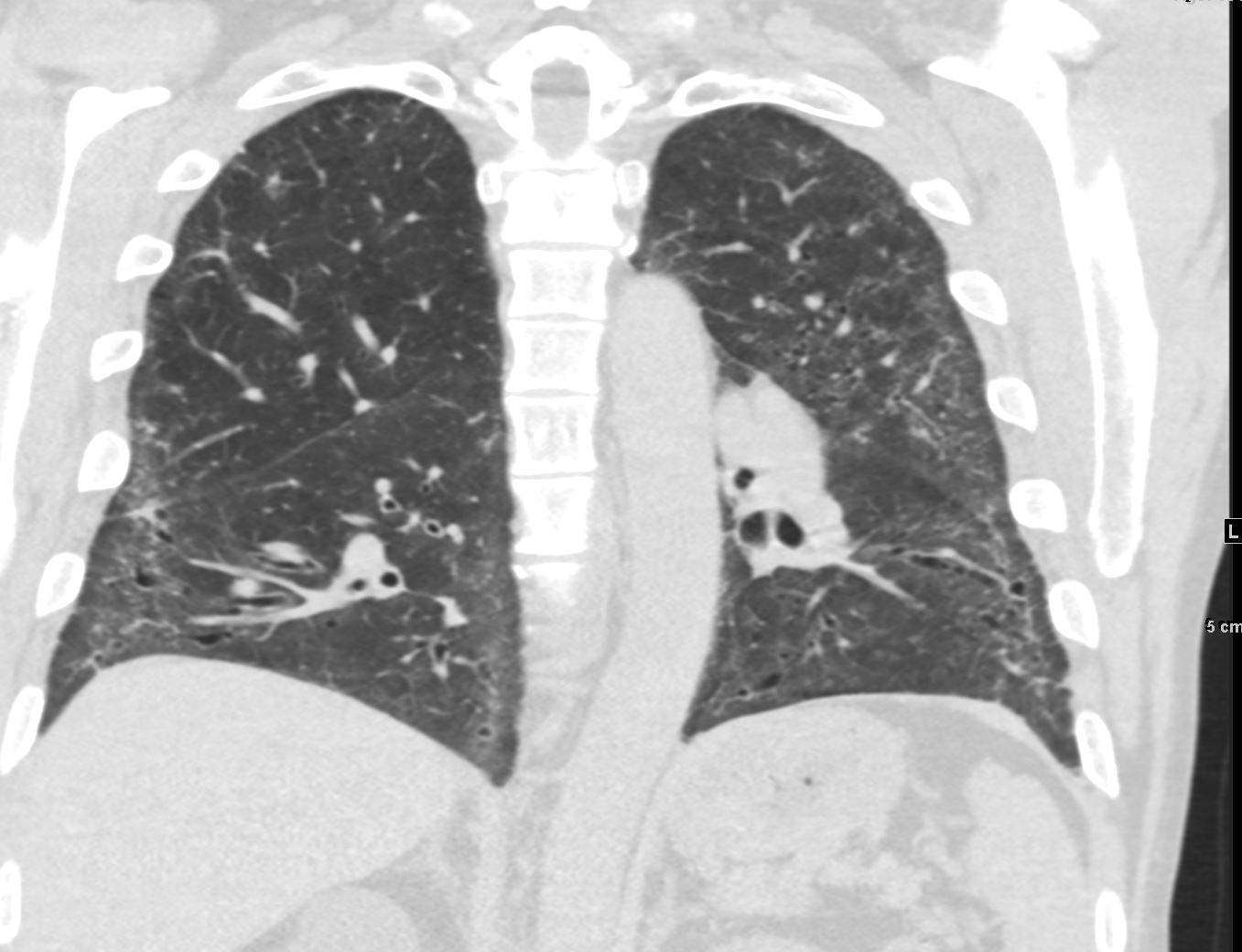
Fibrotic NSIP
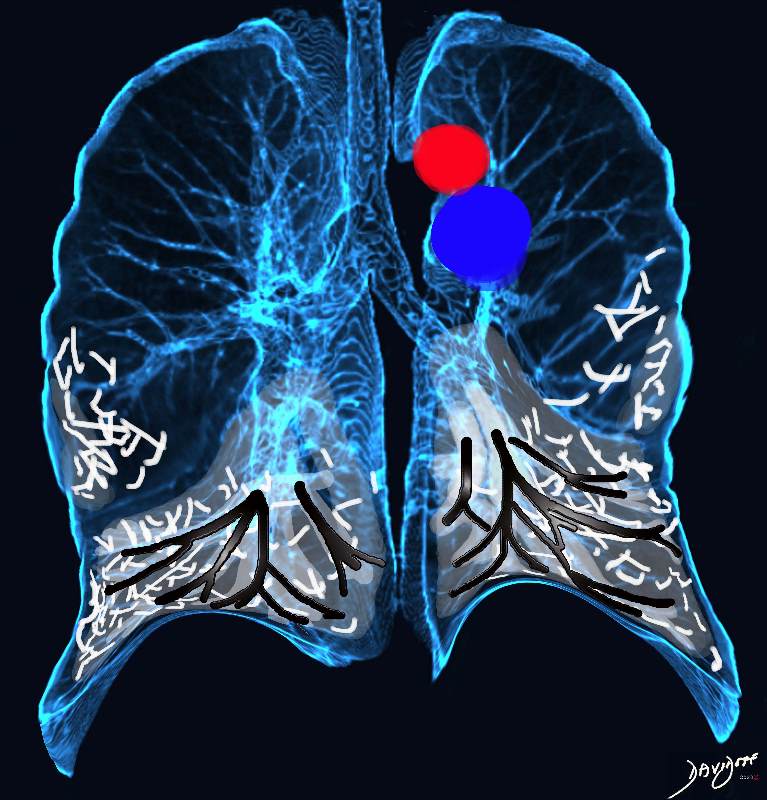
Broncho vascular distribution associated with increased reticular changes, more prominent traction bronchiectasis, decreased lung volumes , and decreased lung volumes, dominantly in the lower lobes but to some extent in the middle lobe and upper lobes. Pulmonary hypertension becomes more common.
Ashley Davidoff MD TheCommonvein.net lungs-0771d
Starts Central and Spreads Outward Along the Bronchovascular bundle
peribronchovascular
symmetric
ground glass
reticulation
traction bronchiectasis
loss of volume
subpleural sparing 60-65%
confluent
reticular
consolidations
honeycomb rare
Interlobular septa
can be thickened.
Alternatively All the S’s
subpleura
sparing
symmeteric
ground glass
scleroderma sle and all the other s’s arthritis, vasculitis
basal
? Interlobular septa
In general not progressive
May get better on Rx
Size
thickening of bronchovascular bundles
Shape
Position
subpleural (subpleural sparing, specific for NSIP but other causes eg small airway disease)
relatively symmetric
apico-basilar gradient
Character
ground glass
fine reticulation
reticular opacities and irregular linear opacities (sometimes – minor subpleural reticulation)
Associated Findings
volume loss
traction bronchiectasis
Classical Subpleural Sparing






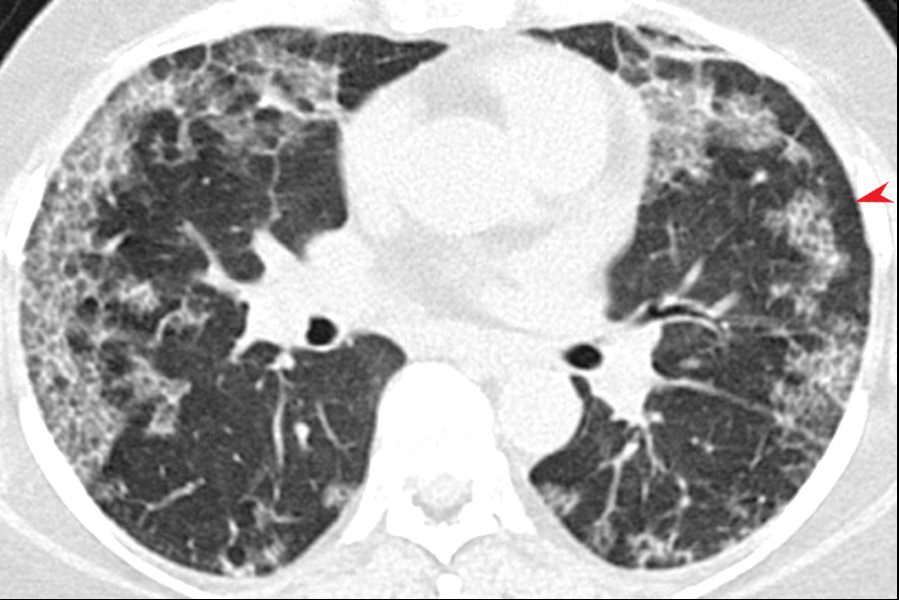
CT scan through the chest shows relatively symmetrical and peripherally positioned ground glass infiltrates with a region of subpleural sparing (red arrowhead)
Courtesy Pathology Outlines
http://www.pathologyoutlines.com/
http://www.pathologyoutlines.com/
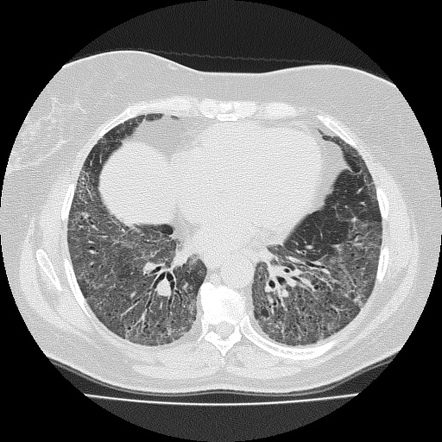
CT scan through the lower lobes showing basilar ground glass opacification with peribronchial thickening and traction bronchiectasis
Courtesy pathology Outlines
http://www.pathologyoutlines.com/
CT scan through the lower lobes showing basilar ground glass opacification, with fine reticulation
Courtesy pathology Outlines
http://www.pathologyoutlines.com/
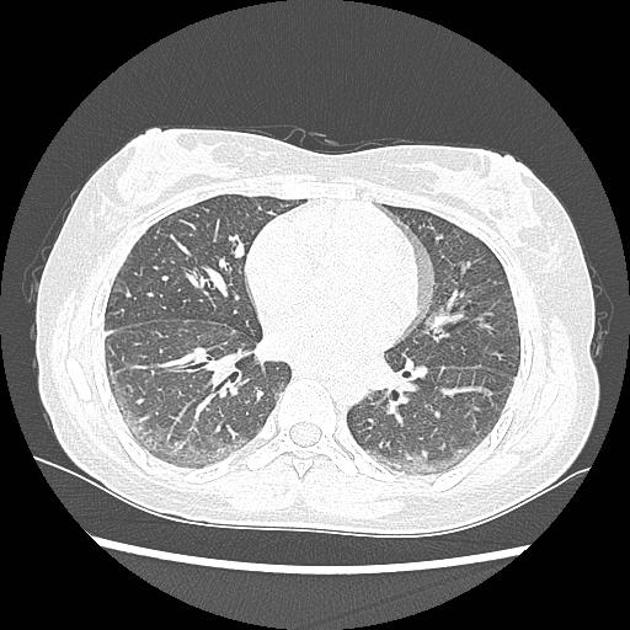
CT scan through the lower lobes showing basilar ground glass opacifictaion with peribronchial thickening and traction bronchiectasis
Courtesy pathology Outlines
http://www.pathologyoutlines.com/

NSIP
CT scan through the lower lobes showing basilar ground glass opacifictaion with peribronchial thickening and traction bronchiectasis
Courtesy pathology Outlines
http://www.pathologyoutlines.com/TYPICAL FINDINGS IN NSIP
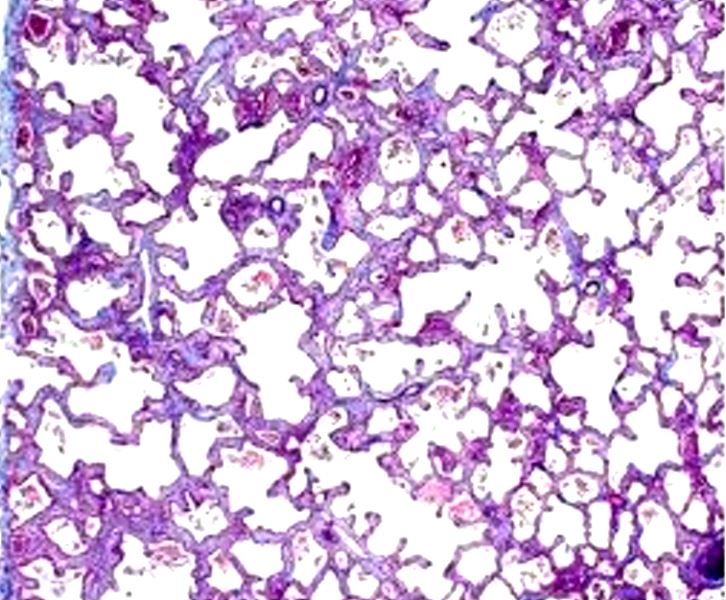
Spatially homogeneous pattern of fibrosis seen in non specific interstitial pneumonia (NSIP) (trichrome stain X40)
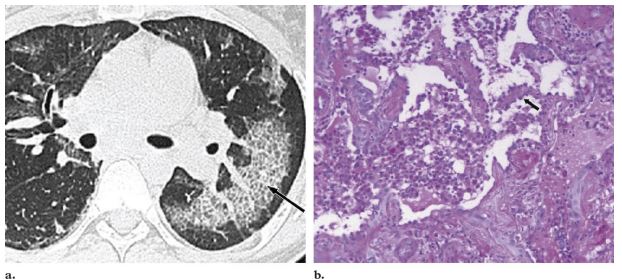
Courtesy Medscape eMedicineMethotrexate-induced NSIP in a 41-year-old woman with rheumatoid arthritis who presented with dyspnea and decreased diffusing capacity of the lungs for carbon monoxide (Dlco). (a) High-resolution CT scan shows
scattered ground-glass attenuation and thickened inter- and intralobular lines (arrow). (b) Photomicrograph (original
magnification, 400; hematoxylin-eosin stain) of a specimen from lung biopsy shows patchy interstitial fibrosis, expansion of the interstitium by chronic inflammatory infiltrates, and reactive hyperplastic type II pneumonocytes (arrow), findings consistent with NSIP induced by the pulmonary toxic effects of methotrexate.
Diffuse mucinous bronchioloalveolar carcinoma in a 78-year-old man. (a) High-resolution CT scan
shows a bilateral crazy-paving pattern and centrilobular nodules. (b) Photomicrograph (original magnification,
400; hematoxylin-eosin stain) of a specimen from open lung biopsy shows replacement of the alveolar epithelium
by epithelial neoplastic cells with abundant intracytoplasmic mucin (arrows).
Rossi, S.E et al “Crazy-Paving” Pattern at Thin-Section CT of the Lungs: RadiologicPathologic Overview Radiographics Volume 23 – Number 6, 2003-
Cellular NSIP and Fibrotic NSIP
- NSIP can be divided into two subtypes based on the predominant histological pattern seen on lung biopsy: cellular NSIP and fibrotic NSIP.
- In Cellular NSIP, the lung tissue is
- relatively little fibrosis. In contrast,
- CT
- patchy or diffuse ground-glass opacities
- may be associated with a reticular pattern and
- traction bronchiectasis
- more pronounced in the
- peripheral regions of the lungs, and may be
- subpleural or
- peribronchovascular
- may also be consolidation in some areas of the lung.
- CT
- In Fibrotic NSIP
- presence of fibrosis or
- scarring within the lung tissue.
- worse prognosis c
- more severe respiratory symptoms,
- lower lung function, and a
- greater likelihood of developing pulmonary hypertension.
- CT
- shows more pronounced and
- diffuse reticular opacities and
- traction bronchiectasis, with
- less ground-glass opacities
- fibrotic changes may be
- more extensive and involve
- larger areas of the lung tissue.
- may also be
- honeycombing in advanced cases.
- CT
- The fibrotic form of nonspecific interstitial pneumonia (NSIP) is a
subtype characterized by a predominant pattern of lung fibrosis,
with varying degrees of inflammation. Unlike the cellular form, the
fibrotic form involves more extensive scarring of the lung
interstitium, leading to thickening and stiffening of the lung tissue.
This subtype is often associated with autoimmune diseases (like
systemic sclerosis, rheumatoid arthritis, or dermatomyositis) and
can also occur as an idiopathic condition. Diagnosis is based on
high-resolution CT (HRCT) scans, which often reveal reticular
opacities, traction bronchiectasis, and subpleural sparing, but
typically lack honeycombing. A lung biopsy may be necessary to
confirm the diagnosis. The fibrotic form of NSIP generally has a less
favorable prognosis than the cellular form, as the extent of fibrosis
limits the reversibility of the condition, though some patients may
still respond to immunosuppressive therapies.
Radiopedia
Primarily idiopathic but the morphological pattern can be seen in association with a number of conditions:
- connective tissue disorders
- other autoimmune diseases
- drug-induced lung disease: especially chemotherapy agents 4
- hypersensitivity lung disease
- slowly healing diffuse alveolar damage (DAD)
- relapsing organizing pneumonia
- occupational exposure
- immunodeficiency (mainly HIV infection) 13
- graft versus host disease (GVHD) 13
- immunoglobulin G4 (IgG4)-related sclerosing disease, with or without overlap features with Rosai-Dorfman disease 13
- multicentric Castleman disease 13
- myelodysplastic syndrome 13
-
- INTERSTITIAL PNEUMONIA , IP
-
- Usual interstitial pneumonia (UIP)
- Nonspecific interstitial pneumonia (NSIP)
- Cryptogenic organizing pneumonia (COP)
- Desquamative interstitial pneumonia (DIP)
- Respiratory bronchiolitis-interstitial lung disease (RB-ILD)
- Acute interstitial pneumonia (AIP)
- Lymphoid interstitial pneumonia (LIP)
- Idiopathic pleuroparenchymal fibroelastosis (PPFE)
-
- INTERSTITIAL PNEUMONIA , IP
References and Links
Videos