
Pneumothorax
-
Pneumothorax
- Etymology:
- Derived from Greek: “pneuma” meaning air and “thorax” meaning chest, describing air in the chest cavity outside the lungs.
- AKA:
- Collapsed lung (colloquial term).
- What is it?
- Pneumothorax refers to the presence of air in the pleural space, disrupting the negative pressure that keeps the lung inflated.
- Classification Based on :
- Based on Size:
Small (less than 2 cm from lung margin to chest wall or approximately 15% of lung volume).
Moderate (2-4 cm or 30% of lung volume).
Large (greater than 4 cm or exceeding 50% of lung volume, or complete lung collapse).
Tension Pneumothorax:
A life-threatening condition with progressive accumulation of air causing hemodynamic compromise.
- Based on Content:
- Simple Pneumothorax (air only).
- Hydrothorax (air and fluid).
- Hemothorax (air and blood).
- Pyothorax (air and pus).
- Pneumothorax with Trapped Lung:
- Occurs when lung expansion is restricted by pleural adhesions or fibrosis, often seen in patients with previous pleural disease.
- Based on Size:
- Caused by:
- Trauma (e.g., rib fractures, penetrating chest wounds).
- Iatrogenic causes (e.g., complications from lung biopsies or central line placements).
- Spontaneous rupture of subpleural blebs or bullae (common in primary spontaneous pneumothorax).
- Underlying lung diseases (e.g., COPD, asthma, cystic fibrosis, interstitial lung diseases, Pneumocystis jiroveci pneumonia [PJP], sarcoidosis, lymphangioleiomyomatosis (LAM), Pulmonary Langerhans Histiocytosis, Marfan syndrome, and rarely, endometriosis-associated thoracic pathology.).
- Resulting in:
- Impaired oxygenation and ventilation due to partial or complete lung collapse.
- Hemodynamic instability in the case of tension pneumothorax.
- Increased risk of recurrence, especially in spontaneous pneumothorax.
- Progression to respiratory failure if untreated.
- Characterized by:
- A sharp pleural line visible on imaging.
- Absence of lung markings distal to the pleural line.
- Varying degrees of lung collapse.
- Anatomically affecting:
- The pleural space between the visceral and parietal pleura.
- Lungs and, in tension pneumothorax, potentially the mediastinum.
- Pathophysiology:
- Air in the pleural space disrupts negative pleural pressure, causing partial or complete lung collapse.
- In tension pneumothorax, progressive air accumulation leads to mediastinal shift, impairing venous return and cardiac output.
- Diagnosis
- Clinical Diagnosis:
- Sudden onset of pleuritic chest pain and dyspnea.
- Physical findings may include decreased or absent breath sounds on the affected side, hyperresonance to percussion, and in severe cases, tracheal deviation (in tension pneumothorax).
- Clinical Diagnosis:
Imaging
- Applied Anatomy to Imaging Principles
- This section provides insights into the structural and functional relationships observed through various imaging modalities for pneumothorax. It aims to bridge anatomical understanding with radiological interpretation, enhancing diagnostic accuracy and clinical decision-making.
- Parts: Pleural space, lung, mediastinum (in tension pneumothorax).
- Size: Radiologists distinguish pneumothorax size by the extent of air in the pleural space:
- small (less than 2 cm from the lung margin to chest wall at the level of the hilum or approximately 15% of lung volume),
- moderate (2-4 cm or 30% of lung volume), and
- large (greater than 4 cm or exceeding 50% of lung volume, or causing complete collapse of the lung).
- Shape: Non-dependent air collection; sharp pleural line conforming to the crescentic shape of the apex in the upright exam. In cases of previous pleural disease with adhesions, the shape may become irregular or localized due to tethering by fibrotic bands.
- Position:
- In upright X-rays, air collects at the apex or upper zones first, while in supine X-rays, air may collect in the anterior pleural space and appear as a deep sulcus sign.
- Character:
- Absence of lung markings beyond pleural line.
- Time:
- Acute onset;
- tension pneumothorax progresses rapidly.
- CXR:
- Visible pleural line with no lung markings beyond it.
- Deep sulcus sign in supine patients.
- Care should be taken to differentiate true pneumothorax from pseudopneumothorax, which can be caused by skin folds, overlapping soft tissues, or external artifacts mimicking a pleural line on imaging.
- CT:
- Most sensitive for detecting small pneumothoraces.
- Identifies associated findings such as bullae or underlying disease.
- Ultrasound:
- Absence of lung sliding and the lung point are diagnostic findings.
- Differential Diagnosis:
- Bullae or blebs mimicking pneumothorax.
- Subcutaneous emphysema.
- Large cysts in cystic lung diseases.
- Recommendations:
- Small Pneumothorax: Observe with serial imaging and oxygen therapy.
- Large or Symptomatic Pneumothorax: Needle aspiration or chest tube placement.
- Tension Pneumothorax: Immediate needle decompression is lifesaving.
- Key Points and Pearls:
- Always assess for tension pneumothorax in cases of hemodynamic instability.
- Patient body habitus, particularly being a young, thin male or female with an asthenic build, is a risk factor for spontaneous pneumothorax.
- Ultrasound is highly sensitive and useful in emergency settings.
- CT can identify subtle pneumothoraces and underlying causes (e.g., bullae, blebs, or trauma).
- Etymology:
The diagnosis is suspected clinically and confirmed by CXR.

Pneumothorax
This case shows a chest x-ray of a patient who had a lung biopsy which was complicated by a pneumothorax and a small amount of pleuroparenchymal hemorrhage. The two components of the pleural layer have been separated and the cohesive/adhesive forces have been disrupted by the air which now intervenes and disturbs the physics of the capillary action. The parietal pleura remains attached to the chest wall while the visceral pleura remains attached to the lung. This is a small pneumothorax and had no effect on the patient or the mechanics of lung movement. In this case we followed the patient with a CXR at 2 and 4 hours later. When no progression was demonstrated we allowed the patient to be discharged home with special instructions to limit activities till the next day. In this case there is an abnormal increase in the density of the visceral pleura
Ashley Davidoff MD TheCommonVein.net 42041b01

The above image is a magnified view of the pneumothorax.
Courtesy Ashley Davidoff MD TheCommonVein.net 42041b02
Treatment depends on the size of the pneumothorax. When large a pigtail catheter or formal chest is used and when small close observation is necessary. tension pneumothorax is an emergency and when suspected immediate decompression with a large bore needle should be attempted.
Accumulation of air in the pleural space leading to collapse of the underlying lung can occur spontaneously in tall and slim young adults or in patients with history of emphysema. Such patients usually present with an acute onset of unilateral pleuritic pain that may be associated with dyspnea. Depending on the size of the pneumothorax, it can be managed conservatively by observation or by evacuation of the air through placement of a chest tube.
Unusual Cases
Parekh, M et al Review of the Chest CT Differential Diagnosis of Ground-Glass Opacities in the COVID Era Radiology Vol. 297, No. 3 July 2020

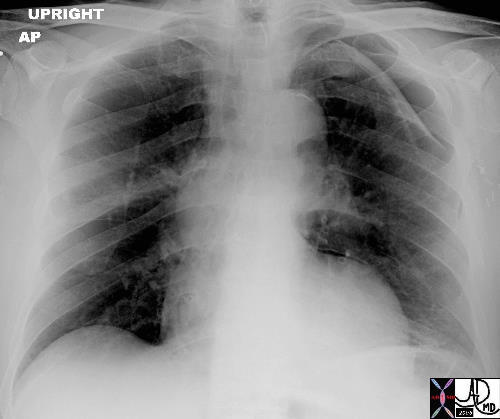
50-year-old male presents with history of Stage 4 sarcoidosis acute chest pain and dyspnea
The initial CXR shows a left sided pneumothorax, diffuse nodular pattern with confluent perihilar infiltrates and a left pleural effusion
Ashley Davidoff MD
This is the type of CXR that sends shivers down the spine. The overall blackness of the left chest cavity, in association with a nubbin of lung tissue in the ipsilateral hilum and rightward mediastinal shift is characteristic of a tension pneumothorax with total atelectasis of the left lung. Immediate and urgent decompression with a chest drain is indicated.
Courtesy of: Ashley Davidoff, M.D.
Loculated Pneumothorax
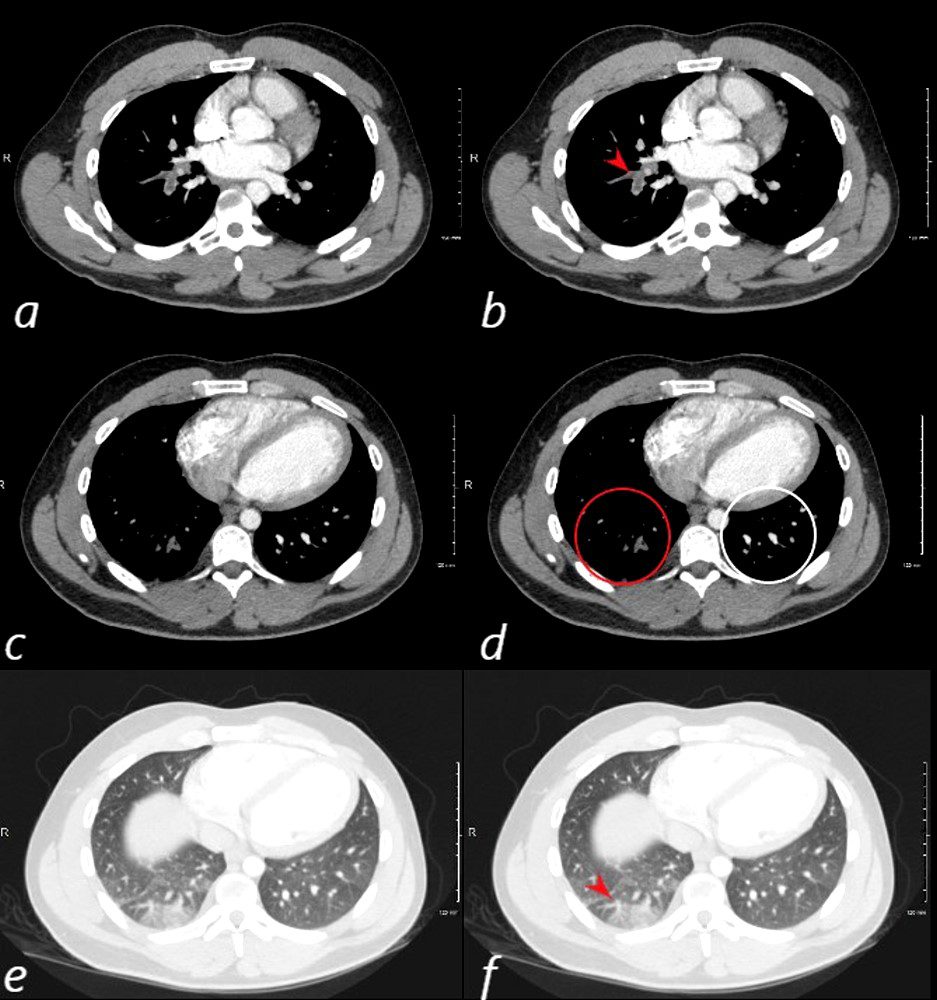
24 year old male with SLE presented with chest pain and dyspnea and initial CT showed occlusive pulmonary emboli to the right lower lobe (a,b, red arrowhead) with total occlusion of the right lobe artery extending into posterior basal segmental vessels (red ring d compared with normal vessels surrounded by white rin (d). An associated wedge shaped ground glass region is noted (e,f red arrowhead) representing either hemorrhage or early infarction
Ashley Davidoff MD
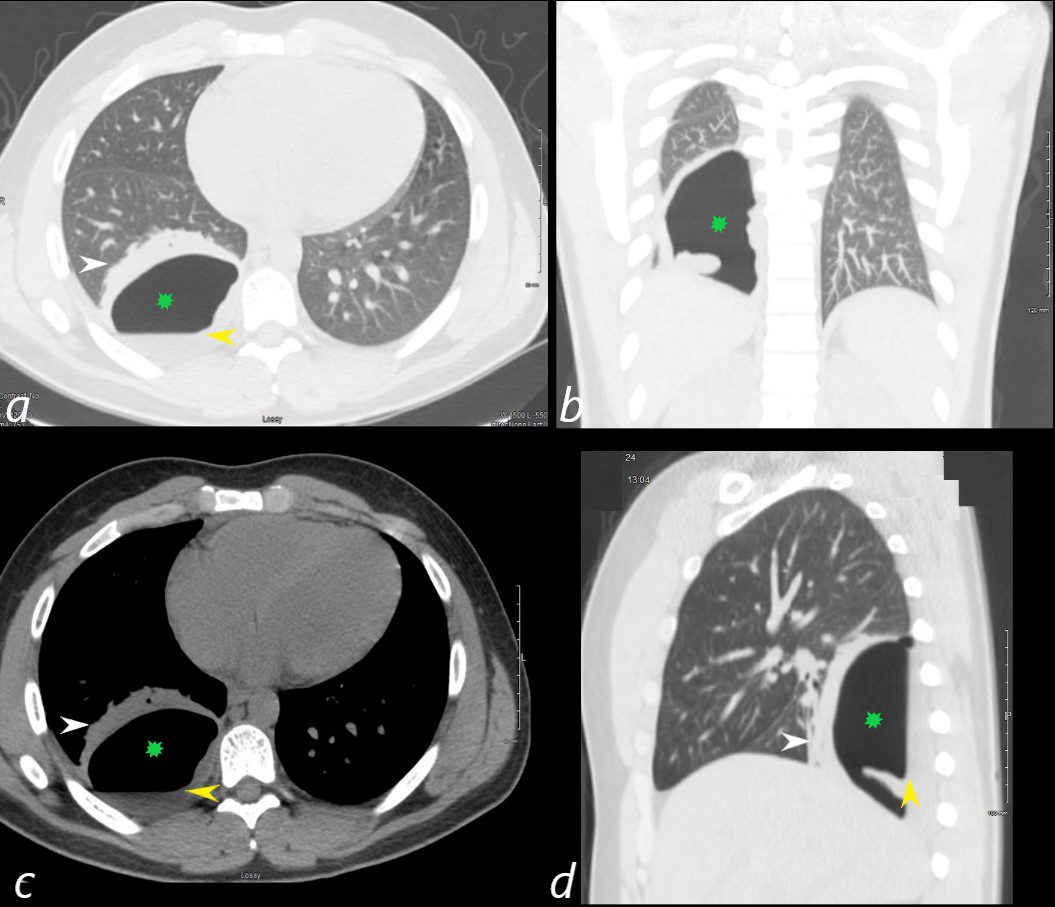
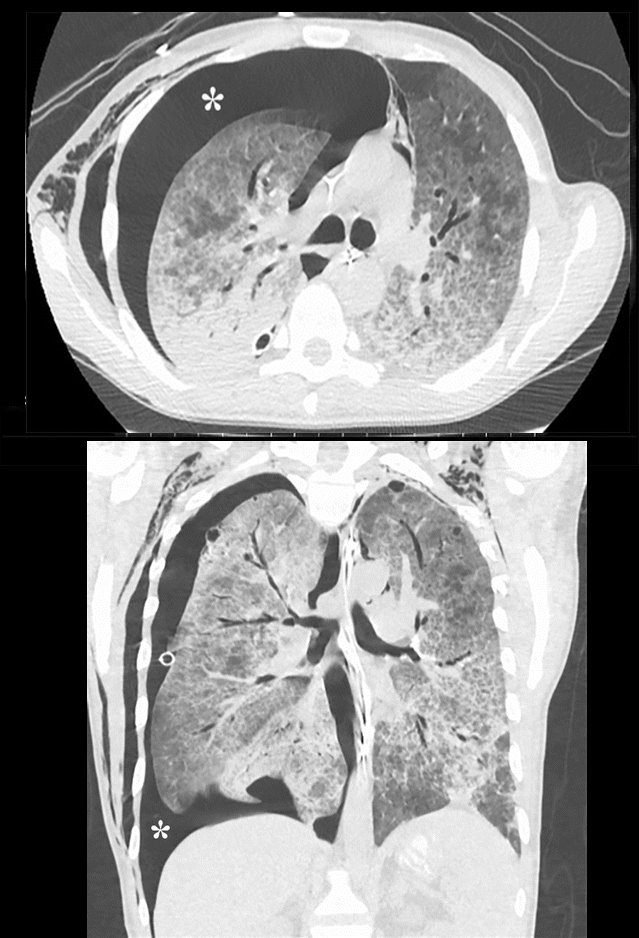
24 year old male with SLE presented with chest pain and dyspnea and initial CT showed occlusive pulmonary emboli to the right lower lobe initially associated with a wedge shaped ground glass region. 2 weeks later this evolved into a bronchopleural fistula, with a loculated pneumothorax in the right lower lobe (green star in a,b,c,d).with an air fluid level (yellow arrowhead in a,c,d) and a region of compressive atelectasis (white arrowhead a,c,d).
Ashley Davidoff MD
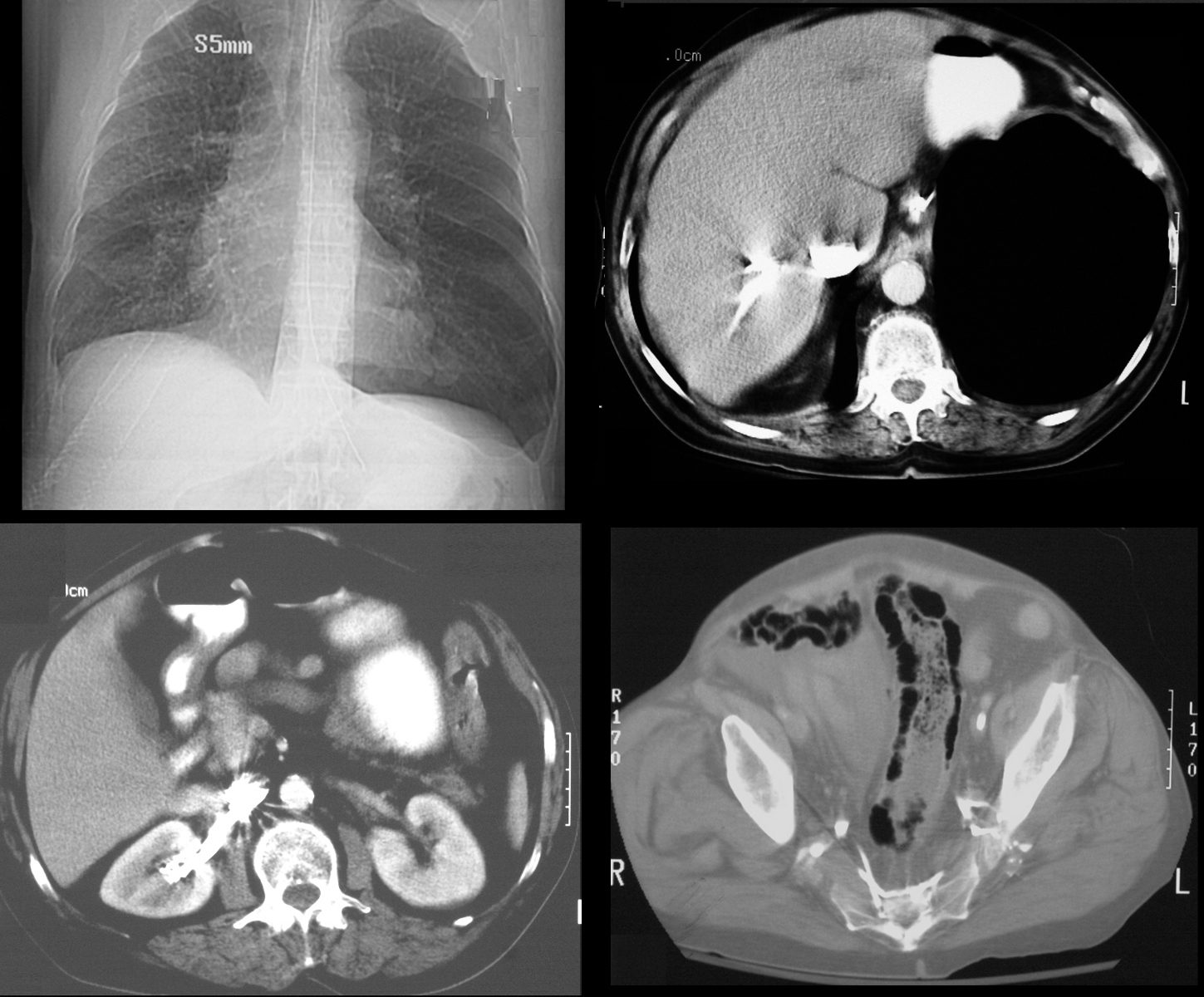
65 year old male s/p MVA presents in shock. Scout film (top left) shows left sided tension pneumothorax with rightward mediastinal shift. Axial CT through the liver (top right) shows expanded pneumothorax at the left lung base with reflux of contrast into the IVC.. Contrast also refluxes into the right renal vein (bottom left) and into the internal iliac veins (bottom right) Associated pneumatosis intestinalis in the sigmoid colon is present as well and likely secondary to the tension pneumothorax
Ashley Davidoff MD TheCommonVein.net
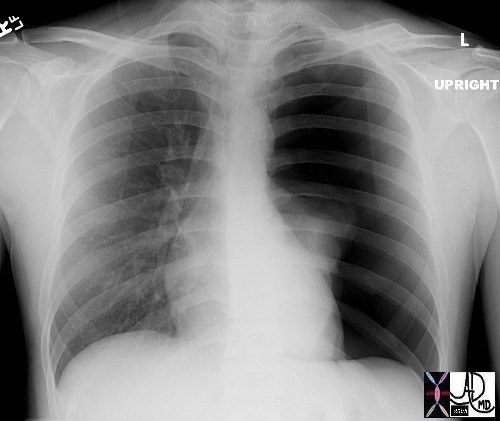
CXR Pseudo-pneumothorax
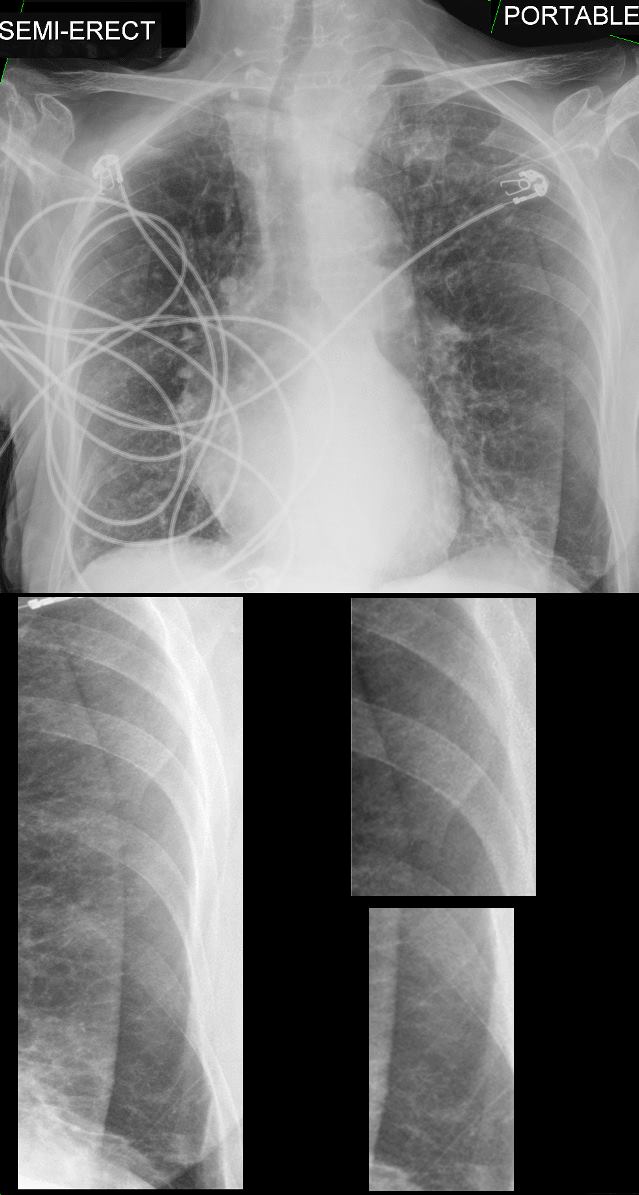
92-year-old female presents with dyspnea. Portable CXR in the frontal projection shows a well- defined line on the lateral aspect of the left lung masquerading as a pleural line and pneumothorax. Closer and magnified evaluation (lower panel images) shows lung markings projecting beyond the sharp line
These findings are consistent with a diagnosis of pseudo-pneumothorax caused by a skin fold
Ashley Davidoff MD TheCommonVein.net 135864c
Tension Pneumothorax
This is the type of CXR that sends shivers down the spine. The overall blackness of the left chest cavity, in association with a nubbin of lung tissue in the ipsilateral hilum and rightward mediastinal shift is characteristic of a tension pneumothorax with total atelectasis of the left lung. Immediate and urgent decompression with a chest drain is indicated.
Courtesy of: Ashley Davidoff, M.D.
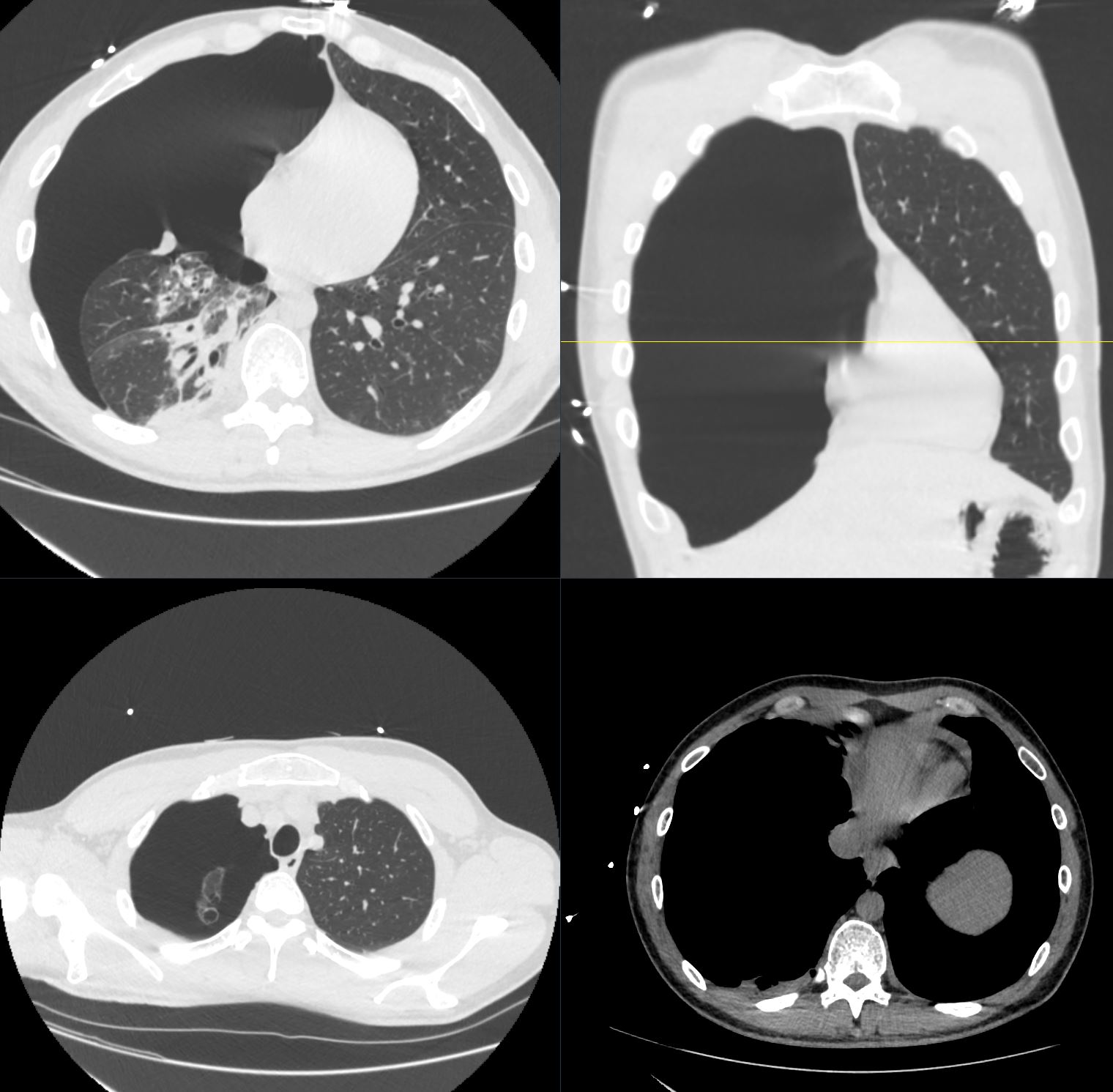
CT scan in the axial and coronal planes show a right sided tension pneumothorax caused by the rupture of an apical bulla. There is total atelectasis of the right lung compression of the right sided heart structures and leftward shift of the mediastinal structures
Ashley Davidoff MD TheCommonVein.net b11585