AKA
Mediastinal emphysema
What is it?
Pneumomediastinum is a condition characterized by the abnormal presence of free air within the mediastinal space. It can occur spontaneously or secondary to trauma, medical procedures, or other underlying conditions.
Caused by:
- Most common causes
- Spontaneous pneumomediastinum: Often due to alveolar rupture with air dissecting along the bronchovascular sheath into the mediastinum (e.g., Valsalva maneuver, severe coughing, vomiting).
- Traumatic pneumomediastinum: Blunt or penetrating trauma to the chest, esophageal rupture (Boerhaave syndrome).
- Other causes include:
- Infections: Necrotizing infections (e.g., gas-forming organisms such as Clostridium).
- Inflammation/Immune: Rarely associated with connective tissue diseases.
- Mechanical Trauma: Tracheal or bronchial injury, barotrauma (e.g., from mechanical ventilation).
- Iatrogenic: Post-procedural complications (e.g., endoscopy, tracheostomy, chest tube insertion).
- Metabolic: Rare cases in hyperventilation syndromes.
- Inherited/Congenital: Associated with conditions such as Marfan syndrome.
Resulting in:
- Compression of mediastinal structures (rare in mild cases).
- Potentially life-threatening complications, such as tension pneumomediastinum or mediastinitis.
Structural changes:
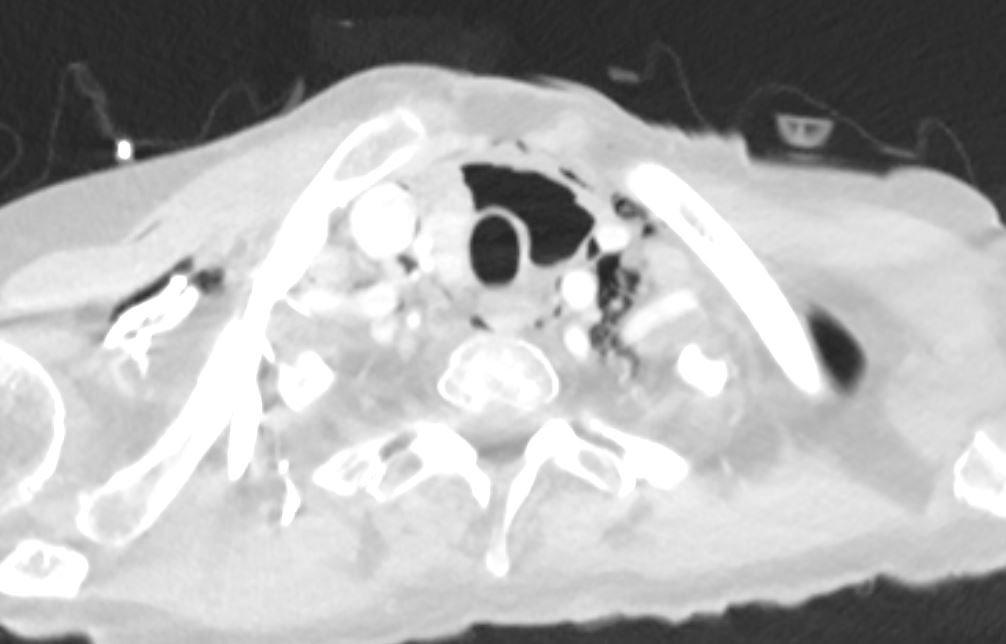
- Air accumulation within the mediastinum, potentially dissecting along fascial planes into the neck, pericardium, or retroperitoneum.
Pathophysiology:
- Alveolar rupture increases intra-alveolar pressure (Macklin effect), allowing air to escape into the interstitium and track along bronchovascular bundles into the mediastinum.
Pathology:
- Microscopic evidence of ruptured alveoli and air dissecting through connective tissue planes.
- Gross evidence of free air in the mediastinal space.
Diagnosis:
- Clinical:
- Symptoms: Chest pain, dyspnea, neck pain, dysphagia, or subcutaneous emphysema.
- Signs: Subcutaneous crepitus, Hamman’s sign (crunching sound synchronous with heartbeat).
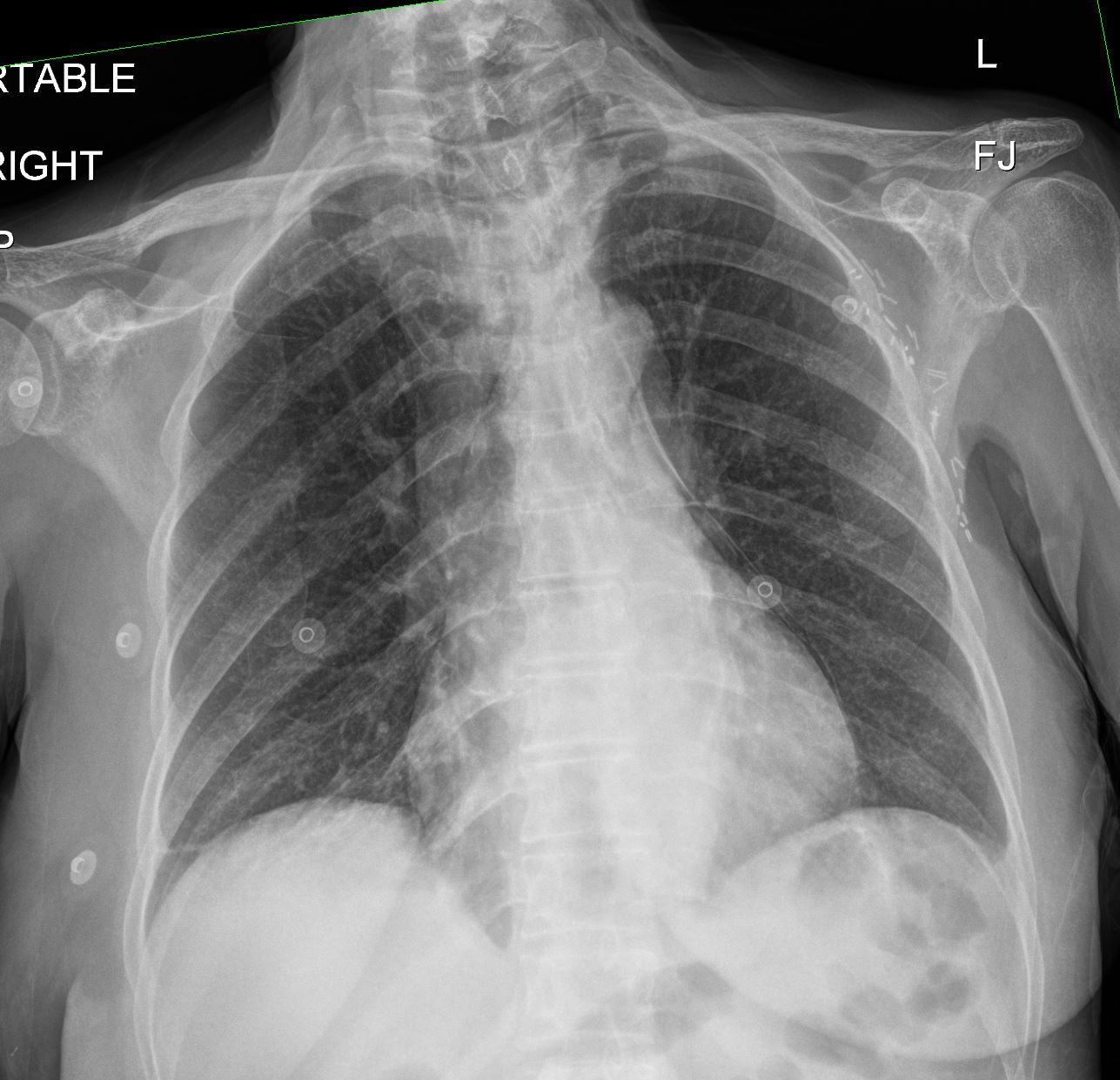
- Radiology:
- CXR: Mediastinal air outlining structures (e.g., aorta, heart, trachea).
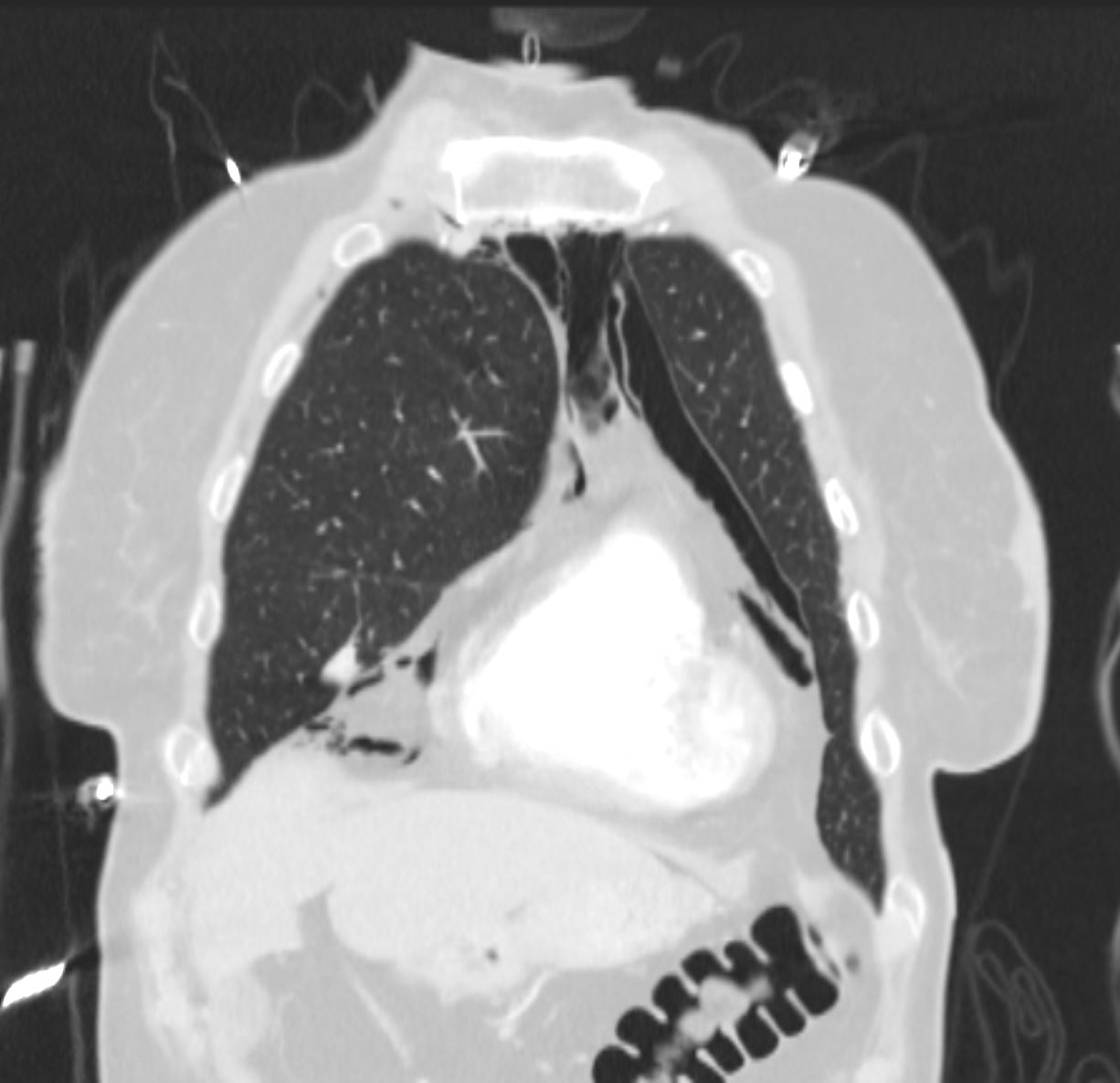
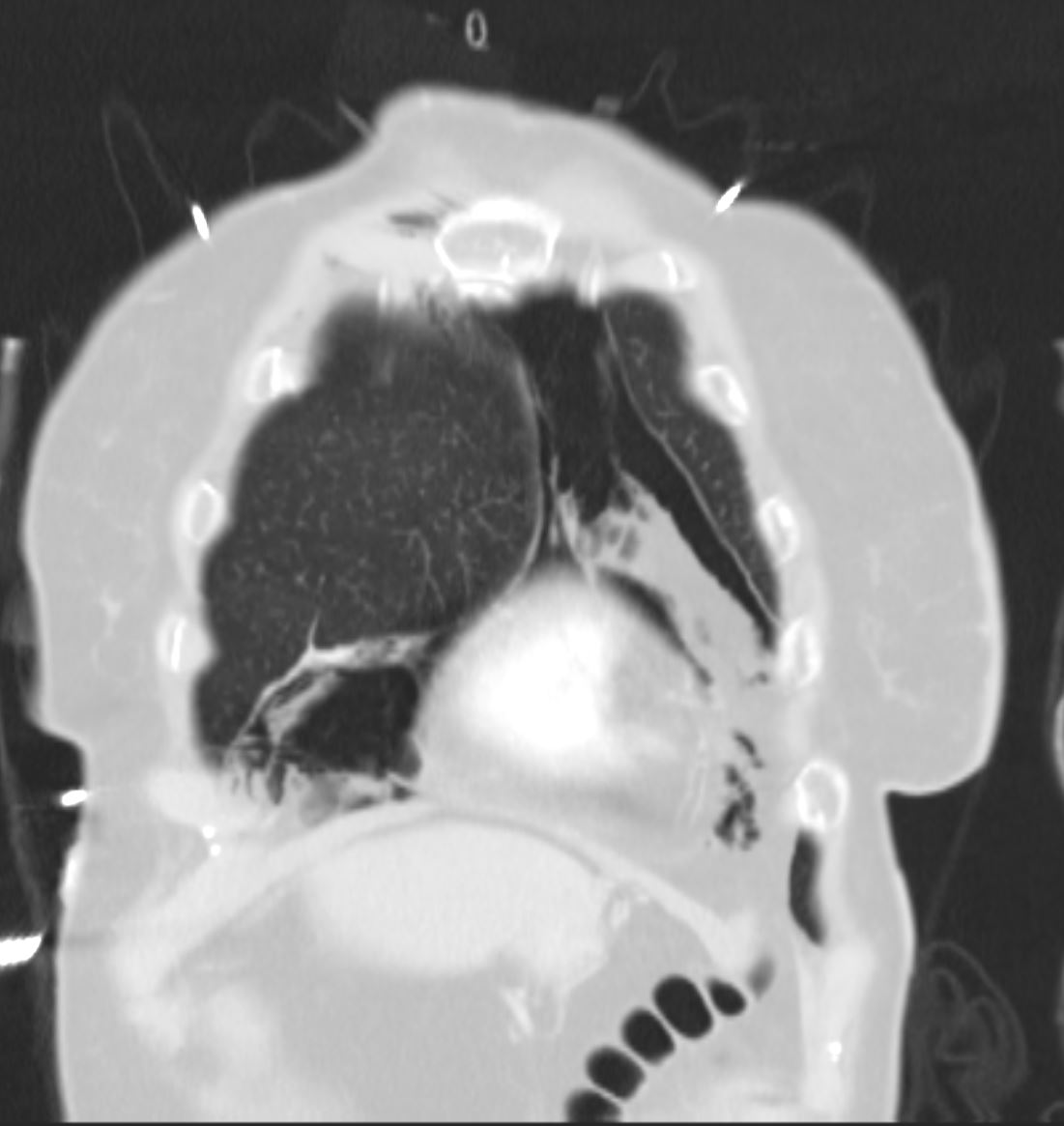
- CT: More sensitive, showing mediastinal air and the site of origin (e.g., alveolar rupture, esophageal perforation).
- Labs:
- Elevated white blood cell count in cases with infection or mediastinitis.
- Arterial blood gas: May show hypoxemia in severe cases.
Management:
- Conservative management (most cases):
- Observation, analgesia, and supplemental oxygen to enhance reabsorption of air.
- Surgical or procedural intervention:
- Indicated for tension pneumomediastinum, significant esophageal rupture, or tracheobronchial injury.
Radiology Detail:
- CXR:
- Findings: Mediastinal air outlining the heart, aorta, or trachea.
- Associated Findings: Subcutaneous emphysema or pneumothorax.
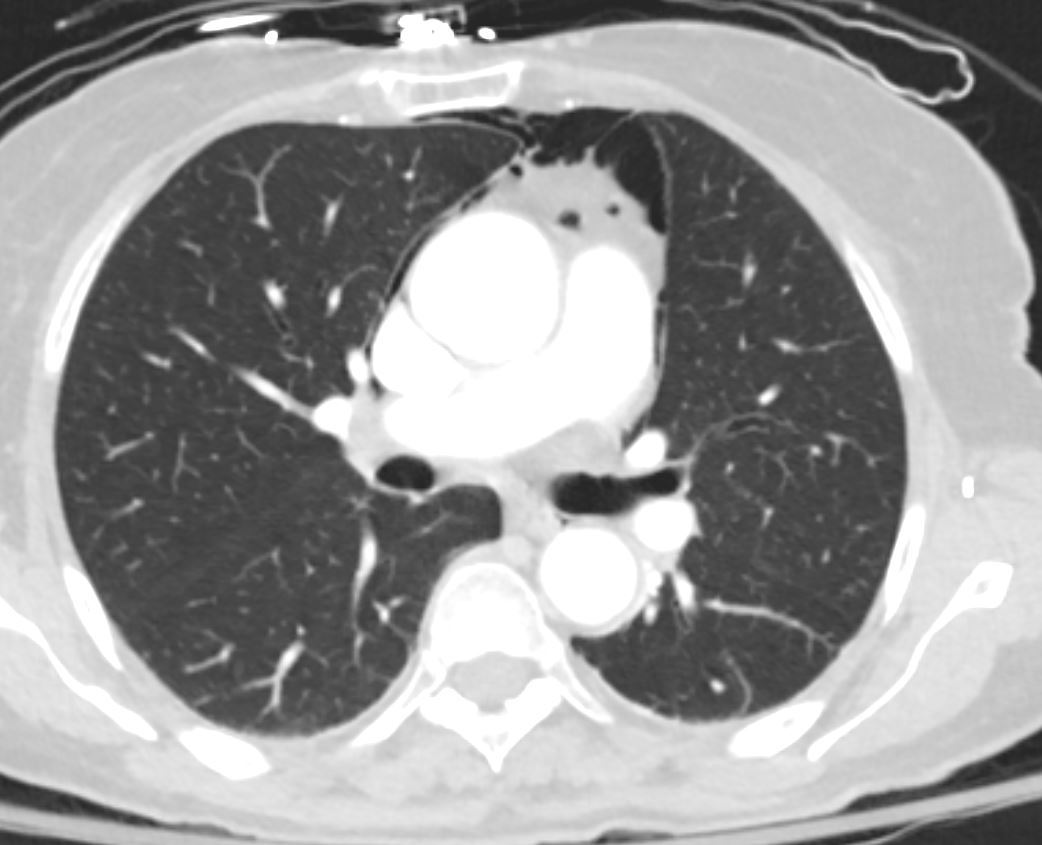
- CT:
- Parts: Mediastinal space, pleural spaces, lung parenchyma.
- Size: Varies with the volume of air.
- Shape: Irregular collections of air outlining mediastinal structures.
- Position: Along the mediastinal compartment, tracking into neck or retroperitoneum.
- Character: Free air with no mass effect unless severe.
- Time: Air may persist for hours to days.
- Associated Findings: Pneumothorax, tracheal or esophageal rupture.
- Specific Signs:
- Continuous Diaphragm Sign: Air outlines the inferior heart border, making the central diaphragm visible.
- Naclerio’s V-sign: V-shaped lucency formed by air outlining the descending aorta and diaphragm.
- Thymic Sail Sign (in children): Elevated thymus caused by mediastinal air.
- Other relevant Imaging Modalities:
- MRI: Rarely used; may demonstrate associated soft tissue changes.
- Ultrasound: Can detect subcutaneous emphysema or tension pneumothorax.
Pulmonary Function Tests (PFTs):
- Rarely performed; not typically indicated in acute cases.
Recommendations:
- Identify and treat the underlying cause (e.g., infection, trauma).
- Monitor for complications such as tension pneumomediastinum or mediastinitis.
- Ensure appropriate oxygenation and pain management.
Key Points and Pearls:
- Spontaneous pneumomediastinum often resolves with conservative management and has a benign prognosis.
- CXR and CT are crucial for diagnosis, with CT being more sensitive in detecting small volumes of air.
- The Macklin effect explains the pathogenesis of spontaneous pneumomediastinum.
- Rarely, pneumomediastinum can progress to life-threatening complications like tension pneumomediastinum or mediastinitis.
S/P thyroidectomy